Request Demo
Last update 06 Dec 2025
Last update 06 Dec 2025
Overview
Related
100 Clinical Results associated with
Login to view more data
0 Patents (Medical) associated with
Login to view more data
6
Literatures (Medical) associated with 01 May 2016·British journal of cancerQ1 · MEDICINE
Comment on ‘Tumour antigen expression in hepatocellular carcinoma in a low-endemic western area’
Q1 · MEDICINE
Letter
Author: Qehajaj, D ; Stifter, S ; Grizzi, F ; Chiriva-Internati, M
A review.Sir, We read with great interest the study by Sideras et al (2015) that combines tissue microarrays (TMA) and immunohistochem. to investigate the expression pattern of 15 antigens belonging to different categories, including cancer testis antigens (CTAs) and oncofetal proteins in primary hepatocellular carcinoma (HCC).Because current therapies for HCC are far from ideal (Ilan, 2014) and immunotherapy has been proposed as a potential therapeutic option, the authors aimed at identifying a panel of relevant tumor antigens with broad expression in a Western European population of HCC patients and specific expression in the tumor tissue (Sideras et al, 2015).Cancer testis antigens represent a family of >200 proteins selectively expressed in malignant cells, but not in their natural counterpart except for human germ cells (Simpson et al, 2005; Gjerstorff et al, 2015; Grizzi et al, 2015).Among the different types of tumor antigens, CTAs identified highly promising therapeutic targets (Gjerstorff et al, 2015).In contrast to previous studies (Xu et al, 2012; Liang et al, 2013; Xia et al, 2013; Wang et al, 2015), Sideras et al (2015) found a low (<10% of patients) prevalence of expression of MAGE-A3/4, NY-ESO-1, MAGE-A1 and MAGE-A10.Moreover, a low (<10% of patients) prevalence of expression of the fetal specific glycoprotein alpha-fetoprotein (AFP) was found.Although its serum level falls rapidly after birth and its synthesis in adult life is repressed, >70% of HCC-affected patients have usually a high serum concentration of AFP.Today, AFP and ultrasonog. are the main tests for HCC surveillance in clin. practice, and in the interim, using ultrasonog. and AFP in combination may be the best strategy to optimize early HCC detection (Mehta and Singal, 2015).Sideras et al (2015) stated that the observed prevalence of expression of CTAs and oncofetal antigens was generally lower because previous studies have been conducted in East Asia where hepatitis B virus infection is the prevalent cause of HCC and the majority of HCC patients have liver cirrhosis.Furthermore, previous investigators used RT-PCR measuring mRNA expression, whereas they evaluated protein expression by immunohistochem.Here, we would like to discuss addnl. points underlying these discrepancies and that impact on the CTAs as immunotherapeutic targets.In an effort to accelerate translation of new developments in basic immunol. into cancer patients, representatives from eight immunotherapy organisations representing Europe, Japan, China and North America convened an 'Immunotherapy Summit' at the 24th Annual Meeting of the International Society for Biol. Therapy of Cancer (now called Society for Immunotherapy of Cancer, SITC).One of the concepts raised by SITC and defined as critical was the need to identify hurdles that impede effective translation of cancer immunotherapy (Fox et al, 2011).The critical hurdles highlighted have been grouped into nine general themes.Among these have been identified the 'complexity of cancer', its 'heterogeneity' and 'immune escape' (Fox et al, 2011).Hepatocellular carcinoma originates and progresses throughout a dynamic process involving different 'driven alterations' that ultimately lead to the malignant transformation of hepatocytes.Malignant transformation may occur regardless of the etiol. agent through a pathway of increased liver cell turnover, induced by chronic liver injury and regeneration in a context of inflammation, immune response and oxidative DNA damage (Li and Wang, 2015).Hepatocellular carcinoma is a heterogeneous disease in 'space' and in 'time'.The term 'heterogeneity' defines the presence of cell clones, within a tumoral mass, with different genetic aberrations that mediate divergent biol. defining the natural history of that particular tumor, i.e., one clone does not represent the entirety of the tumor cell population.This variability is what ultimately determines the evolutionary progression of neoplastic disease and its response to therapy (Luo et al, 2009).Singular cells respond differently to the same stimulus, with some not responding at all (Floor et al, 2012; Almendro et al, 2013).These considerations, in conjunction with the complexity of 'tumor-host' interactions caused by temporal changes in tumor phenotypes and