Request Demo
Last update 11 Jul 2026
Semaglutide (Thery Pharmaceutical)
Last update 11 Jul 2026
Overview
Basic Info
Drug Type Recombinant polypeptide |
Synonyms- |
Target |
Action agonists |
Mechanism GLP-1R agonists(Glucagon-like peptide 1 receptor agonists) |
Therapeutic Areas |
Active Indication |
Inactive Indication- |
Originator Organization |
Active Organization |
Inactive Organization- |
License Organization- |
Drug Highest PhasePhase 3 |
First Approval Date- |
Regulation- |
Login to view timeline
Related
3
Clinical Trials associated with Semaglutide (Thery Pharmaceutical)CTR20244777
司美格鲁肽注射液治疗中国肥胖人群的多中心、随机、开放、平行、阳性药物对照的 Ⅲ 期临床研究
[Translation] A multicenter, randomized, open, parallel, positive drug-controlled phase III clinical study of semaglutide injection in the treatment of obese people in China
CTR20243970
司美格鲁肽注射液在健康成人受试者中的药代动力学特征比较的随机、开放、平行入组的I期临床研究
[Translation] A randomized, open-label, parallel-group phase I clinical study comparing the pharmacokinetic characteristics of semaglutide injection in healthy adult subjects
CTR20241707
司美格鲁肽注射液在健康成人受试者中的药代动力学特征比较的随机、开放、平行入组的I期临床研究
[Translation] A randomized, open, parallel-group phase I clinical study comparing the pharmacokinetic characteristics of semaglutide injection in healthy adult subjects
100 Clinical Results associated with Semaglutide (Thery Pharmaceutical)
Login to view more data
100 Translational Medicine associated with Semaglutide (Thery Pharmaceutical)
Login to view more data
100 Patents (Medical) associated with Semaglutide (Thery Pharmaceutical)
Login to view more data
12
Literatures (Medical) associated with Semaglutide (Thery Pharmaceutical)01 Apr 2026Cancer Prevention Research
Appetite, Obesity, Metabolism, and Malignancy: Do Incretin-Mimetic Drugs Reduce Cancer Risk?
Review
Author: Renehan, Andrew G. ; Pollak, Michael N.
Abstract:
Obesity is associated with increased risk of at least 13 adult cancer types and is the second most common cause of cancer (after tobacco) in many populations. Uncertainty about the extent to which intentional weight loss leads to reduced cancer risk represents a gap in knowledge. Evidence from bariatric surgery studies shows that sustained weight reduction of 20% to 30% in individuals with severe obesity is associated with reduced risk of obesity-related cancers over 10 years. However, in terms of population health, this is not a viable cancer prevention strategy. Recently, glucagon-like peptide-1 receptor agonists (GLP-1RA), known to be effective antidiabetes drugs, have been shown in randomized trials to cause substantial weight loss (in the order of 15%) in obese individuals with or without diabetes. This is a rapidly evolving field, which has revolutionized the modern management of obesity. Much clinical experience has been with semaglutide (a GLP-1RA) and tirzepatide (a dual agonist of the GLP-1 receptor and the glucose-dependent insulinotropic polypeptide receptor), but newer drugs in the class are being developed. We review available data that provide a strong rationale for evaluating incretin-mimetic drugs in a cancer prevention trial but show that the feasibility of such a trial is questionable.
01 Feb 2026ALIMENTARY PHARMACOLOGY & THERAPEUTICS
Exploration of Multiple Non‐Invasive Tests for Assessing Response to Treatment in a Semaglutide Phase 2b Trial in Patients with
MASH
Article
Author: Wong, Vincent Wai‐Sun ; Anstee, Quentin M. ; Fleckner, Jan ; Skalshøi Kjær, Mette ; Nitze, Louise Maymann ; Sanyal, Arun J. ; Krarup, Niels ; Balendran, Clare ; Ratziu, Vlad
ABSTRACT:
Background:
Non‐invasive tests (NITs) are not currently approved as biomarkers of treatment response for patients with metabolic dysfunction‐associated steatohepatitis (MASH).
Aim:
This retrospective study explored a panel of NITs for assessing response to semaglutide treatment in patients with MASH randomised in a phase 2b trial (NCT02970942).
Methods:
The present study was performed using the completer population (268 patients), defined as all patients who were randomised, remained on treatment throughout the trial, and had liver biopsy and NIT results at baseline and week 72. Semaglutide treatment arms were analysed as one semaglutide pooled group. Multiple NITs (alanine transaminase, aspartate transaminase [AST], controlled attenuation parameter, CK18‐M30/M65, SomaSignal nonalcoholic steatohepatitis tests, FibroScan‐AST, NIS‐4, metabolomics advanced steatohepatitis fibrosis score, fibrosis‐4 index, liver stiffness measure [LSM], enhanced liver fibrosis [ELF], PRO‐C3 and ADAPT) were assessed. Treatment response was evaluated by NITs using either mean changes, responder groups, or risk categories from baseline to week 72.
Results:
Semaglutide treatment led to significant reductions versus placebo in all NIT scores from as early as 28 weeks. More patients had MASH improvement and fewer had fibrosis progression versus placebo when assessed by a 20% NIT response (0.5 U for ELF); among patients with baseline LSM > 8 kPa and ELF > 9.8 U, a larger proportion achieved LSM < 8 kPa and ELF < 9.8 kPa with semaglutide versus placebo.
Conclusion:
NITs may be used for assessing a treatment response in patients with MASH. Further studies should confirm the treatment effect of NITs and evaluate the association of NIT changes to outcomes.
01 Jan 2026HEPATOLOGY
Comparative efficacy of pharmacologic therapies for MASH in reducing liver fat content: Systematic review and network meta-analysis
Review
Author: Nah, Benjamin ; Seko, Yuya ; Ramadoss, Vijay ; Noureddin, Mazen ; Takahashi, Hirokazu ; Ng, Cheng Han ; Xiao, Jieling ; Nakajima, Atsushi ; Koh, Benjamin ; Sim, Benedix Kuan Loon ; Teng, Margaret ; Huang, Daniel Q. ; Danpanichkul, Pojsakorn ; Teo, Chong Boon ; Gunalan, Shyna Zhuoying ; Lim, Mei Chin ; Muthiah, Mark ; Law, Michelle ; Wijarnpreecha, Karn ; Loomba, Rohit ; Tan, En Ying
Background and Aims::
Metabolic dysfunction–associated steatohepatitis (MASH) is a leading cause of liver disease. Dynamic changes in MRI proton-density-fat fraction (PDFF) are associated with MASH resolution. We aimed to determine the relative efficacy of therapeutic agents for reducing hepatic fat, assessed by MRI-PDFF.
Approach and Results::
In this systematic review and network meta-analysis, we searched MEDLINE and Embase from inception until December 26, 2023, for published randomized controlled trials comparing pharmacological interventions in patients with MASH that assessed changes in MRI-PDFF. The
primary outcome
was the absolute change in MRI-PDFF. The secondary outcome was a ≥30% decline in MRI-PDFF. A surface under-the-curve cumulative ranking probabilities (SUCRA) analysis was performed. Of 1550 records, a total of 39 randomized controlled trials (3311 participants) met the inclusion criteria. For MRI-PDFF decline at 24 weeks, aldafermin (SUCRA: 83.65), pegozafermin (SUCRA: 83.46), and pioglitazone (SUCRA: 71.67) were ranked the most effective interventions. At 24 weeks, efinopegdutide (SUCRA: 67.02), semaglutide + firsocostat (SUCRA: 62.43), and pegbelfermin (SUCRA: 61.68) were ranked the most effective interventions for achieving a ≥30% decline in MRI-PDFF.
Conclusions::
This study provides an updated, relative rank-order efficacy of therapies for MASH in reducing hepatic fat. These data may help inform the design and sample size calculation of future clinical trials and assist in the selection of combination therapy.
44
News (Medical) associated with Semaglutide (Thery Pharmaceutical)
09 Jul 2026
AcquisitionPatent Infringement
100 Deals associated with Semaglutide (Thery Pharmaceutical)
Login to view more data
External Link
| KEGG | Wiki | ATC | Drug Bank |
|---|---|---|---|
| - | - | - |
R&D Status
10 top R&D records. to view more data
Login
| Indication | Highest Phase | Country/Location | Organization | Date |
|---|---|---|---|---|
| Obesity | Phase 3 | China | 26 Mar 2025 |
Login to view more data
Clinical Result
Clinical Result
Indication
Phase
Evaluation
View All Results
Login to view more data
Translational Medicine
Boost your research with our translational medicine data.
login
or

