Request Demo
Last update 30 Sep 2025
Valziflocept
Last update 30 Sep 2025
Overview
Basic Info
Drug Type Recombinant protein |
Synonyms FcγRIIb, Human soluble Fc-gamma receptor IIb, Valziflocept (USAN) + [5] |
Target |
Action antagonists |
Mechanism CD32B antagonists(Low affinity immunoglobulin gamma Fc region receptor II-b antagonists) |
Active Indication- |
Inactive Indication |
Originator Organization |
Active Organization- |
Inactive Organization |
License Organization- |
Drug Highest PhaseDiscontinuedPhase 2 |
First Approval Date- |
Regulation- |



Login to view timeline
Structure/Sequence
Sequence Code 9555778
Source: *****
Related
5
Clinical Trials associated with ValzifloceptPER-050-16
A Phase 2b, Multidose, Multicenter, Double-blind, Placebocontrolled, 24 Week Study to Evaluate the Efficacy and Safety of Intravenous Infusion with Recombinant Human Soluble Fc-gamma IIB Receptor SM101 in Subjects with Systemic Lupus Erythematosus (SLE)
NCT02605525
A Phase 2 Study to Assess the Efficacy and Safety of Intravenous Infusion With Human Soluble Recombinant Fc-gamma Receptor IIB (SM101/BAX 1810) in Subjects With Immunoglobulin A Nephropathy (IgAN)
EUCTR2010-023396-25-BE
Phase IIa, 2:2:1 randomised, double-blind, placebo-controlled,parallel group, multi-centre clinical trial toinvestigate the safety, efficacy and pharmacokinetics ofrecombinant human soluble Fc-gamma receptor IIb(SM101) for intravenous application in the treatment ofsystemic lupus erythematosus (SLE) patients with orwithout a history of lupus nephritis - SMILE
100 Clinical Results associated with Valziflocept
Login to view more data
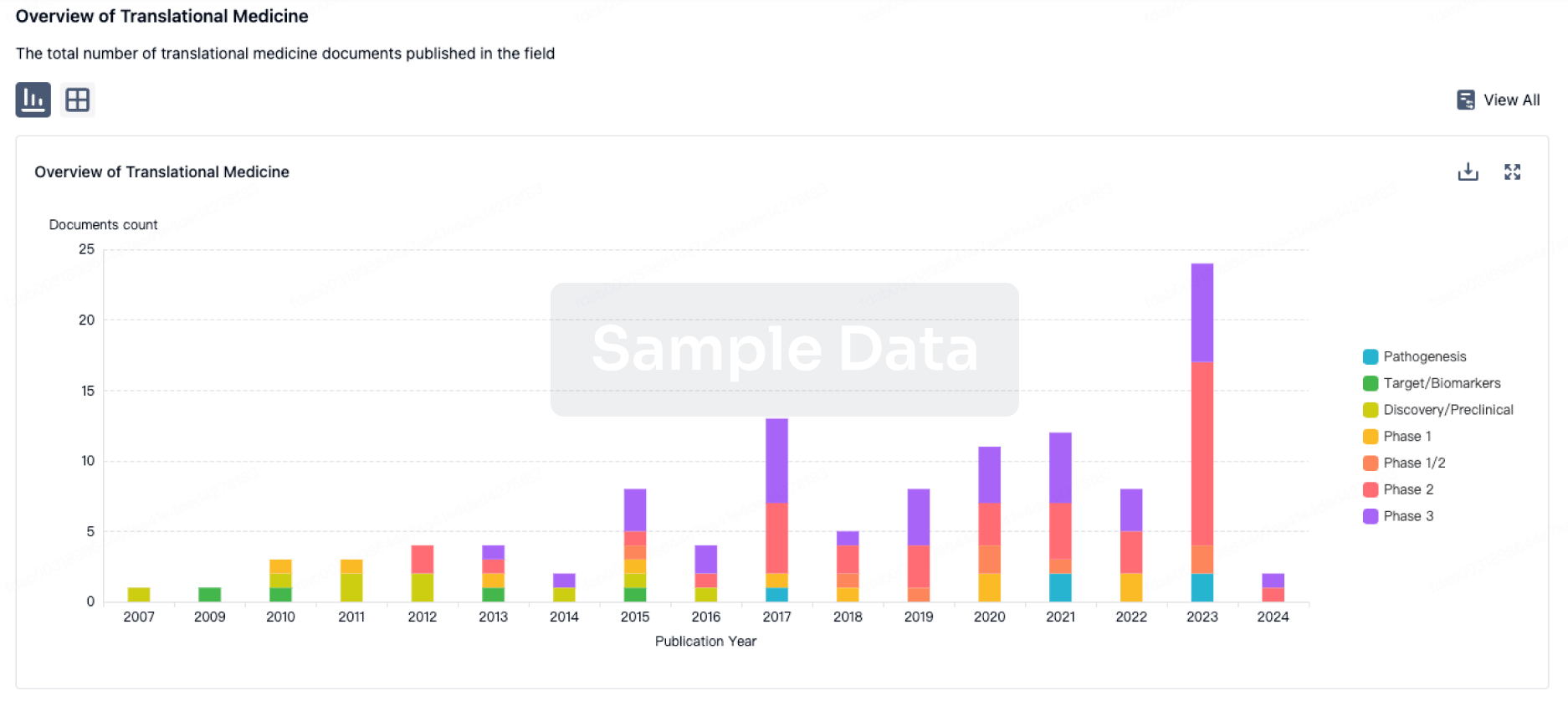
100 Translational Medicine associated with Valziflocept
Login to view more data
100 Patents (Medical) associated with Valziflocept
Login to view more data
8
Literatures (Medical) associated with Valziflocept15 Apr 2020Avian diseasesQ4 · AGRICULTURAL & FORESTRY SCIENCE
Comparison of the Pathogenicity of Five Clostridium perfringens Isolates Using an Eimeria maxima Coinfection Necrotic Enteritis Disease Model in Commercial Broiler Chickens
Q4 · AGRICULTURAL & FORESTRY SCIENCE
Article
Author: Wang, Yunfei ; Liu, Liheng ; Lillehoj, Hyun ; Zhao, Hongyan ; Lu, Mingmin ; Lee, Youngsub ; Melville, Stephen ; Sun, Zhifeng ; Xianyu, Zhezi ; Li, Charles ; Gu, Changqin ; Yan, Xianghe