an array of immune mediators expressed in the tumor microenvironment, might explain the limited reliability and applicability of current therapeutic strategies.Sideras et al (2015) did not report fundamental hallmarks of cancer, including 'cancer complexity', 'tumor heterogeneity' and 'field cancerization', i.e., the presence of abnormal tissue surrounding primary cancerous lesions.These observations lead us to reflect on the appropriateness of TMAs to state the CTAs and oncofetal proteins as potential therapeutic targets.It is known that diagnostic accuracy of a histol. assay may be affected if the 'target antigen' is uniquely present in a fraction of a tumor (Sottoriva et al, 2015).Tissue microarray consists of small fractions of tissue inserted into a recipient paraffin block such that a tissue section on a single glass slide can contain numerous patient samples in a spatially structured pattern.Although the study of whole-tissue sections for the evaluation of large tumor cohorts is tedious and costly, the genome-wide network of intra-tumor heterogeneity across multiple spatial and temporal scales, and patient-specific patterns of cancer evolution limits the appropriateness of investigating a small fraction of tissue, and is prone to controversial results and consequences for treatment design (Chiriva-Internati et al, 2004).In addition, Sideras et al (2015) applied a scoring system, called 'H-score' obtained by multiplying the intensity score (range: 0-3) with the level of % of pos. cells, where 1≤5%, 2=5-25%, 3=25-75% and 4 ≥75%.However, this approach generates equivalent 'math. products', (i.e., condition 1: intensity=1 multiplied with the level of % of pos. cells 2=5-25% is the same product obtained multiplying intensity=2 with the level of % of pos. cells 1≤5%; condition 2: intensity=1 multiplied with the level of % of pos. cells 3=25-75% is the same product obtained multiplying intensity=3 with the level of % of pos. cells 1 <5%; condition 3: intensity=1 multiplied with the level of % of pos. cells 4 ≥75% is the same product obtained multiplying intensity=2 with the level of % of pos. cells 2=5-25%; condition 4: intensity=2 multiplied with the level of % of pos. cells 3=25-75% is the same product obtained multiplying intensity=3 with the level of % of pos. cells 2=5-25%), although their biol. significance is completely different.In other words, these overlapping 'scores' subtend different impacts on the capacity of CTAs to elicit the immune response and the heterogeneous behavior of HCC.In conclusion, to advance our knowledge in a currently widely debated field of investigation such as that of immunotherapy and HCC, a clearer distinction must be made between the exploration of CTA expression pattern and their real application in human clin. trials.Because the anal. of CTA expression is useful in identifying patients who are most likely to benefit from immune intervention strategies, we need to adopt a more adequate exptl. approach and a change in our 'mind' from a 'qual.' or 'semi-quant.' to a more advanced 'quant.' thinking.
01 Dec 2015·Journal of translational medicineQ2 · MEDICINE
AAV2/8-humanFOXP3 gene therapy shows robust anti-atherosclerosis efficacy in LDLR-KO mice on high cholesterol diet
Q2 · MEDICINE
ArticleOA
Author: Chiriva-Internati, M ; Cao, M ; Figueroa, J A ; Theus, S A ; Straub, K D ; Hermonat, P L ; Mirandola, L
Inflammation is a key etiologic component in atherogenesis. Previously we demonstrated that adeno-associated virus (AAV) 2/8 gene delivery of Netrin1 inhibited atherosclerosis in the low density lipoprotein receptor knockout mice on high-cholesterol diet (LDLR-KO/HCD). One important finding from this study was that FOXP3 was strongly up-regulated in these Netrin1-treated animals, as FOXP3 is an anti-inflammatory gene, being the master transcription factor of regulatory T cells. These results suggested that the FOXP3 gene might potentially be used, itself, as an agent to limit atherosclerosis. To test this hypothesis AAV2/8 (AAV)/hFOXP3 or AAV/Neo (control) gene therapy virus were tail vein injected into the LDLR-KO/HCD animal model. It was found that hFOXP3 gene delivery was associated with significantly lower HCD-induced atherogenesis, as measured by larger aortic lumen cross sectional area, thinner aortic wall thickness, and lower aortic systolic blood velocity compared with Neo gene-HCD-treated controls. Moreover these measurements taken from the hFOXP3/HCD-treated animals very closely matched those measurements taken from the normal diet (ND) control animals. These data strongly suggest that AAV/hFOXP3 delivery gave a robust anti-atherosclerosis therapeutic effect and further suggest that FOXP3 be examined more stringently as a therapeutic gene for clinical use.
