Request Demo
Last update 03 May 2025
Ocrelizumab biosimilar(Cinnagen)
Last update 03 May 2025
Overview
Basic Info
Drug Type Biosimilar, Monoclonal antibody |
Synonyms Ocrelizumab Biosimilar (CinnaGen Co.), Xacrel, 奥瑞珠单抗生物类似药(CinnaGen Co.) |
Target |
Action inhibitors |
Mechanism CD20 inhibitors(B-lymphocyte antigen CD20 inhibitors), ADCC(Antibody-dependent cell-mediated cytotoxicity (ADCC) effects), CD20-directed cytolytic effects |
Therapeutic Areas |
Active Indication- |
Inactive Indication |
Originator Organization |
Active Organization- |
Inactive Organization |
Drug Highest PhasePendingPhase 3 |
First Approval Date- |
Regulation- |

Login to view timeline
Structure/Sequence
Sequence Code 31212L
The sequence is quoted from: *****
Sequence Code 42721H
The sequence is quoted from: *****
Related
1
Clinical Trials associated with Ocrelizumab biosimilar(Cinnagen)NCT04966338
A Phase III, Randomized, Two-armed, Double-blind, Parallel, Active-controlled Clinical Trial to Evaluate Equivalency of the Efficacy and Safety of Ocrelizumab (CinnaGen, Iran) in Comparison to Reference Product, Ocrevus® (Roche, Switzerland) in Patients With Relapsing Multiple Sclerosis
100 Clinical Results associated with Ocrelizumab biosimilar(Cinnagen)
Login to view more data
100 Translational Medicine associated with Ocrelizumab biosimilar(Cinnagen)
Login to view more data
100 Patents (Medical) associated with Ocrelizumab biosimilar(Cinnagen)
Login to view more data
2
Literatures (Medical) associated with Ocrelizumab biosimilar(Cinnagen)01 Feb 2024ACTA NEUROLOGICA BELGICA
Comparing infusion-related reactions of the first full dose (600 mg) biosimilar ocrelizumab administration with the standard divided protocol in multiple sclerosis patients: a randomized controlled trial study
Article
Author: Baghbanian, S. M. ; Navardi, S ; Hosseini, S. ; Kamali, H. ; Langroodi, H. Ghalyanchi ; Ameli, Z ; Sahraian, M. A. ; Ghadiri, F. ; Navardi, S. ; Kamali, H ; Nahayati, M A ; Abbasi Kasbi, Naghmeh ; Moghadasi, A Naser ; Poursadeghfard, M. ; Ghadiri, F ; Nahayati, M. A. ; Baghbanian, S M ; Shahmohammadi, S ; Moghadasi, A. Naser ; Hosseini, S ; Langroodi, H Ghalyanchi ; Heidari, H ; Heidari, H. ; Sahraian, M A ; Shahmohammadi, S. ; Poursadeghfard, M ; Ameli, Z.
BACKGROUND:
Ocrelizumab is a humanized antiCD20, thought to be a highly effective disease-modifying therapy (DMT). Its most frequent adverse effects are infusion-related reactions (IRRs). To reduce these reactions, the first dose of ocrelizumab is administered as two 300 mg infusions separated by two weeks. However, in the phase II trial of ocrelizumab, severe IRRs were not significantly different between two doses of 600 mg dose (two separate 300 mg doses) and 2000 mg dose (two separate 1000 mg doses). We compared the IRRs in undivided full (one 600 mg) and divided (two 300 mg) doses of ocrelizumab which is the standard protocol.
METHODS:
MS patients (relapsing or primary progressive MS) who are selected to receive ocrelizumab by neurologist or MS fellowship were enrolled in an open-label randomized controlled trial. Iranian biosimilar of the drug (Xacrel® by Cinnagen, approved by the Iranian Food and Drug Administration in 2021) was used. The participants received the first dose of ocrelizumab as either one 600 mg dose in one session or two 300 mg doses in two weeks apart. IRRs during or in the first 24 h after infusion were recorded.