Deal
Boost your decision using our deal data.
login
or

Core Patent
Boost your research with our Core Patent data.
login
or

Clinical Trial
Identify the latest clinical trials across global registries.
login
or

Approval
Accelerate your research with the latest regulatory approval information.
login
or

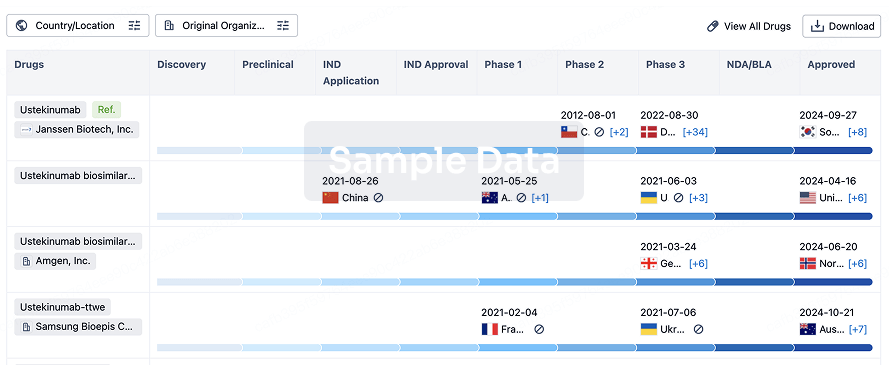
Biosimilar
Competitive landscape of biosimilars in different countries/locations. Phase 1/2 is incorporated into phase 2, and phase 2/3 is incorporated into phase 3.
login
or
Regulation
Understand key drug designations in just a few clicks with Synapse.
login
or

AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free