03 Sep 2014·International reviews of immunology
Editorial: International Reviews of Immunology
Article
Author: Internati, Maurizio Chiriva ; Bot, Adrian ; Mirandola, Leonardo
The immune system constantly patrols the body and, under steady-state conditions, it can generally eliminate abnormal, “transformed” cells before they can give rise to a tumor. This happens continu...
54
News (Medical) associated with 18 Feb 2025
HOUSTON--(BUSINESS WIRE)--Feb. 18, 2025-- Kiromic BioPharma, Inc. (OTCQB: KRBP) (“Kiromic” or the “Company”) reports continued favorable efficacy results from the 10-month follow-up visit for the fourth patient enrolled in its Deltacel-01 Phase 1 clinical trial and provides an enrollment update. This trial is evaluating Deltacel™ (KB-GDT-01), the Company’s allogeneic, off-the-shelf, Gamma Delta T-cell (GDT) therapy, in patients with stage 4 metastatic or locally-advanced non-small cell lung cancer (NSCLC) who have failed to respond to standard therapies.
The fourth patient in Deltacel-01 demonstrated a partial response (defined as a 30% or greater decrease in the size of the tumor) at the eight-month follow-up visit and continued without any evidence of disease progression as of the 10-month follow-up visit, thereby extending progression-free survival (PFS) to 10 months.
“We are very pleased that as of January 2025 Patient 4 had no evidence of disease progression since the partial response registered in November 2024, with a PFS of 10 months reinforcing our view that Deltacel may offer a transformative treatment option for people with advanced solid tumors,” said Pietro Bersani, Chief Executive Officer of Kiromic BioPharma. “Our team remains committed to advancing the Deltacel-01 clinical program, and we look forward to building upon these encouraging results as we expand the trial to additional participants.”
Additionally, Kiromic reports that two subjects are undergoing screening and are scheduled to start treatment at Texas Oncology in Tyler, Texas, in late February and early March, respectively.
About Deltacel-01
In Kiromic’s open-label Phase 1 clinical trial, titled “Phase 1 Trial Evaluating the Safety and Tolerability of Gamma Delta T Cell Infusions in Combination With Low Dose Radiotherapy in Subjects With Stage 4 Metastatic Non-Small Cell Lung Cancer” (NCT06069570), patients with advanced NSCLC receive three intravenous infusions of Deltacel™ with six courses of low-dose, localized radiation over a 31-day period. The primary objective of Deltacel-01 is to evaluate safety, while secondary measurements include objective response, progression-free survival, overall survival, time to progression, time to treatment response and disease control rates.
About Deltacel™
Deltacel™ (KB-GDT-01) is an investigational gamma delta T-cell (GDT) therapy currently in the Deltacel-01 Phase 1 trial for the treatment of stage 4 metastatic NSCLC. An allogeneic product consisting of unmodified, donor-derived gamma delta T cells, Deltacel™ is the leading candidate in Kiromic’s GDT platform. Deltacel™ is designed to exploit the natural potency of GDT cells to target solid cancers, with an initial clinical focus on NSCLC, which represents about 80% to 85% of all lung cancer cases. Data from two preclinical studies demonstrated Deltacel™’s favorable safety and efficacy profile when it was combined with low-dose radiation.