Clostridium perfringens (CP) is the etiologic agent of necrotic enteritis (NE) in broiler chickens that is responsible for massive economic losses in the poultry industry in response to voluntary reduction and withdrawal of antibiotic growth promoters. Large variations exist in the CP isolates in inducing intestinal NE lesions. However, limited information is available on CP isolate genetics in inducing NE with other predisposing factors. This study investigated the ability of five CP isolates from different sources to influence NE pathogenesis by using an Eimeria maxima (EM) coinfection NE model: Str.13 (from soil), LLY_N11 (healthy chicken intestine), SM101 (food poisoning), Del1 (netB+tpeL-) and LLY_Tpel17 (netB+tpeL+) for NE-afflicted chickens. The 2-wk-old broiler chickens were preinfected with EM (5 × 103 oocysts) followed by CP infection (around 1 × 109 colony-forming units per chicken). The group of the LLY_Tpel17 isolate with EM coinfection had 25% mortality. No mortality was observed in the groups infected with EM alone, all CP alone, or dual infections of EM/other CP isolates. In this model of EM/CP coinfections, the relative percentages of body weight gain showed statistically significant decreases in all EM/CP groups except the EM/SM101 group when compared with the sham control group. Evident gut lesions were only observed in the three groups of EM/LLY_N11, EM/Del1, and EM/LLY_Tpel17, all of which possessed an essential NE pathogenesis locus in their genomes. Our studies indicate that LLY_Tpel17 is highly pathogenic to induce severe gut lesions and would be a good CP challenge strain for studies investigating pathogenesis and evaluating the protection efficacy for antibiotic alternative approaches.
01 May 2016Journal of clinical immunologyQ2 · MEDICINE
The FcγR/IgG Interaction as Target for the Treatment of Autoimmune Diseases
Q2 · MEDICINE
Review
Author: Sondermann, Peter
FcγRs are a crucial component of the antibody response as they mediate the cellular effector functions in response to IgG-containing immune complexes (ICs). Therefore, they also play a central role in the pathogenesis of autoimmune diseases which offers an attractive option to specifically target this class of molecules and their interaction with IgG for treatment of immune disorders. In detail, two strategies are discussed in this article. SM101, a soluble FcγR that is already in clinical development competes with the interaction of IgG with membrane FcγRs. Oppositely, SM201 recruits the inhibitory FcγRIIB for a broad down-modulation of the immune system. The presented approaches for the treatment of autoimmune diseases have the potential be more efficacious with fewer side effects than the currently used therapeutic options.
