Request Demo
Last update 06 Dec 2025
Anti-CD19 CART(Anhui Provincial Hospital)
Last update 06 Dec 2025
Overview
Basic Info
Drug Type CAR-T |
Synonyms SWK-002 |
Target |
Action modulators |
Mechanism CD19 modulators(B-lymphocyte antigen CD19 modulators) |
Therapeutic Areas |
Active Indication |
Inactive Indication- |
Originator Organization |
Active Organization |
Inactive Organization- |
License Organization- |
Drug Highest PhaseClinical |
First Approval Date- |
Regulation- |
Related
1
Clinical Trials associated with Anti-CD19 CART(Anhui Provincial Hospital)NCT06503237
Safety and Efficacy of SWK002 in Patients With D2T-Rheumatoid Arthritis
100 Clinical Results associated with Anti-CD19 CART(Anhui Provincial Hospital)
Login to view more data
100 Translational Medicine associated with Anti-CD19 CART(Anhui Provincial Hospital)
Login to view more data
100 Patents (Medical) associated with Anti-CD19 CART(Anhui Provincial Hospital)
Login to view more data
12
Literatures (Medical) associated with Anti-CD19 CART(Anhui Provincial Hospital)01 Dec 2023Molecular therapy. Methods & clinical development
Cytokine and reactivity profiles in SLE patients following anti-CD19 CART therapy
Article
Author: Wong, Steven ; Patel, Darshil ; Müller, Fabian ; Basu, Samik ; Nunez, Daniel ; Volkov, Jenell ; Schett, Georg ; Aigner, Michael ; Mackensen, Andreas ; Vorndran, Zachary ; Völkl, Simon
Chimeric antigen receptor (CAR) T cells targeting CD19+ B cells have demonstrated efficacy in refractory systemic lupus erythematosus (SLE). Although initial clinical data suggest that anti-CD19 CAR T cell therapy is well tolerated and highly effective, the immunologic consequences of CAR T cell therapy in SLE patients remain unclear. We profiled serum in six refractory SLE patients prior to and 3 months following CAR T cell infusion. Three months post T cell infusion, the inflammatory cytokines IL-6 and TNFα decreased in patient sera. This was accompanied by elevations in serum IL-7 and BAFF. Furthermore, SLE-associated antibodies dropped profoundly in five of six patients. Last, consistent with other reports of CD19 CAR T therapy in B cell malignancies, we were able to show marginal impact of anti-CD19 CART therapy on pre-existing humoral immune responses in SLE patients. Together, these results provide insights into the mechanisms of efficacy of anti-CD19 CAR T cell therapy in SLE.
01 Jul 2023British journal of haematology
Early lymphocyte collection for anti‐CD19 CART production improves T‐cell fitness in patients with relapsed/refractory diffuse large B‐cell lymphoma
Article
Author: Asherie, N. ; Assayag, M. ; Gatt, M. E. ; Avni, B. ; Lebel, E. ; Grisariu, S. ; Dubnikov Sharon, T. ; Goldschmidt, N. ; Kfir-Erenfeld, S. ; Stepensky, P.
Summary:
Background:
Chimeric antigen receptor (CAR) T cells targeted to the CD19 B‐cell antigen form an approved treatment for patients with relapsed/refractory diffuse large B‐cell lymphoma (r/r DLBCL). However, since this therapy is administered after multiple lines of treatment and exposure to lymphotoxic agents, there is an urgent need to optimize this modality of treatment.
Methods:
To circumvent the difficulties of harvesting adequate and optimal T cells from DLBCL patients and improve CART therapy, we suggest an earlier lymphopheresis (i.e. at first relapse, before salvage treatment). We conducted a prospective study and evaluated the potential benefit of an earlier lymphopheresis (early group, n = 22) on the clinical outcome of CD19‐CART infused DLBCL patients, in comparison with standard lymphopheresis (i.e. at second relapse and beyond; standard group, n = 23).
