Request Demo
Last update 04 Dec 2025
PF-06263507
Last update 04 Dec 2025
Overview
Basic Info
Drug Type Antibody drug conjugate (ADC) |
Synonyms A1-MAFODOTIN, Anti-5T4 monoclonal antibody, MMAF ADC + [2] |
Target |
Action modulators, inhibitors |
Mechanism 5T4 modulators(Trophoblast glycoprotein modulators), Tubulin inhibitors |
Therapeutic Areas |
Active Indication- |
Inactive Indication |
Originator Organization |
Active Organization- |
Inactive Organization |
License Organization- |
Drug Highest PhaseDiscontinuedPhase 1 |
First Approval Date- |
Regulation- |


Login to view timeline
Structure/Sequence
Boost your research with our ADC technology data.
login
or
Sequence Code 160833H
Sequence Code 160835L
Related
1
Clinical Trials associated with PF-06263507NCT01891669
A PHASE 1, DOSE ESCALATION STUDY OF PF-06263507 IN PATIENTS WITH ADVANCED SOLID TUMORS
100 Clinical Results associated with PF-06263507
Login to view more data
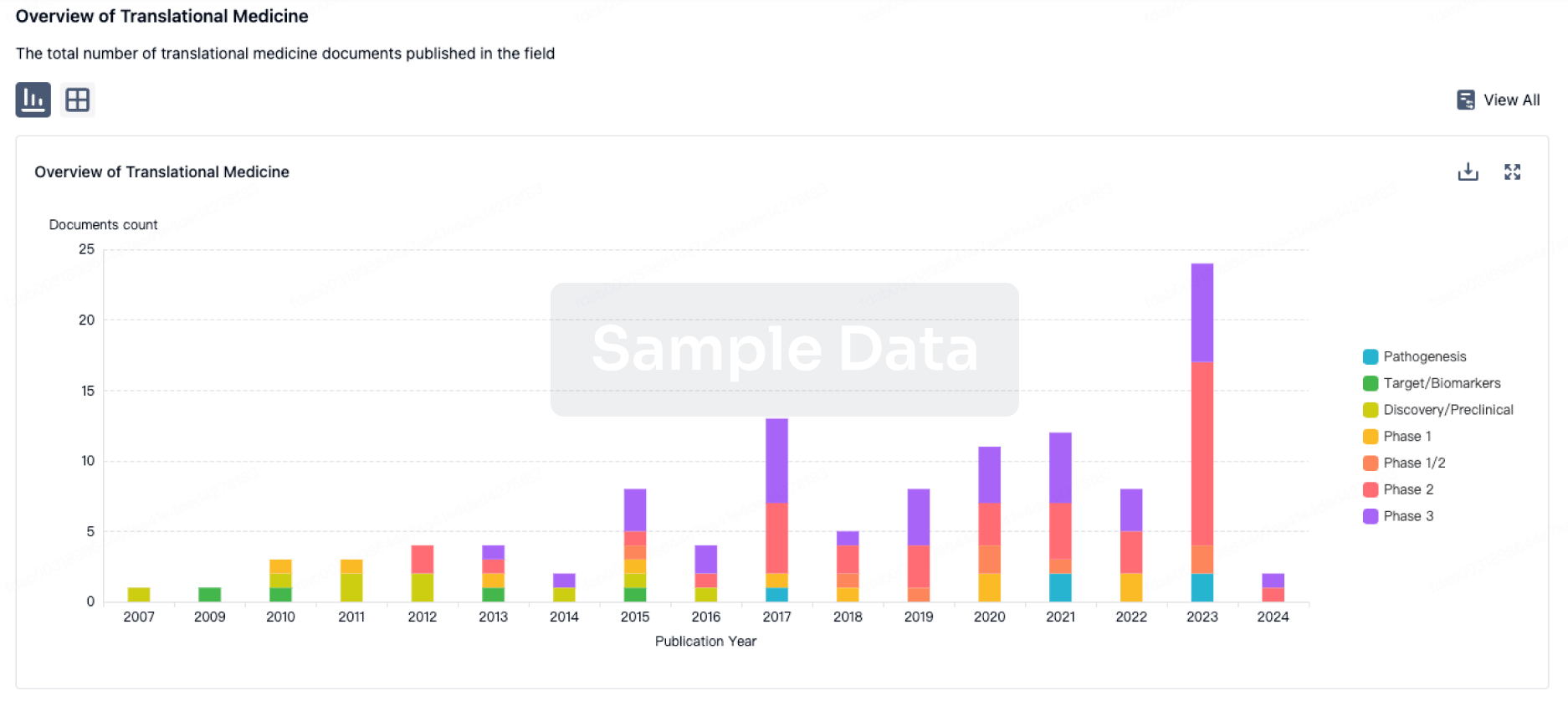
100 Translational Medicine associated with PF-06263507
Login to view more data
100 Patents (Medical) associated with PF-06263507
Login to view more data
109
Literatures (Medical) associated with PF-0626350706 Apr 2023Bioconjugate chemistry
One-Pot Assembly of Dual-Site-Specific Antibody-Drug Conjugates via Glycan Remodeling and Affinity-Directed Traceless Conjugation.