RESULTS:
Of 332 participants, 150 received two 300 mg doses, and 182 received one 600 mg dose (by random selection). Life-threatening adverse effects were not observed in both groups. Overnight admission or permanent drug discontinuation was not needed. Temporary drug discontinuation was significantly higher in the one 600 mg dose group (p-value < 0.001). During the infusions, malaise (p-value: 0.003), skin reactions (p-value: 0.04), throat swelling (p-value: 0.03), and dyspnea (p-value: 0.01) were significantly increased in the intervention group. However, in the first 24 h, there was no significant difference between two different treatment protocols (one 600 mg dose or two 300 mg doses) in the onset of IRRS (p-value: 0.12).
CONCLUSION:
These findings suggest one 600 mg dose of ocrelizumab administration for the first dose is relatively safe. With some protocol modifications, it could lead to fewer patient referrals, saving time and cost and improvement the access for patients.
Scientific Reports
Evaluating efficacy and safety of ocrelizumab biosimilar (Xacrel) compared to the originator (Ocrevus) in relapsing multiple sclerosis: a phase III, randomized, equivalency, clinical trial
Article
Author: Baghbanian, Seyed Mohammad ; Ghiasian, Masoud ; Razazian, Nazanin ; Nikseresht, Alireza ; Naser Moghadasi, Abdorreza ; Asadollahzadeh, Elnaz ; Albooyeh, Sogol ; Kafi, Hamidreza ; Sahraian, Mohammad Ali ; Mohammadianinejad, Seyed Ehsan ; Ghalyanchi Langroodi, Hamidreza ; Abolfazli, Roya ; Beladi Moghadam, Nahid ; Ashtari, Fereshteh ; Shaygannejad, Vahid ; Sedighi, Behnaz ; Navardi, Samira ; Majdinasab, Nastaran ; Nahayati, Mohammad Ali ; Ayromlou, Hormoz ; Sabzvari, Araz
Multiple sclerosis is an inflammatory demyelinating disease and represents a global health concern. Ocrelizumab, a humanized IgG monoclonal antibody, selectively targets CD20 on B cells and CD20-expressing T cells. This study aimed to compare the efficacy and safety of the biosimilar ocrelizumab candidate (Xacrel) to the originator product (Ocrevus) in Relapsing Multiple Sclerosis (RMS) patients. In this randomized trial, patients received either Xacrel or Ocrevus for 96 weeks. The primary endpoint was the equivalency of the medications in reducing the annualized relapse rate (ARR) at week 48. The secondary endpoints included time to the onset of disability progression confirmed at 12 and 24 weeks, the proportion of relapse-free patients, magnetic resonance imaging (MRI) evaluations, safety assessments, and immunogenicity over 96 weeks. A total of 170 patients were randomized (1:1 ratio). In the per protocol analysis, the upper and lower limits of 95% two-sided confidence intervals of difference between treatments in the 48-week ARR rate were in the predefined margin of - 0.2 to 0.2 (- 0.002; 95% CI - 0.080 to 0.075). The two products were also comparable in terms of other efficacy parameters, safety, and immunogenicity. The results confirmed that Xacrel is equivalent to Ocrevus in terms of 48-week ARR in RMS patients, with no considerable difference in other efficacy parameters and the safety profile during the 96 weeks. The trial was registered in Iranian registry of clinical trials (IRCT) on 10/06/2019 with the registration number of IRCT20150303021315N13 and in Clinicaltrials.gov on 19/07/2021 with the registration code of NCT04966338.