About Texas Oncology
With more than 530 physicians and 280 locations, Texas Oncology is an independent private practice that sees more than 71,000 new cancer patients each year. Founded in 1986, Texas Oncology provides comprehensive, multidisciplinary care and includes Texas Center for Proton Therapy, Texas Breast Specialists, Texas Colon & Rectal Specialists, Texas Oncology Surgical Specialists, Texas Urology Specialists and Texas Infusion and Imaging Center. Texas Oncology’s robust community-based clinical trials and research program have contributed to the development of more than 100 FDA-approved cancer therapies. Learn more at www.TexasOncology.com.
About the Beverly Hills Cancer Center
As a private, academic, community-based cancer center, the Beverly Hills Cancer Center not only provides the latest state-of-the-art cancer treatments all under one roof, but also provides leading clinical trials and research, attracting patients globally. By providing access to groundbreaking clinical trials, the Beverly Hills Cancer Center offers patients the opportunity to participate in the most advanced cancer treatments currently in development in the world. Beverly Hills Cancer Center is comprised of an internationally recognized multidisciplinary medical team consisting of medical oncologists, radiation oncologists, radiologists, hematologists and internists who provide exceptional patient care and support services including a robust and highly efficient team of clinical research professionals. More information is available at www.BHCancerCenter.com.
About Kiromic BioPharma
Kiromic BioPharma, Inc. is a clinical-stage, fully integrated biotherapeutics company developing a multi-indication allogeneic cell therapy platform that exploits the natural potency of Gamma Delta T-cells to target solid tumors. Kiromic is using its proprietary DIAMOND® artificial intelligence (AI) 2.0 platform to discover novel targets for immuno-oncology. The Company maintains offices in Houston, Texas. To learn more, visit www.kiromic.com and connect with us on Twitter and LinkedIn.
Forward-Looking Statements
This press release contains forward-looking statements that involve substantial risks and uncertainties. All statements other than statements of historical facts are forward-looking statements. In some cases, you can identify forward-looking statements by terms such as: “will,” “potential,” “could,” “can,” “believe,” “intends,” “continue,” “plans,” “expects,” “anticipates,” “estimates,” “may,” or the negative of these terms or other comparable terminology. These forward-looking statements include, but are not limited to, statements regarding: Kiromic’s ability to achieve its objectives and Kiromic’s financing strategy and availability of funds. These forward-looking statements involve known and unknown risks, uncertainties and other factors that may cause actual results, levels of activity, performance, or achievements to be materially different from the information expressed or implied expressed or implied by these forward-looking statements. These risks and uncertainties include, but are not limited to, the risks and uncertainties discussed in our Annual Report on Form 10-K for the year ended December 31, 2024, and as detailed from time to time in our other SEC filings. You should not rely upon forward-looking statements as predictions of future events. Although we believe that the expectations reflected in the forward-looking statements are reasonable, we cannot guarantee that the future results, levels of activity, performance, or events and circumstances reflected in the forward-looking statements will be achieved or occur. Moreover, neither we nor any other person assumes responsibility for the accuracy and completeness of the forward-looking statements. Such forward-looking statements relate only to events as of the date of this press release. We undertake no obligation to update any forward-looking statements except to the extent required by law.
View source version on businesswire.com: https://www.businesswire.com/news/home/20250218269453/en/
Alliance Advisors IR Tirth T. Patel tpatel@allianceadvisors.com 212-201-6614
Beverly Hills Cancer Center Sharon Neman, MBA Chief Strategy Officer SN@bhcancercenter.com 310-432-8925
Source: Kiromic BioPharma, Inc.
Phase 1Clinical ResultCell TherapyRadiation Therapy
21 Jan 2025
Provides Enrollment Update for Phase 1 Study in Late-Stage Non-small Cell Lung Cancer
HOUSTON--(BUSINESS WIRE)--Jan. 21, 2025-- Kiromic BioPharma, Inc. (OTCQB: KRBP) (“Kiromic” or the “Company”) reports favorable efficacy results from the 12-month follow-up visit for the first patient and the two-month follow-up visit for the seventh patient enrolled in its Deltacel-01 Phase 1 clinical trial, and provides an enrollment update. This trial is evaluating Deltacel™ (KB-GDT-01), the Company’s allogeneic, off-the-shelf, Gamma Delta T-cell (GDT) therapy, in patients with stage 4 metastatic or locally-advanced non-small cell lung cancer (NSCLC) who have failed to respond to standard therapies.