Results:
An increased percentage of naïve T cells and increased in vitro T‐cell functionality were observed in the early group. Additionally, these cells exhibit a lower exhaustion profile than T cells collected in the standard group.
Conclusion:
While improved T‐cell phenotype and function in the lymphopheresis product did not translate into significantly improved clinical outcomes, a trend towards better overall survival (OS) and progression‐free survival (PFS) was observed. Early lymphopheresis maximizes the potential of salvage therapies, without compromising CAR T‐cell quality.
01 Jun 2023Bone marrow transplantation
Role of allogeneic hematopoietic cell transplant for relapsed/refractory aggressive B-cell lymphomas in the CART era.
Article
Author: López, Sebastián Garzón ; Pérez-Ortega, Laura ; Albo, Carmen ; Sureda, Anna ; Español, Ignacio ; Bastos-Oreiro, Mariana ; Hernani, Rafael ; Torrent, Anna ; Caballero, Dolores ; Perez, Antonio ; Martínez-Cibrián, Nuria ; Ortí, Guillermo ; Benzaquén, Ana ; Gómez, Juan Montoro ; Campos, António ; Perera, María ; Bailen, Rebeca ; Reguera, Juan Luis ; Yáñez, Lucrecia ; Bento, Leyre ; Echechipia, Izaksun Ceberio ; Rius-Sansalvador, Blanca ; Ferra, Christelle ; Mussetti, Alberto ; Pascual, Maria-Jesús ; López-Godino, Oriana ; Guerra, Luisa Maria ; Sanchez, Jose M ; Corral, Lucía López ; González Sierra, Pedro Antonio ; Iacoboni, Gloria ; Barba, Pere ; Briones, Javier ; Kwon, Mi ; Jiménez-Ubieto, Ana ; Sanz, Jaime ; Varela, Rosario ; Caballero, Ana Carolina ; Ortiz-Maldonado, Valentín ; Munoz, Maria Carmen Martinez
Anti-CD19 chimeric antigen receptor T cells (CART) has rapidly been adopted as the standard third-line therapy to treat aggressive B-cell lymphomas (ABCL) after failure of second-line therapy despite the lack of direct comparisons with allogeneic hematopoietic cell transplantation (alloHCT)-based strategies. Using the Grupo Español de Trasplante y Terapia Celular (GETH-TC) registry, we selected patients with the following characteristics: CART or alloHCT performed between 2016 and 2021; ≥18 years old; ABCL diagnosis; ≥2 lines of therapy; and either anti-CD19 CART or alloHCT as therapy at relapse. The analysis included a total of 316 (CART = 215, alloHCT = 101) patients. Median follow-up was 15 and 36 months for the CART and alloHCT cohorts, respectively. In the multivariate analysis, CART was confirmed to be similar to alloHCT for the primary study endpoint (progression-free survival) (hazard ratio [HR] 0.92, CI95%:0.56-1.51, p = 0.75). Furthermore, when the analysis was limited to only patients with chemo-sensitive diseases (complete and partial response) at infusion (CART = 26, alloHCT=93), no differences were reported (progression-free survival at month +18: 65% versus 55%, p = 0.59). However, CART had lower non-relapse mortality (HR 0.34, 95% CI: 0.13-0.85, p = 0.02). Given the lower toxicity and similar survival outcomes, these results suggest the use of CART before alloHCT.
