Request Demo
Last update 04 Apr 2026
Atrial natriuretic peptide(Beijing SL Pharmaceutical)
Last update 04 Apr 2026
Overview
Basic Info
Drug Type Recombinant polypeptide |
Synonyms atrial natriuretic peptide(Beijing SL Pharmaceutical) |
Target |
Action agonists |
Mechanism NPRA agonists(Natriuretic peptide receptor 1 agonists) |
Therapeutic Areas |
Active Indication- |
Inactive Indication |
Originator Organization |
Active Organization- |
Inactive Organization |
License Organization- |
Drug Highest PhasePendingDiscovery |
First Approval Date- |
Regulation- |
Related
3
Clinical Trials associated with Atrial natriuretic peptide(Beijing SL Pharmaceutical)JPRN-UMIN000010970
Elucidation of renal function protection with human atrial natriuretic peptide (hANP) - Elucidation of renal function protection with hANP
JPRN-UMIN000003909
the Prevention of Contrast-Induced Nephropathy by Atrial Natriuretic Peptide in Endovascular Aneurysm Repair. - the Prevention of Contrast-Induced Nephropathy by Atrial Natriuretic Peptide in Endovascular Aneurysm Repair.
JPRN-UMIN000001524
Efficacy of Low-Dose Continuous Infusion of Human Atrial Natriuretic Peptide (hANP) During Lung Resection Surgery - Efficacy of hANP During Lung Resection Surgery
100 Clinical Results associated with Atrial natriuretic peptide(Beijing SL Pharmaceutical)
Login to view more data
100 Translational Medicine associated with Atrial natriuretic peptide(Beijing SL Pharmaceutical)
Login to view more data
100 Patents (Medical) associated with Atrial natriuretic peptide(Beijing SL Pharmaceutical)
Login to view more data
15
Literatures (Medical) associated with Atrial natriuretic peptide(Beijing SL Pharmaceutical)01 Feb 2002Journal of chromatography. B, Analytical technologies in the biomedical and life sciencesQ3 · MEDICINE
Quantitative liquid chromatography-mass spectrometry determination of isatin in urine using automated on-line extraction
Q3 · MEDICINE
Article
Author: Holzgrabe, Ulrike ; Benet, Leslie Z. ; Unger, Matthias ; Jacobsen, Wolfgang
Here we describe a simple, fast and sensitive liquid chromatography/mass spectrometry method with automated on-line extraction to quantify isatin, an endogenous monoamine oxidase, and atrial natriuretic peptide inhibitor, in urine. After derivatisation of isatin to isatinoxime with hydroxylamine hydrochloride and zinc sulfate precipitation, samples were loaded on the extraction column, washed and, after activation of the column-switching valve, backflushed onto the analytical column. Using electrospray ionisation, [M+H]+ ions could be detected in the selected ion monitoring mode. The assay was linear from 5 to 5000 ng/ml (r2>0.99) and analytical recovery was >80%. Inter-assay precision for the quality control samples was less than 3% and inter-assay accuracy was within +/- 5%.
01 May 1997Critical care medicineQ1 · MEDICINE
The atrial natriuretic peptide receptor antagonist HS 142-1 improves cardiovascular filling and mean arterial pressure in a hyperdynamic ovine model of sepsis
Q1 · MEDICINE
Article
Author: Lillian D. Traber ; Michael Booke ; Daniel L. Traber ; Frank Hinder
OBJECTIVE:
To test whether systemic vascular resistance and mean arterial pressure increase during the administration of the atrial natriuretic peptide antagonist, HS 142-1, in ovine experimental hyperdynamic sepsis.
DESIGN:
Prospective trial.
SETTING:
Research laboratory at a large university medical center.
SUBJECTS:
Chronically instrumented Merino breed ewes (n = 14).
INTERVENTIONS:
Continuous infusion of Pseudomonas aeruginosa (2.5 x 10(6) colony-forming units/min) for the experimental period of 48 hrs. One group (HS 142-1) received a continuous infusion of HS 142-1 (3 mg/kg/hr) from 40 to 48 hrs; the remaining sheep ("control") were given the vehicle sodium chloride 0.9%.
MEASUREMENTS AND MAIN RESULTS:
All sheep developed a hyperdynamic cardiovascular response by 40 hrs that was characterized by low values of systemic vascular resistance index (p < .05) and mean arterial pressure (p < .05), and an increased cardiac index (p < .05). HS 142-1 increased cardiac filling pressures (p < .05) without apparent effects on fluid balance, and was associated with a significantly (p < .05) higher mean arterial pressure than was found in the control group at 44 and 48 hrs. HS 142-1 did not change systemic vascular resistance index. At 44 and 48 hrs, cardiac index values were found to have significantly (p < .05) increased in the animals receiving HS 142-1, when these data were compared with cardiac output values at 40 hrs.
CONCLUSION:
HS 142-1 increases cardiac filling pressures and maintains mean arterial pressure in hyperdynamic sepsis without reversal of sepsis-induced vasodilation.
01 Jan 1994The American journal of physiology
ANF-C-receptor-mediated inhibition of aortic smooth muscle cell proliferation and thymidine kinase activity
Article
Author: Hassid, A. ; Cahill, P. A.
We have investigated the inhibition of DNA synthesis and cell proliferation by rat atrial natriuretic factor [rANF-(99-126)] and several synthetic peptides that bind selectively to the ANF-C-type clearance receptors in subcultured aortic smooth muscle cells. These peptides decreased serum-induced 1) [3H]thymidine incorporation, 2) cell proliferation, and 3) thymidine kinase activity without altering basal or elevated cAMP or cGMP levels. In contrast, another ANF-C-receptor-binding peptide, des[Gln116,Ser117,Gly118,Leu119,Gly120] rANF-(102-121)-NH2 (cANF), failed to decrease serum-induced mitogenesis, yet 100 nM cANF reversed the inhibition of DNA synthesis and cell proliferation and the decrease of thymidine kinase activity elicited by other C receptor-binding peptides, including rANF-(99-126), rANF-(103-125), and porcine C-type natriuretic peptide [pCNP-(1-22)]. Delayed addition experiments indicated that atrial peptides influence a relatively late event (or events) during the G1 phase of the cell cycle. The inhibition of DNA synthesis by C-receptor-binding atrial peptides appeared to be selective for aortic smooth muscle cells, inasmuch as a potent inhibitory agonist peptide, Cys116-rANF-(102-116), was without significant influence on the incorporation of thymidine in cultured rat mesangial cells or bovine pulmonary artery endothelial cells. These results indicate that atrial natriuretic peptide analogues decrease vascular smooth muscle cell mitogenesis and proliferation by a cyclic nucleotide-independent mechanism involving the C-type receptor. Moreover the inhibition of DNA synthesis by rANF-(99-126) and the neuropeptide pCNP-(1-22) appears to be mediated by the ANF-C-type receptor and is associated with inhibition of thymidine kinase activity.
100 Deals associated with Atrial natriuretic peptide(Beijing SL Pharmaceutical)
Login to view more data
R&D Status
10 top R&D records. to view more data
Login
| Indication | Highest Phase | Country/Location | Organization | Date |
|---|---|---|---|---|
| Heart Failure | Discovery | China | - |
Login to view more data
Clinical Result
Clinical Result
Indication
Phase
Evaluation
View All Results
Login to view more data
Translational Medicine
Boost your research with our translational medicine data.
login
or

