Request Demo
Last update 23 Aug 2025
Semaglutide(Merdury Biopharmaceutical Corporation)
Last update 23 Aug 2025
Overview
Basic Info
Drug Type Recombinant polypeptide |
Synonyms- |
Target |
Action modulators |
Mechanism GLP-1R modulators(Glucagon-like peptide 1 receptor modulators) |
Therapeutic Areas |
Active Indication |
Inactive Indication- |
Originator Organization |
Active Organization |
Inactive Organization- |
License Organization- |
Drug Highest PhasePreclinical |
First Approval Date- |
Regulation- |
Related
2
Clinical Trials associated with Semaglutide(Merdury Biopharmaceutical Corporation)ChiCTR2500096141
The effect of semaglutide injection on gastric emptying time
JPRN-UMIN000042482
Effect of Semaglutide 0.25mg on glycemic controls in type2 diabetes patients compared with dulaglutide 0.75mg. - Effect of Semaglutide 0.25mg on glycemic controls in type2 diabetes patients compared with dulaglutide 0.75mg.
100 Clinical Results associated with Semaglutide(Merdury Biopharmaceutical Corporation)
Login to view more data
100 Translational Medicine associated with Semaglutide(Merdury Biopharmaceutical Corporation)
Login to view more data
100 Patents (Medical) associated with Semaglutide(Merdury Biopharmaceutical Corporation)
Login to view more data
285
Literatures (Medical) associated with Semaglutide(Merdury Biopharmaceutical Corporation)01 Oct 2025EUROPEAN JOURNAL OF PHARMACOLOGY
Real-world safety comparison of liraglutide and semaglutide in weight management: Insights from European pharmacovigilance data
Article
Author: Esposito, Katherine ; Caruso, Paola ; Capuano, Annalisa ; Ruggiero, Rosanna ; Mascolo, Annamaria ; Longo, Miriam ; D'Amato, Rossana ; Di Nuzzo, Michela ; Maiorino, Maria Ida ; Laino, Ludovica Vittoria ; Rafaniello, Concetta
BACKGROUND:
In recent years, the use of glucagon-like peptide-1 receptor agonists (GLP-1 RAs), as liraglutide and semaglutide, for weight management has significantly risen. Even if these medications are effective, some concerns remain about their safety profiles, particularly regarding long-term adverse events (AEs). This study provides an evaluation of the safety profiles of liraglutide and semaglutide in a real-world setting.
METHODS:
A retrospective case-non-case study was conducted using data from the EudraVigilance database. All cases involving liraglutide or semaglutide used for weight management and collected in the database between January 2018 and December 2023 were analyzed. Disproportionality analysis was performed to assess the reporting odds ratios for events of interest (gastrointestinal events, pancreatitis, gallbladders disorders, psychiatric events, and gallbladder, pancreatic or thyroid tumors) reported at least three times.
RESULTS:
A total of 27,639 cases were identified. Most cases occurred in female patients aged 18-64 years. Most reported AEs were not-serious. Gastrointestinal events were the most common, with nausea, vomiting, and diarrhea leading the list. Two events were related to gallbladder tumors. Disproportionality analysis revealed that liraglutide was associated with a higher reporting frequency of pancreatitis, gallbladder disorders, and thyroid tumors, while semaglutide showed a greater likelihood of vomiting and abdominal pain. No significant differences were found for other common gastrointestinal events, pancreatic tumors, depression, or suicidal ideation.
CONCLUSIONS:
Liraglutide and semaglutide showed distinct safety profiles when used for weight management. These findings highlight the importance of considering individual patient profiles and potential risks when prescribing these medications for weight management. Further real-world studies are needed to explore long-term safety and to clarify the potential association between GLP-1 RAs and malignancies.
01 Sep 2025Obesity Pillars
Knowledge, attitudes, and practices in obesity among trained and in-training primary care providers in an urban safety-net hospital system
Article
Author: Rizo, Ivania ; Fantasia, Kathryn L ; Campos, Alejandro
Background:
Obesity is a highly prevalent, chronic, and treatable disease that disproportionately impacts some minoritized populations who seek care in safety-net settings. Given that primary care providers (PCPs) often serve as the initial point of contact for patients, we aimed to assess their knowledge, attitudes, and practices related to management of obesity.
Methods:
This was a cross-sectional study conducted to assess knowledge, attitudes, and practices on obesity management through an anonymous, electronic survey among trained (MD/DO and NP) and in-training (residents) primary care providers (PCPs) in the Departments of Internal Medicine and Family Medicine within an urban safety-net healthcare system.
Results:
Among 350 sampled, 96 PCPs completed the survey (27 % response rate). Participants were predominantly (60.4 %) Internal Medicine trainees. The majority of PCPs accurately identified common weight-related comorbidities and improvement of these with >10 % weight loss. Only 25 % of PCPs correctly identified both body mass index (BMI) criteria for anti-obesity medication (AOM) prescription and only 9.1 % identified both BMI criteria for bariatric surgery. Nearly two-thirds (64 %) of PCPs reported prescribing AOMs, with greater comfort in using glucagon like peptide-1 receptor agonist (GLP-1 RA) injectable agents (semaglutide and liraglutide) than with older oral AOMs (phentermine, phentermine-topiramate, and naltrexone-bupropion). Knowledge about side effects and insurance coverage were reported as influencing AOM prescription. Time constraints and lack of training and/or knowledge were identified as barriers in obesity management by more than 50 % of PCPs.
Conclusions:
Our study highlights gaps in obesity-related knowledge and practice among PCPs, emphasizing the need for enhanced training, clinical support, and policy reforms to improve obesity management and patient outcomes.
01 Sep 2025EUROPEAN JOURNAL OF PHARMACOLOGY
Lanifibranor and semaglutide demonstrate multiple metabolic benefits in free-choice diet induced obese hamster models of MASH and MetALD
Article
Author: Wettstein, Guillaume ; Sulpice, Thierry ; Broqua, Pierre ; Assaly, Rana ; Bigot, Claire ; Briand, François ; Dubroca, Caroline ; Breyner, Natalia ; Grasset, Estelle
Obesity is associated with several comorbidities including Heart Failure with preserved Ejection Fraction (HFpEF), Metabolic dysfunction-Associated SteatoHepatitis (MASH), also termed MetALD when MASH patients have increased alcohol intake. The worldwide epidemic of obesity creates a constant need for new therapies and animal models to test their effectiveness. In the present study, we evaluated the effects of the GLP-1 receptor agonist semaglutide and the pan-PPAR agonist lanifibranor in the free choice diet induced obese MASH hamster, a preclinical model with human-like lipoprotein metabolism, MASH and HFpEF. The same model was exposed to ethanol to evaluate the effects of both semaglutide and lanifibranor on chronic alcohol intake. To set up a model of MetALD, obese MASH hamsters were also challenged to alcohol binge drinking and the preventative effects of lanifibranor were evaluated. Compared with vehicle, semaglutide transiently reduced food intake and significantly reduced fructose and alcohol consumption. This effect was associated with significant body weight loss, lower HOMA-IR index of insulin resistance, improved dyslipidemia and HFpEF, but semaglutide only reduced hepatic fat content. Lanifibranor showed the same cardiometabolic benefits but had superior effects in the liver, with significant improvement in MASH and MetALD. As observed in humans, lanifibranor and semaglutide showed multiple metabolic benefits in free-choice diet induced obese hamster models of MASH and MetALD. These hamster models demonstrated good translability regarding the effects observed in clinical trials and will be helpful to evaluate novel therapies targeting obesity and associated comorbidities, including MetALD.
4
News (Medical) associated with Semaglutide(Merdury Biopharmaceutical Corporation)30 Jul 2025