01 Mar 2015The Journal of investigative dermatologyQ1 · MEDICINE
Recombinant Soluble CD32 Suppresses Disease Progression in Experimental Epidermolysis Bullosa Acquisita
Q1 · MEDICINE
Letter
Author: Zillikens, Detlef ; Möckel, Nicole ; Vorobyev, Artem ; Pipi, Elena ; Sondermann, Peter ; van Beek, Nina ; Ludwig, Ralf J ; Iwata, Hiroaki
TO THE EDITOR: Epidermolysis bullosa acquisita (EBA) is a prototypic organ-specific autoimmune disease, which is characterized by chronic mucocutaneous subepidermal blistering (Gupta et al., 2012; Schmidt and Zillikens, 2013).The autoimmune response is directed against a 290-kDa protein located at the dermal-epidermal junction (DEJ), which has been identified as the type VII collagen (Woodley et al., 1988).Despite major achievements in the understanding of EBA pathogenesis (Gupta et al., 2012), therapy of EBA patients remains difficult, and, because of the low incidence of the disease, data from clin. trials are still missing.Most commonly corticosteroids in combination with other (immunosuppressive) drugs are used (Engineer and Ahmed, 2001), which is associated with severe and potentially life-threatening adverse reactions.Therefore, there is a great and so far unmet medical need for effective and safe treatment options in EBA.We have recently established a mouse model of EBA induced by immunization with an immunodominant domain located within the non-collagenous 1 domain of murine type VII collagen (Iwata et al., 2013).Induction of skin blistering in exptl. EBA depends on the expression of activating Fc gamma receptor (FcγR; Kasperkiewicz et al., 2012).The detrimental contribution of FcγR binding to tissue-deposited immune complexes (ICs) has been well documented in models of autoantibody-mediated diseases, such as rheumatoid arthritis (Kleinau et al., 2000), immune-mediated thrombocytopenia (McKenzie et al., 1999), and autoimmune bullous dermatoses (Ludwig et al., 2013).On the basis of these findings, FcγR seems to be a promising therapeutic target for the treatment of autoantibody-mediated inflammatory diseases.Currently, several novel compounds targeting the interaction of ICs with FcγR are pursued either in preclin. model systems or in clin. trials.Notably, pharmacol. modifications of IgG glycosylation at the Fc fragment, which alters IgG's affinity to FcγR, have prophylactic and therapeutic effects in several models of autoimmunity (Collin and Ehlers, 2013).Other potentially promising FcγR targeting strategies, such as competitive binding of ICs by recombinant soluble FcγR2B (soluble CD32, sCD32, and SM101) in idiopathic thrombocytopenia or systemic lupus erythematosus, are already evaluated in phase I/II clin. trials (http://www.controlled-trials.com/isrctn/search.htmlsrch=SM101).Here, we evaluated whether treatment with sCD32 has therapeutic effects in exptl. EBA. sCD32 binds to IC and thereby blocks the binding of FcγR expressed on the surface of immune cells.Eventually, effector cells cannot be activated via FcγR (Ierino et al., 1993).First, we investigated the effect of sCD32 on activating FcγR-dependent reactive oxygen species (ROS) release from IC-activated neutrophils (Supplementary Materials and Methods online). sCD32 inhibited IC-induced neutrophil ROS production in a dose-dependent manner (Figure 1a).In detail, compared with pos. control, 0.01, 0.1, and 0.5 mg ml-1 sCD32 significantly reduced ROS production by 30, 65, and 75%, resp.Next, we tested whether sCD32 could hinder dermal-epidermal separation in an ex vivo model of autoimmune bullous dermatoses.Accordingly, in the presence of leukocytes, sCD32 successfully impaired FcγR-dependent dermal-epidermal separation on cryosections of human skin incubated with sera containing pathogenic antibodies against DEJ structures (Figure 1b and c; Supplementary Materials and Methods online).To validate this ex vivo