At the 12-month post-treatment follow-up visit, the first patient in Deltacel-01 had a 33.33% reduction in tumor volume compared with their pre-treatment tumor size, thereby achieving a partial response. This marks the second patient in the Deltacel-01 study with a partial response after our fourth patient. Additionally, the seventh patient had a 9.5% reduction in tumor size at their two-month follow-up visit. Both patients are being treated at the Beverly Hills Cancer Center (BHCC).
“The sustained, positive results we are seeing with the Deltacel-01 clinical trial are highly encouraging. Having a second patient achieve partial response with the first patient’s remarkable 33% tumor shrinkage at the 12-month follow-up highlights the therapeutic potential of our gamma-delta T cell therapy. The early response observed in the seventh patient further supports our confidence in this platform. We are expanding trial enrollment to expose more patients to the potential benefit of Deltacel while bolstering our clinical dataset,” said Pietro Bersani, Chief Executive Officer of Kiromic BioPharma.
"The remarkable 33% tumor reduction seen in the first and fourth patient at our center along with the encouraging 9.5% reduction in the seventh patient, are truly exciting results from the Deltacel-01 clinical trial. These data, coupled with the patients’ reports of improved energy and better quality of life, reinforce the potential of Kiromic's gamma delta T-cell therapy to deliver meaningful clinical benefit for patients with advanced lung cancer who have exhausted other treatment options,” said Dr. Afshin Eli Gabayan, Medical Oncologist, Medical Director, and Principal Investigator at BHCC. “As a leading cancer center focused on providing access to the most innovative therapies, we are proud to partner with Kiromic and look forward to continuing to enroll patients and generate additional evidence supporting Deltacel's promise as a transformative new treatment option."
The Eighth Patient Completes Treatment
The eighth patient successfully completed the Deltacel-01 treatment regimen and is tolerating therapy well. Initial efficacy results for this patient are expected in late February 2025. This patient was enrolled at the Clinical Research Advisors Koreatown, a satellite location of BHCC.
Kiromic also announces that the ninth patient in Deltacel-01 started treatment at Virginia Oncology Associates (Norfolk, VA). Additionally, the company expects to enroll the 10th and 11th patients into the trial by the end of January.
About Deltacel-01
In Kiromic’s open-label Phase 1 clinical trial, titled “Phase 1 Trial Evaluating the Safety and Tolerability of Gamma Delta T Cell Infusions in Combination With Low Dose Radiotherapy in Subjects With Stage 4 Metastatic Non-Small Cell Lung Cancer” (NCT06069570), patients with advanced NSCLC receive three intravenous infusions of Deltacel™ with six courses of low-dose, localized radiation over a 31-day period. The primary objective of Deltacel-01 is to evaluate safety, while secondary measurements include objective response, progression-free survival, overall survival, time to progression, time to treatment response and disease control rates.
About Deltacel™
Deltacel™ (KB-GDT-01) is an investigational gamma delta T-cell (GDT) therapy currently in the Deltacel-01 Phase 1 trial for the treatment of stage 4 metastatic NSCLC. An allogeneic product consisting of unmodified, donor-derived gamma delta T cells, Deltacel™ is the leading candidate in Kiromic’s GDT platform. Deltacel™ is designed to exploit the natural potency of GDT cells to target solid cancers, with an initial clinical focus on NSCLC, which represents about 80% to 85% of all lung cancer cases. Data from two preclinical studies demonstrated Deltacel™’s favorable safety and efficacy profile when it was combined with low-dose radiation.
