Request Demo
Last update 08 May 2025
Recombinant human nerve growth factor(Jiangsu Zhongxin Medicine Co Ltd)
Last update 08 May 2025
Overview
Basic Info
Drug Type Growth factors |
Synonyms + [1] |
Target |
Action agonists, stimulants |
Mechanism p75NTR agonists(Low affinity neurotrophin receptor p75NTR agonists), Neurons stimulants |
Therapeutic Areas |
Active Indication |
Inactive Indication- |
Originator Organization |
Active Organization |
Inactive Organization |
License Organization |
Drug Highest PhasePhase 2 |
First Approval Date- |
RegulationSpecial Review Project (China) |
Login to view timeline
Related
5
Clinical Trials associated with Recombinant human nerve growth factor(Jiangsu Zhongxin Medicine Co Ltd)CTR20242836
重组人神经生长因子滴眼液在中国健康受试者的安全性、耐受性和药代动力学的随机、双盲、安慰剂对照单次/多次给药I期临床试验
[Translation] A randomized, double-blind, placebo-controlled, single/multiple-dose phase I clinical trial of the safety, tolerability and pharmacokinetics of recombinant human nerve growth factor eye drops in healthy Chinese subjects
CTR20230387
重组人神经生长因子(ZX1305)注射液治疗视神经损伤有效性、安全性和免疫原性的Ⅱ
期临床研究
[Translation] Phase II clinical study on the efficacy, safety and immunogenicity of recombinant human nerve growth factor (ZX1305) injection in the treatment of optic nerve damage
CTR20230957
重组人神经生长因子(ZX1305)注射液治疗开角型青光眼导致的视神经损伤有效性、安全性和免疫原性的II期临床研究
[Translation] Phase II clinical study on the efficacy, safety and immunogenicity of recombinant human nerve growth factor (ZX1305) injection in the treatment of optic nerve damage caused by open-angle glaucoma
100 Clinical Results associated with Recombinant human nerve growth factor(Jiangsu Zhongxin Medicine Co Ltd)
Login to view more data
100 Translational Medicine associated with Recombinant human nerve growth factor(Jiangsu Zhongxin Medicine Co Ltd)
Login to view more data
100 Patents (Medical) associated with Recombinant human nerve growth factor(Jiangsu Zhongxin Medicine Co Ltd)
Login to view more data
5
Literatures (Medical) associated with Recombinant human nerve growth factor(Jiangsu Zhongxin Medicine Co Ltd)01 Aug 2021CorneaQ3 · MEDICINE
Treatment of Dry Eye from Laser-Assisted In Situ Keratomileusis With Recombinant Human Nerve Growth Factor (Cenegermin)
Q3 · MEDICINE
Article
Author: Habibi, Roya N ; Lee, Michele D
01 Jun 2021American Journal of Ophthalmology Case Reports
Neurotrophic keratitis after penetrating keratoplasty for lattice dystrophy
Author: Penatti, Raphael ; Gouvea, Larissa ; Rocha, Karolinne Maia
01 Feb 2019Ophthalmology
Re: Bonini et al.: Phase 2 randomized, double-masked, vehicle-controlled trial of recombinant human nerve growth factor for neurotrophic keratitis (Ophthalmology. 2018;125:1332-1343)
Letter
Author: Ting, Darren Shu Jeng
100 Deals associated with Recombinant human nerve growth factor(Jiangsu Zhongxin Medicine Co Ltd)
Login to view more data
R&D Status
10 top R&D records. to view more data
Login
| Indication | Highest Phase | Country/Location | Organization | Date |
|---|---|---|---|---|
| Neurotrophic keratitis | Phase 2 | China | 23 Apr 2025 | |
| Glaucoma, Open-Angle | Phase 2 | China | 10 May 2023 | |
| Optic Nerve Injuries | Phase 2 | China | 10 May 2023 | |
| Glaucoma | Preclinical | United States | 01 Dec 2016 |
Login to view more data
Clinical Result
Clinical Result
Indication
Phase
Evaluation
View All Results
Login to view more data
Translational Medicine
Boost your research with our translational medicine data.
login
or

Deal
Boost your decision using our deal data.
login
or

Core Patent
Boost your research with our Core Patent data.
login
or

Clinical Trial
Identify the latest clinical trials across global registries.
login
or

Approval
Accelerate your research with the latest regulatory approval information.
login
or

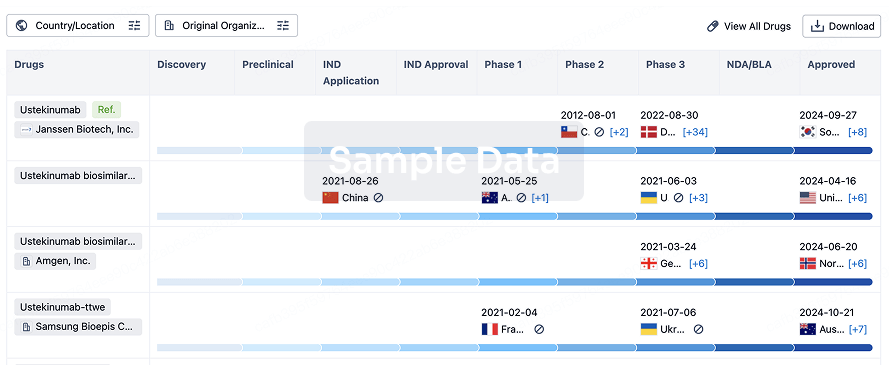
Biosimilar
Competitive landscape of biosimilars in different countries/locations. Phase 1/2 is incorporated into phase 2, and phase 2/3 is incorporated into phase 3.
login
or
Regulation
Understand key drug designations in just a few clicks with Synapse.
login
or

AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free