Phase 1Financial Statement
06 Jun 2025
100 Deals associated with Semaglutide(Merdury Biopharmaceutical Corporation)
Login to view more data
R&D Status
10 top R&D records. to view more data
Login
| Indication | Highest Phase | Country/Location | Organization | Date |
|---|---|---|---|---|
| Diabetes Mellitus | Preclinical | China | 25 Jul 2024 | |
| Obesity | Preclinical | China | 25 Jul 2024 |
Login to view more data
Clinical Result
Clinical Result
Indication
Phase
Evaluation
View All Results
Login to view more data
Translational Medicine
Boost your research with our translational medicine data.
login
or

Deal
Boost your decision using our deal data.
login
or

Core Patent
Boost your research with our Core Patent data.
login
or

Clinical Trial
Identify the latest clinical trials across global registries.
login
or

Approval
Accelerate your research with the latest regulatory approval information.
login
or

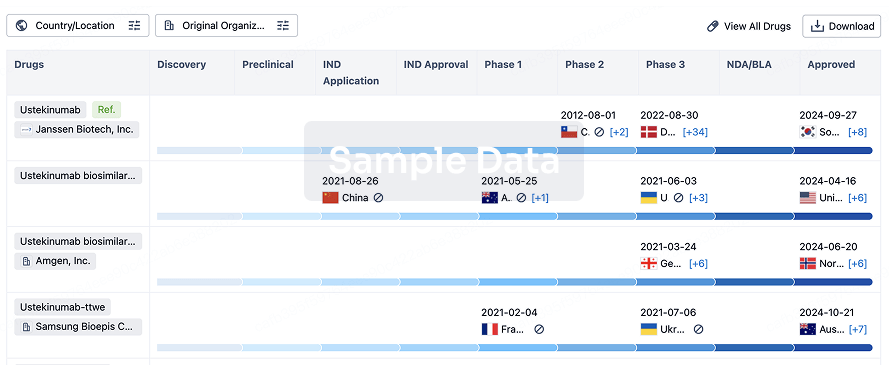
Biosimilar
Competitive landscape of biosimilars in different countries/locations. Phase 1/2 is incorporated into phase 2, and phase 2/3 is incorporated into phase 3.
login
or
Regulation
Understand key drug designations in just a few clicks with Synapse.
login
or

AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free