Article
Author: Jiang, Zhong-Xing ; Yao, Xu ; Tang, Feng ; Zeng, Yue ; Tang, Caihong ; Zhang, Jianxin ; Huang, Wei ; Zheng, Xing ; Shi, Wei
The drug-to-antibody ratio (DAR) value and dual-drug combination greatly influence the therapeutic index of antibody-drug conjugates (ADCs). The reported approaches usually require multifunctional branched linkers, a combination of complicated technologies, or protein-protein ligation, which may incorporate multihydrophobic fragments or result in low coupling efficiency. Herein, we developed a facile and efficient one-pot method to assemble dual-site-specific ADCs with defined DARs at both the N-glycosylation site and K248 site, either with the same payloads or with two types of payloads. The constructed dual-site ADCs showed acceptable homogeneity, excellent buffer stability, and enhanced in vitro and in vivo efficiency.
21 Mar 2023Leukemia & lymphoma
Hepatic Veno-occlusive disease (VOD) in multiple myeloma patient receiving Belantamab Mafodotin
Letter
Author: Trajce, Enkeleida ; Danglis, Fotios ; Pessach, Ilias ; Argyrakopoulou, Georgia ; Chandrinou, Eleni ; Rapti, Irene ; Petropoulos, Fotios
This is a case of a 74 yr old man with a history of IgGkappa MM from 2009.He had undergone treatment with Bortezomib-Dexamethasone at diagnosis, which was repeated 6 years afterwards followed by ASCT and Lenalidomide maintenance.Belamaf is a first-in-class humanized IgG1 ADC targeting B-cell maturation antigen (BCMA), covalently linked via a cysteine linker to the microtubule inhibitor monomethyl auristatin F (MMAF), which is released after internalization of the ADC to BCMA on tumor plasma cell, and inhibits its polymerization with the arrest of G2/M caspase dependent apoptosis.The patient received Levofloxacin 12-wk prophylaxis, acyclovir and co-trimoxazole prophylaxis, hydromellose eye drops throughout the treatment period, a coolant eye mask during every Belamaf infusion, and was ophthalmologicaly assessed before each cycle.2 Wk later, patient was urgently re-admitted with consciousness disturbances, weight gain, abdominal pain, defecation incapacity, and significant hyperbilirubinemia (total bilirubin: 6 mg/dL, direct bilirubin: 3 mg/dL, indirect bilirubin: 3 mg/dL).Our patient had never received an Allo-SCT, he had undergone an Autologous SCT many years before the VOD presentation and he had received several lines of treatment without presenting signs of hepatic toxicity.In conclusion, we described a rare case of VOD, histol. proven, in a MM patient on Belamaf-a novel ADC approved for treatment of relapsed or refractory MM.