100 Deals associated with Anti-CD19 CART(Anhui Provincial Hospital)
Login to view more data
R&D Status
10 top R&D records. to view more data
Login
| Indication | Highest Phase | Country/Location | Organization | Date |
|---|---|---|---|---|
| Rheumatoid Arthritis | Clinical | China | 09 Nov 2023 |
Login to view more data
Clinical Result
Clinical Result
Indication
Phase
Evaluation
View All Results
Login to view more data
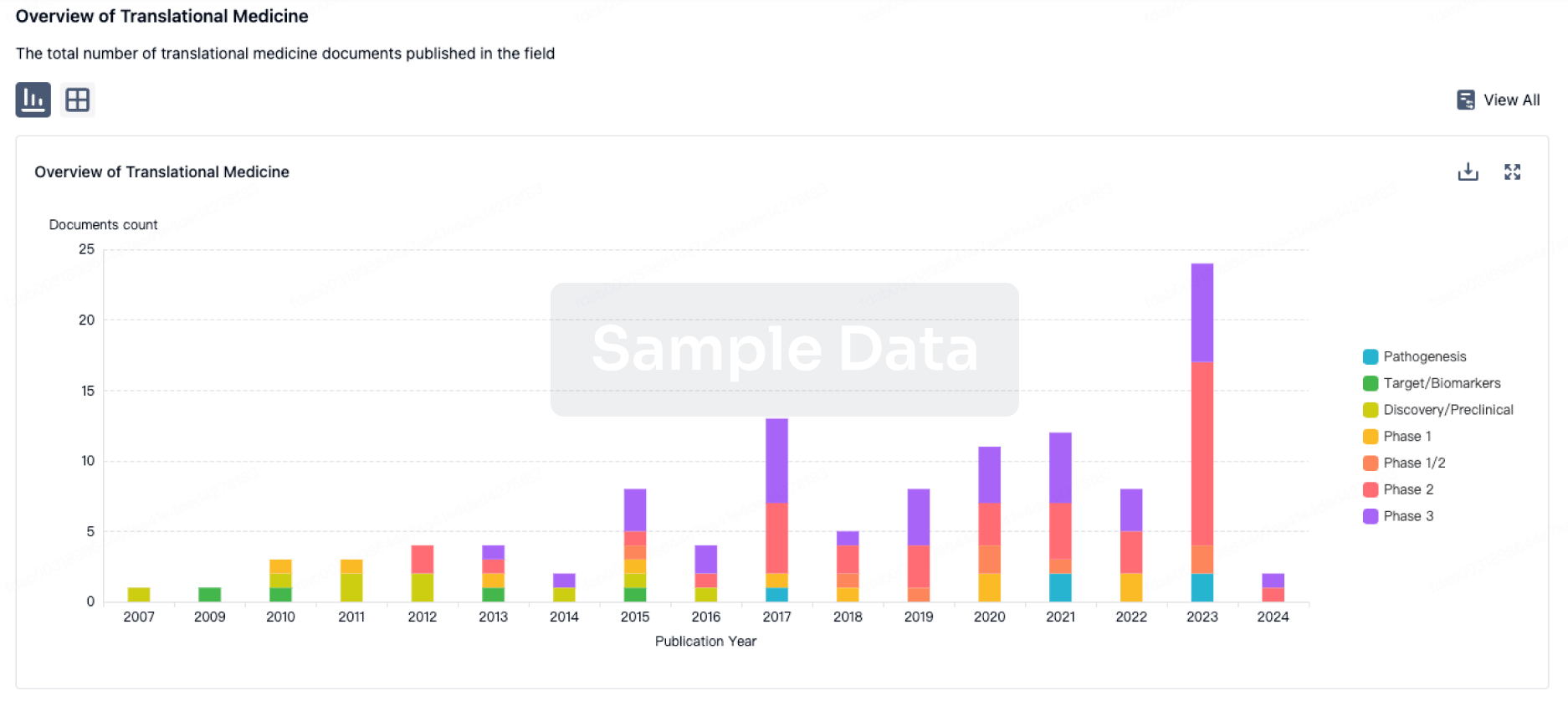
Translational Medicine
Boost your research with our translational medicine data.