inhibitory activity of sCD32 on antibody-induced tissue injury in vivo, we next induced exptl. EBA in mice by immunization with vWFA2 (Supplementary Materials and Methods online).After immunization, mice were allocated to sCD32 or phosphate-buffered saline (PBS) treatment if individual mice had 2% or more of their body-surface area affected by skin lesions (Supplementary Materials and Methods online).Compared with PBS-injected mice, sCD32 treatment led to a significantly lower clin. disease severity (Figure 2a, left, *P<0.05, t-test).At inclusion to treatment (week 0), average disease scores were not different between the groups (3.4±0.21% and 3.4±0.20%) of affected body-surface area in PBS and sCD32 treatment, resp.Cumulative disease severity expressed as area under the curve during the entire observation period was also significantly lower in sCD32-treated mice as compared with PBS control mice (Figure 2a, right, P=0.031, t-test).At the end of the 4-wk treatment period, PBS-treated mice showed diffuse erythema and crusts on the ear and tail, and hair loss around the eyes (Figure 2b, left).In contrast, less erythema on the ear and no disease on tail or around the eyes in mice treated with sCD32 were observed (Figure 2b, right).Histol., mice treated with sCD32 showed a significant decrease in the dermal leukocyte infiltration, compared with PBS-treated mice (P<0.05, Figure 2c). sCD32 treatment also led to an ∼20% reduction in circulating antigen-specific autoantibodies compared with PBS-treated mice (Figures 2d, P=0.048; t-test), whereas total IgG levels were not significantly different (data not shown).At the same time point, all mice showed similar IgG deposits at DEJ as determined by direct immunofluorescence (Figure 2e, upper).Representative pictures of direct immunofluorescence show IgG deposits at DEJ (Figure 2e, down).This discrepancy between circulating and tissue bound autoantibodies may be because of their different half-lives. sCD32 treatment has also demonstrated beneficial effects in models of other autoantibody-mediated diseases, such as nephritis in lupus-prone NZB/NZW F(1) hybrid mice (Werwitzke et al., 2008) and joint inflammation in collagen-induced arthritis (Magnusson et al., 2008).On the basis of our observations ex vivo and in vivo, the therapeutic effect of sCD32 can be attributed to both direct and indirect mechanisms, which mean the inhibition of neutrophil function and autoantibody production, resp.On the basis of our observation of therapeutic efficacy in exptl. EBA, it is tempting to speculate that sCD32 binds to the in situ deposited ICs.This assumption, however, needs further exptl. exploration.Regarding the effect on autoantibody production, controversial results have been reported.In the lupus-prone NZM/NZW mouse model neither prophylactic nor therapeutic treatment with sCD32 affected anti-double stranded DNA serum titers (Werwitzke et al., 2008).In contrast, sCD32 suppressed secondary and primary in vitro antibody responses (Varin et al., 1989) and caused a temporary decrease in collagen-specific autoantibodies in CIA (Magnusson et al., 2008).In support of these later observations, we here report a sustained reduction of antigen-specific but not of total circulating IgG in immunization-induced EBA.This effect may be mediated through a blockade of the IgG2a-mediated enhancement of antibody and T-cell responses via increased antigen presentation to CD4+ T cells by FcγR-expressing antigen-presenting cells (Getahun et al., 2004).Taken together, our findings provide evidence for a beneficial role of sCD32 in exptl. EBA.As this model mostly reflects the inflammatory variant of EBA, our findings may pave the way for its clin. application in patients with autoimmune bullous dermatoses, where disease manifestation depends on an interaction of ICs with effector myeloid cells.