01 Mar 2023Journal of controlled release : official journal of the Controlled Release Society
Comparison of HER2-targeted affibody conjugates loaded with auristatin- and maytansine-derived drugs
Article
Author: Tretyakova, Maria S ; Tolmachev, Vladimir ; Zhang, Jie ; Belousov, Mikhail V ; Orlova, Anna ; Liu, Yongsheng ; Oroujeni, Maryam ; Yin, Wen ; Gräslund, Torbjörn ; Ding, Haozhong ; Bodenko, Vitalina ; Xu, Tianqi ; Vorobyeva, Anzhelika
Treatment with antibody drug conjugates targeting receptors over-expressed on cancer cells is well established for clinical use in several types of cancer, however, resistance often occurs motivating the development of novel drugs. We have recently investigated a drug conjugate consisting of an affibody molecule targeting the human epidermal growth factor receptor 2 (HER2), fused to an albumin-binding domain (ABD) for half-life extension, loaded with the cytotoxic maytansine derivative DM1. In this study, we investigated the impact of the cytotoxic payload on binding properties, cytotoxicity and biodistribution by comparing DM1 with the auristatins MMAE and MMAF, as part of the drug conjugate. All constructs had specific and high affinity binding to HER2, human and mouse albumins with values in the low- to sub-nM range. ZHER2-ABD-mcMMAF demonstrated the most potent cytotoxic effect on several HER2-over-expressing cell lines. In an experimental therapy study, the MMAF-based conjugate provided complete tumor regression in 50% of BALB/c nu/nu mice bearing HER2-over-expressing SKOV3 tumors at a 2.9 mg/kg dose, while the same dose of ZHER2-ABD-mcDM1 provided only a moderate anti-tumor effect. A comparison with the non-targeting ZTaq-ABD-mcMMAF control demonstrated HER2-targeting specificity. In conclusion, a combination of potent cytotoxicity in vitro, with minimal uptake in normal organs in vivo, and efficient delivery to tumors provided a superior anti-tumor effect of ZHER2-ABD-mcMMAF, while maintaining a favorable toxicity profile with no observed adverse effects.
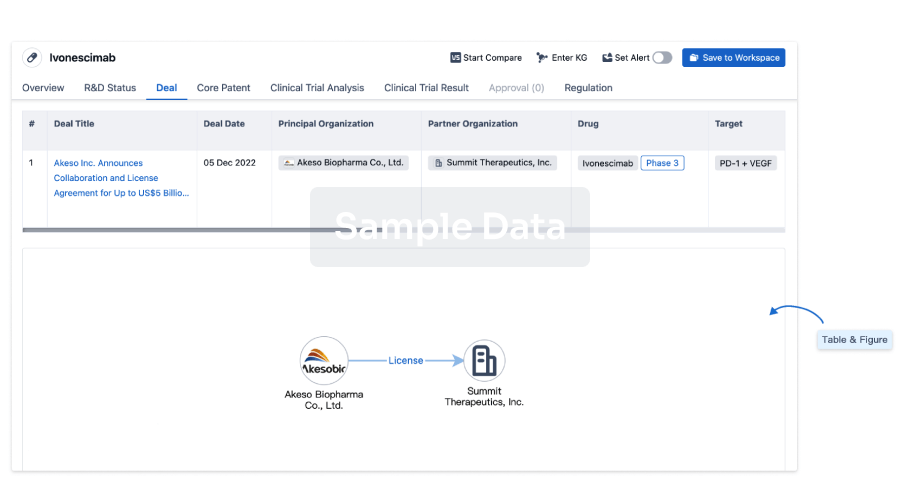
100 Deals associated with PF-06263507
Login to view more data
R&D Status
10 top R&D records. to view more data
Login
| Indication | Highest Phase | Country/Location | Organization | Date |
|---|---|---|---|---|
| Advanced Malignant Solid Neoplasm | Phase 1 | United States | 08 Aug 2013 | |
| Breast Cancer | Phase 1 | United States | 08 Aug 2013 | |
| Non-Small Cell Lung Cancer | Phase 1 | United States | 08 Aug 2013 | |
| Ovarian Cancer | Phase 1 | United States | 08 Aug 2013 |
Login to view more data
Clinical Result
Clinical Result
Indication
Phase
Evaluation
View All Results
Login to view more data
Translational Medicine
Boost your research with our translational medicine data.
login
or
Deal
Boost your decision using our deal data.