Deal
Boost your decision using our deal data.
login
or

Core Patent
Boost your research with our Core Patent data.
login
or

Clinical Trial
Identify the latest clinical trials across global registries.
login
or

Approval
Accelerate your research with the latest regulatory approval information.
login
or

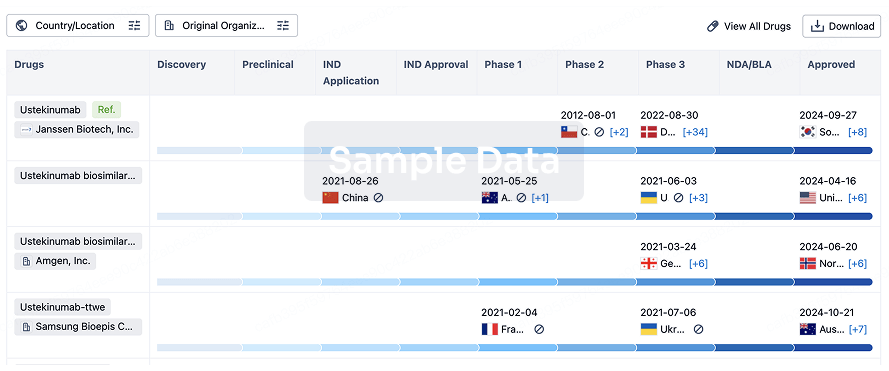
Biosimilar
Competitive landscape of biosimilars in different countries/locations. Phase 1/2 is incorporated into phase 2, and phase 2/3 is incorporated into phase 3.
login
or
Regulation
Understand key drug designations in just a few clicks with Synapse.
login
or

AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free