About the Beverly Hills Cancer Center
As a private, academic, community-based cancer center, the Beverly Hills Cancer Center not only provides the latest state-of-the-art cancer treatments all under one roof, but also provides leading clinical trials and research, attracting patients globally. By providing access to groundbreaking clinical trials, the Beverly Hills Cancer Center offers patients the opportunity to participate in the most advanced cancer treatments currently in development in the world. Beverly Hills Cancer Center is comprised of an internationally recognized multidisciplinary medical team consisting of medical oncologists, radiation oncologists, radiologists, hematologists and internists who provide exceptional patient care and support services including a robust and highly efficient team of clinical research professionals. More information is available at www.BHCancerCenter.com.
About Clinical Research Advisors LLC
Founded in 2022 by current researchers and technology entrepreneurs at Beverly Hills Cancer Center, Clinical Research Advisors is a first-of-its-kind clinical trial optimization company harnessing the power of AI and real-world data capitalizing on the decade success of the high-quality clinical trial program developed at its main site, Beverly Hills Cancer Center, established over 15 years ago. Having a central site makes us different than other site networks. We strive to accelerate the development of new treatments and cures by addressing major roadblocks in patient recruitment and site activation. By leveraging our central site, Beverly Hills Cancer Center, integrated network of growing satellite sites and advanced technologies, we aim to make clinical research participation more accessible and efficient. More information is available at www.ClinicalResearchAdvisors.com
About Kiromic BioPharma
Kiromic BioPharma, Inc. is a clinical-stage, fully integrated biotherapeutics company developing a multi-indication allogeneic cell therapy platform that exploits the natural potency of Gamma Delta T-cells to target solid tumors. Kiromic is using its proprietary DIAMOND® artificial intelligence (AI) 2.0 platform to discover novel targets for immuno-oncology. The Company maintains offices in Houston, Texas. To learn more, visit www.kiromic.com and connect with us on Twitter and LinkedIn.
Forward-Looking Statements
This press release contains forward-looking statements that involve substantial risks and uncertainties. All statements other than statements of historical facts are forward-looking statements. In some cases, you can identify forward-looking statements by terms such as: “will,” “potential,” “could,” “can,” “believe,” “intends,” “continue,” “plans,” “expects,” “anticipates,” “estimates,” “may,” or the negative of these terms or other comparable terminology. These forward-looking statements include, but are not limited to, statements regarding: Kiromic’s ability to achieve its objectives and Kiromic’s financing strategy and availability of funds. These forward-looking statements involve known and unknown risks, uncertainties and other factors that may cause actual results, levels of activity, performance, or achievements to be materially different from the information expressed or implied expressed or implied by these forward-looking statements. These risks and uncertainties include, but are not limited to, the risks and uncertainties discussed in our Annual Report on Form 10-K for the year ended December 31, 2023, and as detailed from time to time in our other SEC filings. You should not rely upon forward-looking statements as predictions of future events. Although we believe that the expectations reflected in the forward-looking statements are reasonable, we cannot guarantee that the future results, levels of activity, performance, or events and circumstances reflected in the forward-looking statements will be achieved or occur. Moreover, neither we nor any other person assumes responsibility for the accuracy and completeness of the forward-looking statements. Such forward-looking statements relate only to events as of the date of this press release. We undertake no obligation to update any forward-looking statements except to the extent required by law.
View source version on businesswire.com: https://www.businesswire.com/news/home/20250121548136/en/
Alliance Advisors IR Tirth T. Patel tpatel@allianceadvisors.com 212-201-6614
Beverly Hills Cancer Center Sharon Neman, MBA Chief Strategy Officer SN@bhcancercenter.com 310-432-8925
Clinical Research Advisors LLC Ali Muhammad, MD, MBA Co-Founder & Director of Clinical Research Operations AMuhammad@BHCancerCenter.com Ali@ClinicalResearchAdvisors.com 310-432-8934
Source: Kiromic BioPharma, Inc.