login
or
Core Patent
Boost your research with our Core Patent data.
login
or
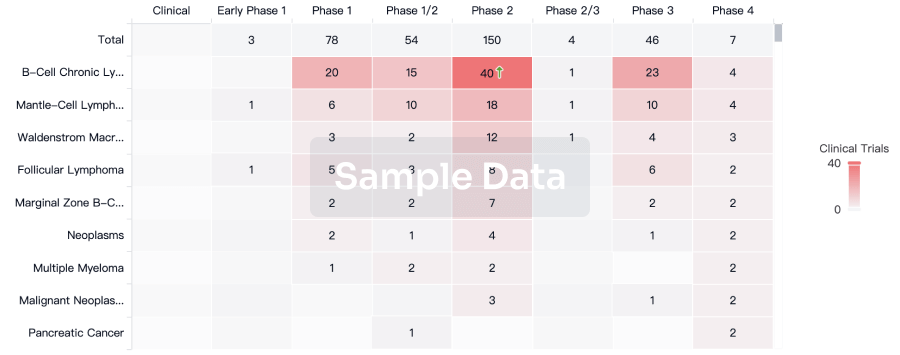
Clinical Trial
Identify the latest clinical trials across global registries.
login
or
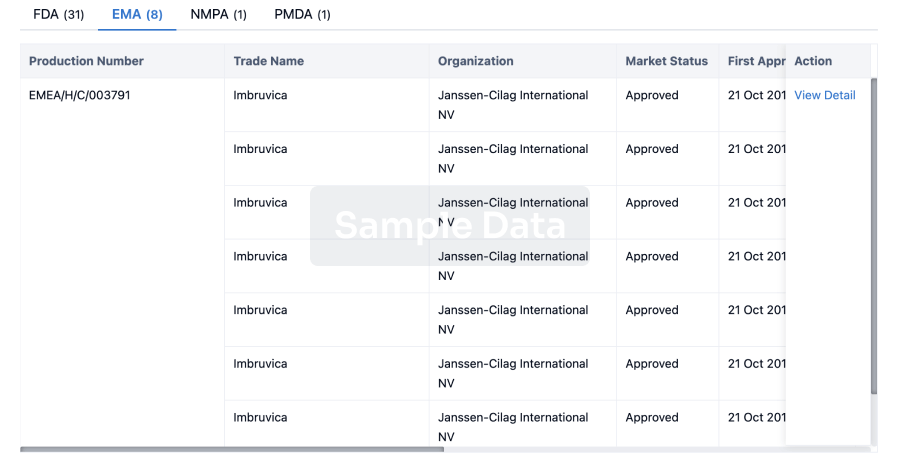
Approval
Accelerate your research with the latest regulatory approval information.
login
or
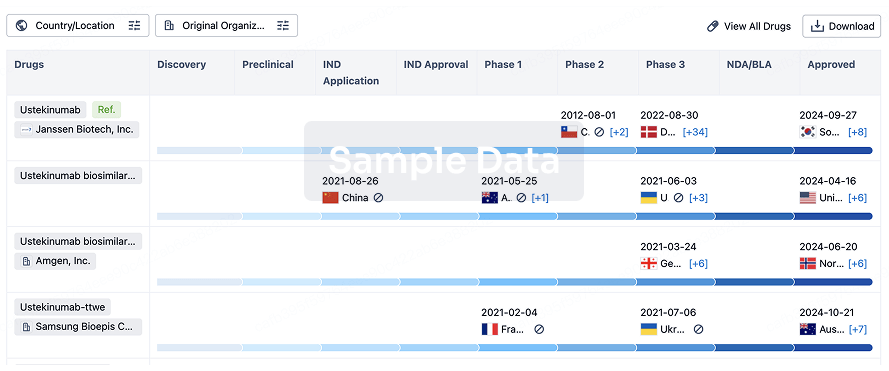
Biosimilar
Competitive landscape of biosimilars in different countries/locations. Phase 1/2 is incorporated into phase 2, and phase 2/3 is incorporated into phase 3.
login
or
Regulation
Understand key drug designations in just a few clicks with Synapse.
login
or
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free