login
or
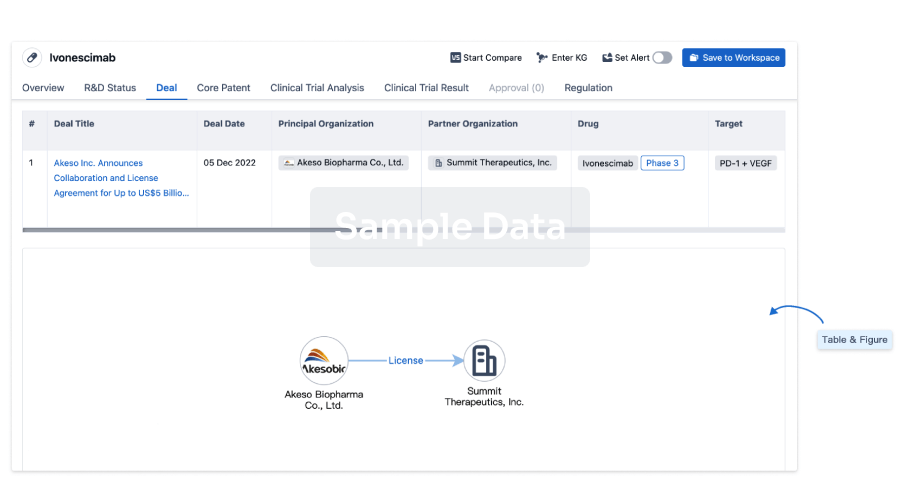
Deal
Boost your decision using our deal data.
login
or
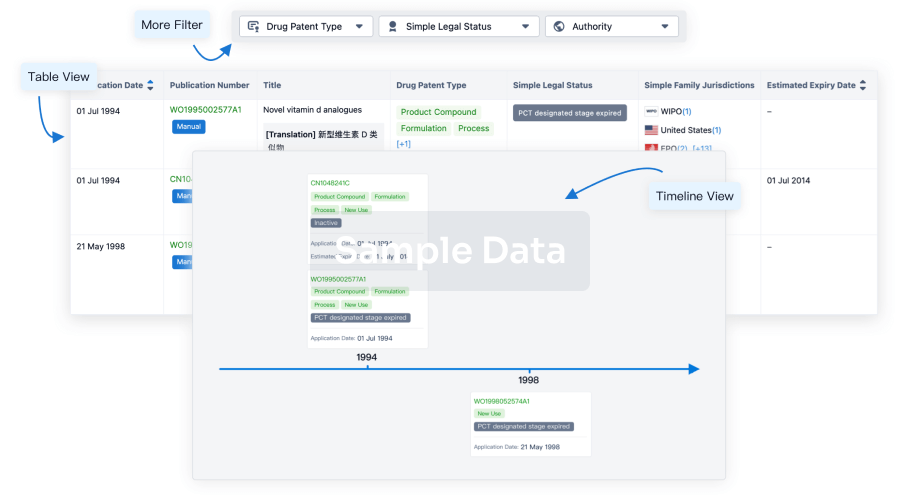
Core Patent
Boost your research with our Core Patent data.
login
or
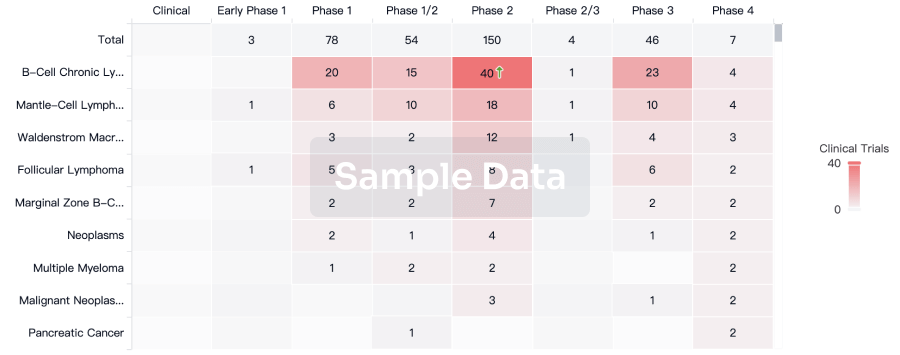
Clinical Trial
Identify the latest clinical trials across global registries.
login
or
Approval
Accelerate your research with the latest regulatory approval information.
login
or
Regulation
Understand key drug designations in just a few clicks with Synapse.
login
or
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free