100 Deals associated with Ocrelizumab biosimilar(Cinnagen)
Login to view more data
External Link
| KEGG | Wiki | ATC | Drug Bank |
|---|---|---|---|
| - | - | - |
R&D Status
10 top R&D records. to view more data
Login
| Indication | Highest Phase | Country/Location | Organization | Date |
|---|---|---|---|---|
| Multiple sclerosis relapse | Phase 3 | Iran | 19 Aug 2019 | |
| Multiple Sclerosis, Relapsing-Remitting | Phase 3 | Iran | 19 Aug 2019 |
Login to view more data
Clinical Result
Clinical Result
Indication
Phase
Evaluation
View All Results
Login to view more data
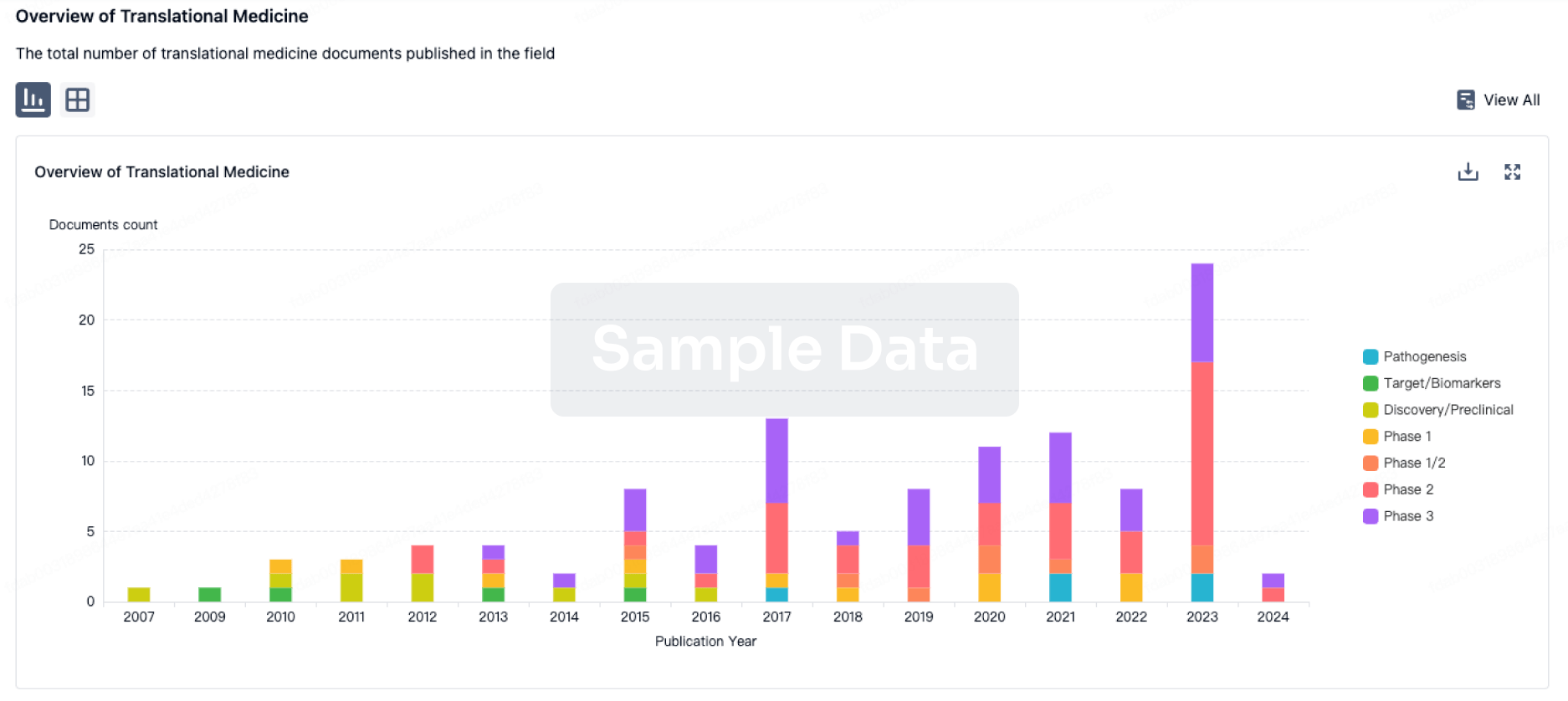
Translational Medicine
Boost your research with our translational medicine data.