3
News (Medical) associated with Valziflocept12 Aug 2025
Phase 2Phase 3Financial StatementImmunotherapyClinical Result
15 May 2025
Phase 2Phase 3Financial StatementExecutive ChangePhase 1
19 Jan 2022
CollaborateAntibodyOrphan DrugFirst in ClassImmunotherapy
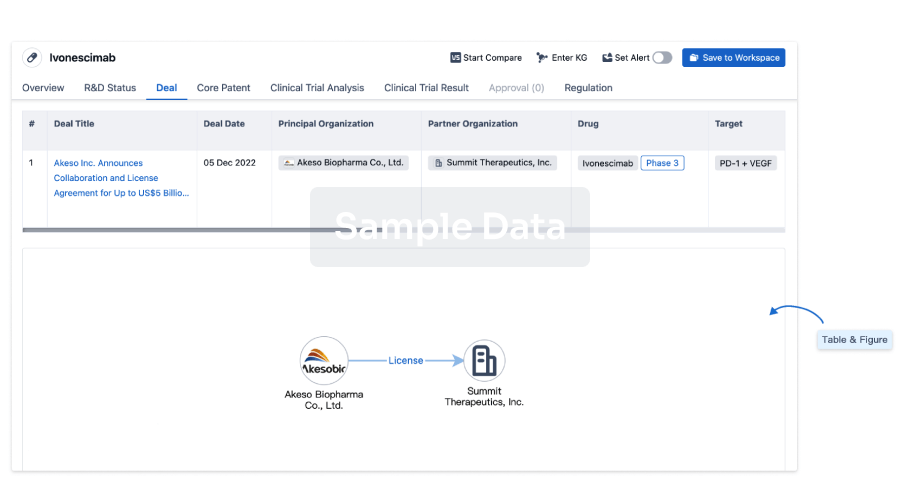
100 Deals associated with Valziflocept
Login to view more data
External Link
| KEGG | Wiki | ATC | Drug Bank |
|---|---|---|---|
| D11339 | - | - | - |
R&D Status
10 top R&D records. to view more data
Login
| Indication | Highest Phase | Country/Location | Organization | Date |
|---|---|---|---|---|
| Glomerulonephritis, IGA | Phase 2 | - | 31 Dec 2015 | |
| Purpura, Thrombocytopenic, Idiopathic | Phase 2 | Belgium | - | |
| Purpura, Thrombocytopenic, Idiopathic | Phase 2 | Germany | - | |
| Purpura, Thrombocytopenic, Idiopathic | Phase 2 | Poland | - | |
| Purpura, Thrombocytopenic, Idiopathic | Phase 2 | Russia | - | |
| Purpura, Thrombocytopenic, Idiopathic | Phase 2 | Ukraine | - |
Login to view more data
Clinical Result
Clinical Result
Indication
Phase
Evaluation
View All Results
Login to view more data
Translational Medicine
Boost your research with our translational medicine data.
login
or
Deal
Boost your decision using our deal data.
login
or
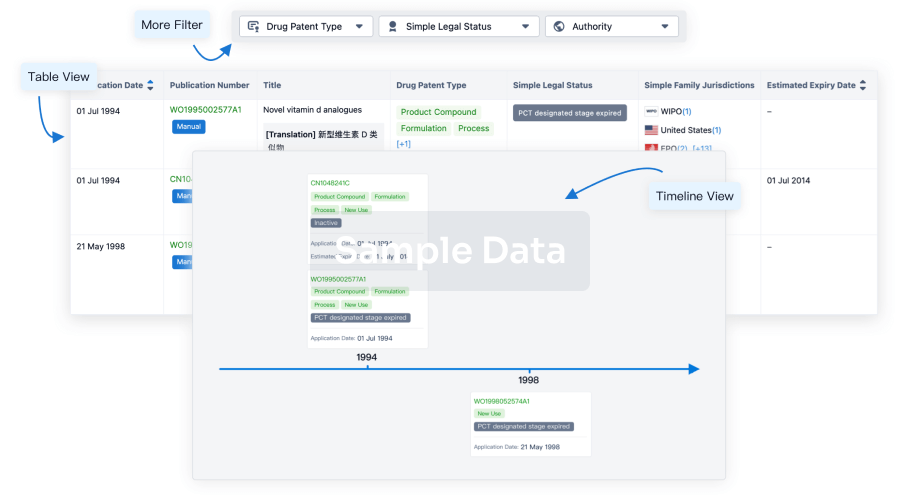
Core Patent
Boost your research with our Core Patent data.
login
or
Clinical Trial
Identify the latest clinical trials across global registries.
login
or
Approval
Accelerate your research with the latest regulatory approval information.
login
or
Biosimilar
Competitive landscape of biosimilars in different countries/locations. Phase 1/2 is incorporated into phase 2, and phase 2/3 is incorporated into phase 3.
login
or
Regulation
Understand key drug designations in just a few clicks with Synapse.
login
or
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free