Cell TherapyPhase 1Clinical ResultImmunotherapyRadiation Therapy
12 Dec 2024
HOUSTON--(
BUSINESS WIRE
)--
Kiromic BioPharma, Inc. (OTCQB: KRBP) (“Kiromic” or the “Company”)
reports favorable ongoing efficacy results from the eight-month follow-up visit for the fourth patient enrolled in its Deltacel-01 Phase 1 clinical trial, and provides additional updates on the first and seventh patients. This trial is evaluating Deltacel
™
(KB-GDT-01), the Company’s allogeneic, off-the-shelf, Gamma Delta T-cell (GDT) therapy, in patients with stage 4 metastatic non-small cell lung cancer (NSCLC) who have failed to respond to standard therapies.
8-Month Follow-Up for Patient #4: Partial Response with Tumor Reduction of 32%
Preliminary results from the eight-month follow-up visit for the fourth patient enrolled in Deltacel-01 revealed an approximately 32% decrease in tumor volume compared with the pre-treatment size. This patient continues to experience clinical benefit without adverse events.
11-Month Follow-Up for Patient #1: Stable Disease Maintained
The first patient enrolled in the Deltacel-01 trial has maintained stable disease with no evidence of disease progression or new sites of malignancy. Kiromic last reported that in this patient, the tumor size was reduced by approximately 27% compared with the pre-treatment size, and no new sites of disease were identified. As a result, the PFS has reached 11 months with no reported adverse events. This patient's final follow-up visit is scheduled for the end of December.
Patient #7 Completes Treatment
The seventh patient successfully completed the Deltacel-01 treatment regimen and is tolerating therapy well. Initial efficacy results for this patient are expected in early January 2025.
Patient #8 Enrolled
The eighth patient in the Deltacel-01 clinical study was enrolled this week at the Clinical Research Advisors Koreatown, a satellite location of the Beverly Hills Cancer Center (BHCC).
“The magnitude of the tumor reduction observed in Patient #4 is significant and highly encouraging. We look forward to reporting results from the first and seventh patients in January, and expect to enroll additional patients through the beginning of 2025,” said Pietro Bersani, Chief Executive Officer of Kiromic BioPharma.
"The remarkable 32% tumor reduction seen in the fourth patient treated with Deltacel is truly exciting and holds great promise for improving outcomes for patients with advanced lung cancer. As a leading cancer center focused on delivering the most innovative and effective therapies, we are proud to partner with Kiromic on this important clinical trial. The early safety and tolerability data, coupled with these signs of robust antitumor activity, suggest Deltacel’s promise as a transformative new treatment option. We look forward to continued enrollment and results that could change the standard of care for these patients who have exhausted other options," said Dr. Afshin Eli Gabayan, Medical Oncologist, Medical Director, and Principal Investigator at Beverly Hills Cancer Center. “At the Beverly Hills Cancer Center, our mission is to provide our patients with access to the most advanced and cutting-edge cancer treatments available. By working with visionary companies like Kiromic, we are able to offer our patients the opportunity to participate in groundbreaking clinical trials that have the potential to transform cancer care. We look forward to continuing to support the Deltacel-01 trial and reporting on the progress of the additional patients enrolled at our center. Together, we are making important strides in the fight against this devastating disease."
About Deltacel-01
In Kiromic’s open-label Phase 1 clinical trial, titled “Phase 1 Trial Evaluating the Safety and Tolerability of Gamma Delta T Cell Infusions in Combination With Low Dose Radiotherapy in Subjects With Stage 4 Metastatic Non-Small Cell Lung Cancer” (
NCT06069570
), patients with stage 4 NSCLC will receive two intravenous infusions of Deltacel
™
with four courses of low-dose, localized radiation over a 10-day period. The primary objective of Deltacel-01 is to evaluate safety, while secondary measurements include objective response, progression-free survival, overall survival, time to progression, time to treatment response and disease control rates.
About Deltacel
™
Deltacel
™
(KB-GDT-01) is an investigational gamma delta T-cell (GDT) therapy currently in the Deltacel-01 Phase 1 trial for the treatment of stage 4 metastatic NSCLC. An allogeneic product consisting of unmodified, donor-derived gamma delta T cells, Deltacel
™
is the leading candidate in Kiromic’s GDT platform. Deltacel
™
is designed to exploit the natural potency of GDT cells to target solid cancers, with an initial clinical focus on NSCLC, which represents about 80% to 85% of all lung cancer cases. Data from two preclinical studies demonstrated Deltacel
™
’s favorable safety and efficacy profile when it was combined with low-dose radiation.