login
or
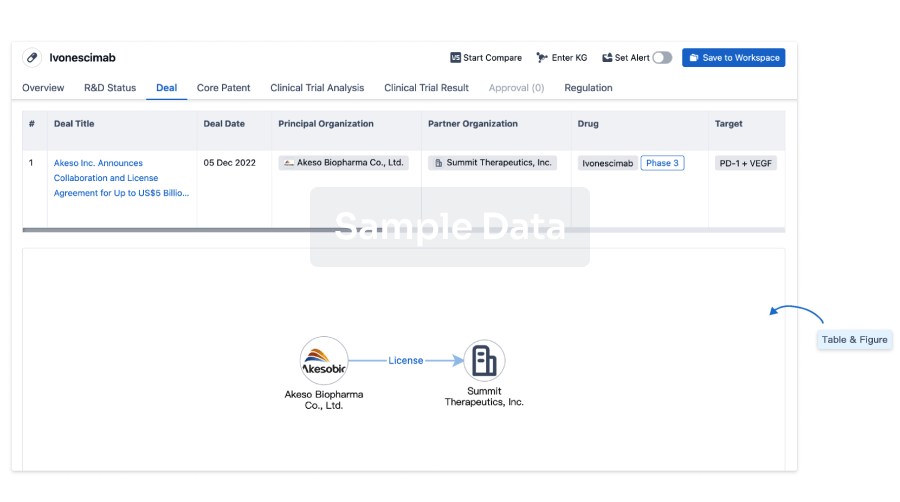
Deal
Boost your decision using our deal data.
login
or
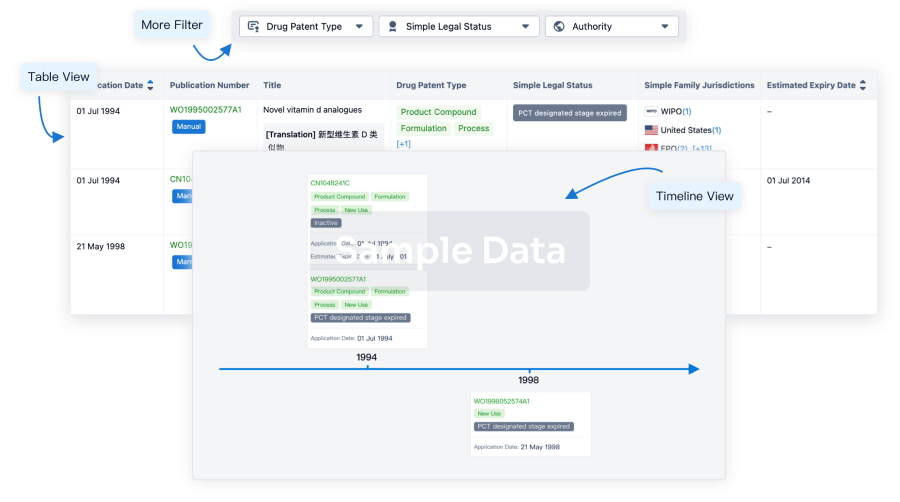
Core Patent
Boost your research with our Core Patent data.
login
or
Clinical Trial
Identify the latest clinical trials across global registries.
login
or
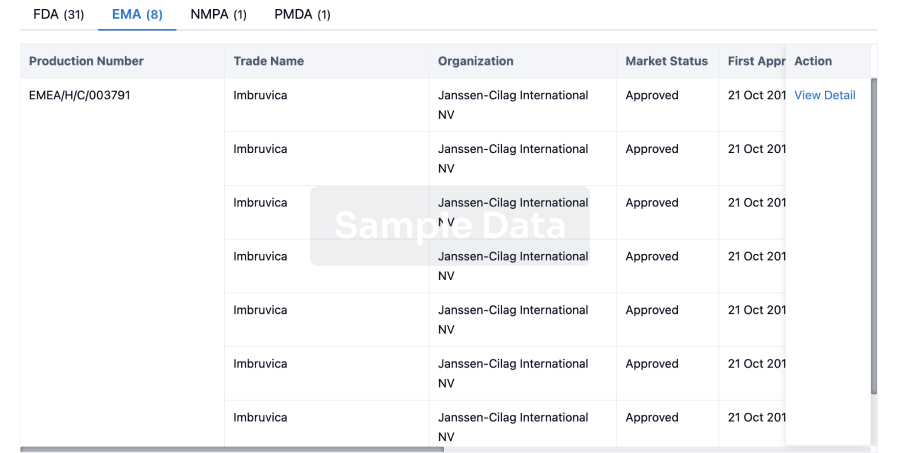
Approval
Accelerate your research with the latest regulatory approval information.
login
or
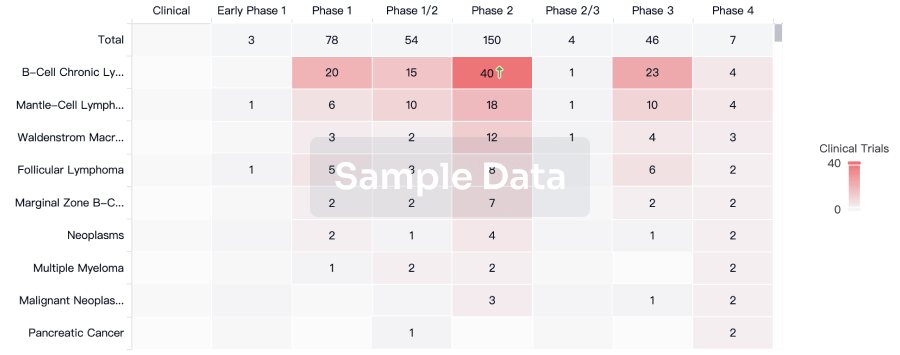
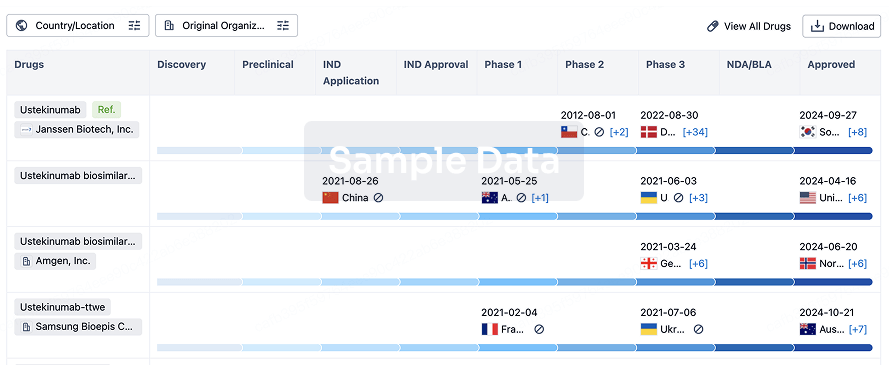
Biosimilar
Competitive landscape of biosimilars in different countries/locations. Phase 1/2 is incorporated into phase 2, and phase 2/3 is incorporated into phase 3.
login
or
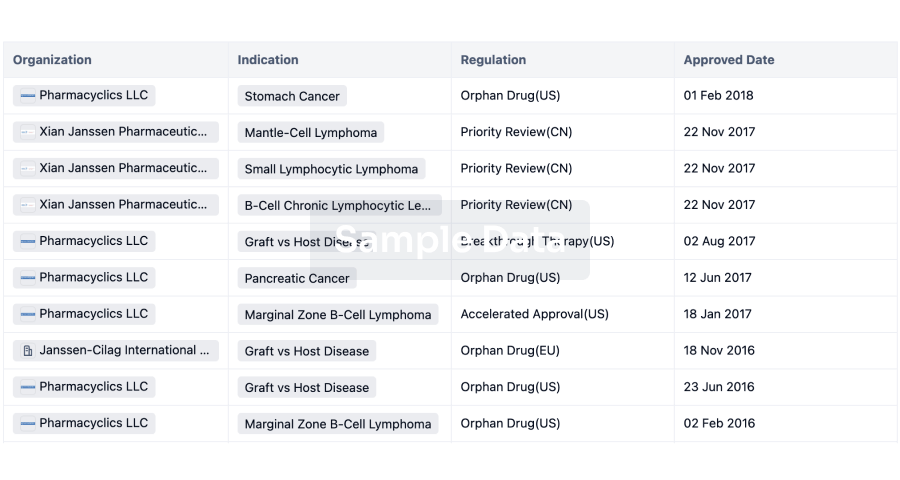
Regulation
Understand key drug designations in just a few clicks with Synapse.
login
or
Chat with Hiro
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free