About the Beverly Hills Cancer Center
As a private, academic, community-based cancer center, the Beverly Hills Cancer Center not only provides the latest state-of-the-art cancer treatments all under one roof, but also provides leading clinical trials and research, attracting patients globally. By providing access to groundbreaking clinical trials, the Beverly Hills Cancer Center offers patients the opportunity to participate in the most advanced cancer treatments currently in development in the world. Beverly Hills Cancer Center is comprised of an internationally recognized multidisciplinary medical team consisting of medical oncologists, radiation oncologists, radiologists, hematologists and internists who provide exceptional patient care and support services including a robust and highly efficient team of clinical research professionals. More information is available at
www.BHCancerCenter.com
.
About Clinical Research Advisors LLC
Founded in 2022 by current researchers and technology entrepreneurs at Beverly Hills Cancer Center, Clinical Research Advisors is a first-of-its-kind clinical trial optimization company harnessing the power of AI and real-world data capitalizing on the decade success of the high-quality clinical trial program developed at it's main site, Beverly Hills Cancer Center, established over 15 years ago. Having a central site makes us different than other site networks. We strive to accelerate the development of new treatments and cures by addressing major roadblocks in patient recruitment and site activation. By leveraging our central site, Beverly Hills Cancer Center, integrated network of growing satellite sites and advanced technologies, we aim to make clinical research participation more accessible and efficient. More information is available at
www.ClinicalResearchAdvisors.com
About Kiromic BioPharma
Kiromic BioPharma, Inc. is a clinical-stage, fully integrated biotherapeutics company developing a multi-indication allogeneic cell therapy platform that exploits the natural potency of Gamma Delta T-cells to target solid tumors. Kiromic is using its proprietary DIAMOND
®
artificial intelligence (AI) 2.0 platform to discover novel targets for immuno-oncology. The Company maintains offices in Houston, Texas. To learn more, visit
www.kiromic.com
and connect with us on
Twitter
and
LinkedIn
.
Forward-Looking Statements
This press release contains forward-looking statements that involve substantial risks and uncertainties. All statements other than statements of historical facts are forward-looking statements. In some cases, you can identify forward-looking statements by terms such as: “will,” “potential,” “could,” “can,” “believe,” “intends,” “continue,” “plans,” “expects,” “anticipates,” “estimates,” “may,” or the negative of these terms or other comparable terminology. These forward-looking statements include, but are not limited to, statements regarding: Kiromic’s ability to achieve its objectives and Kiromic’s financing strategy and availability of funds. These forward-looking statements involve known and unknown risks, uncertainties and other factors that may cause actual results, levels of activity, performance, or achievements to be materially different from the information expressed or implied expressed or implied by these forward-looking statements. These risks and uncertainties include, but are not limited to, the risks and uncertainties discussed in our Annual Report on Form 10-K for the year ended December 31, 2023, and as detailed from time to time in our other SEC filings. You should not rely upon forward-looking statements as predictions of future events. Although we believe that the expectations reflected in the forward-looking statements are reasonable, we cannot guarantee that the future results, levels of activity, performance, or events and circumstances reflected in the forward-looking statements will be achieved or occur. Moreover, neither we nor any other person assumes responsibility for the accuracy and completeness of the forward-looking statements. Such forward-looking statements relate only to events as of the date of this press release. We undertake no obligation to update any forward-looking statements except to the extent required by law.
Phase 1Clinical ResultCell TherapyImmunotherapyRadiation Therapy
100 Deals associated with
Login to view more data
100 Translational Medicine associated with
Login to view more data
Corporation Tree
Boost your research with our corporation tree data.
login
or
Pipeline
Pipeline Snapshot as of 20 Dec 2025
No data posted
Login to keep update
Deal
Boost your decision using our deal data.
login
or
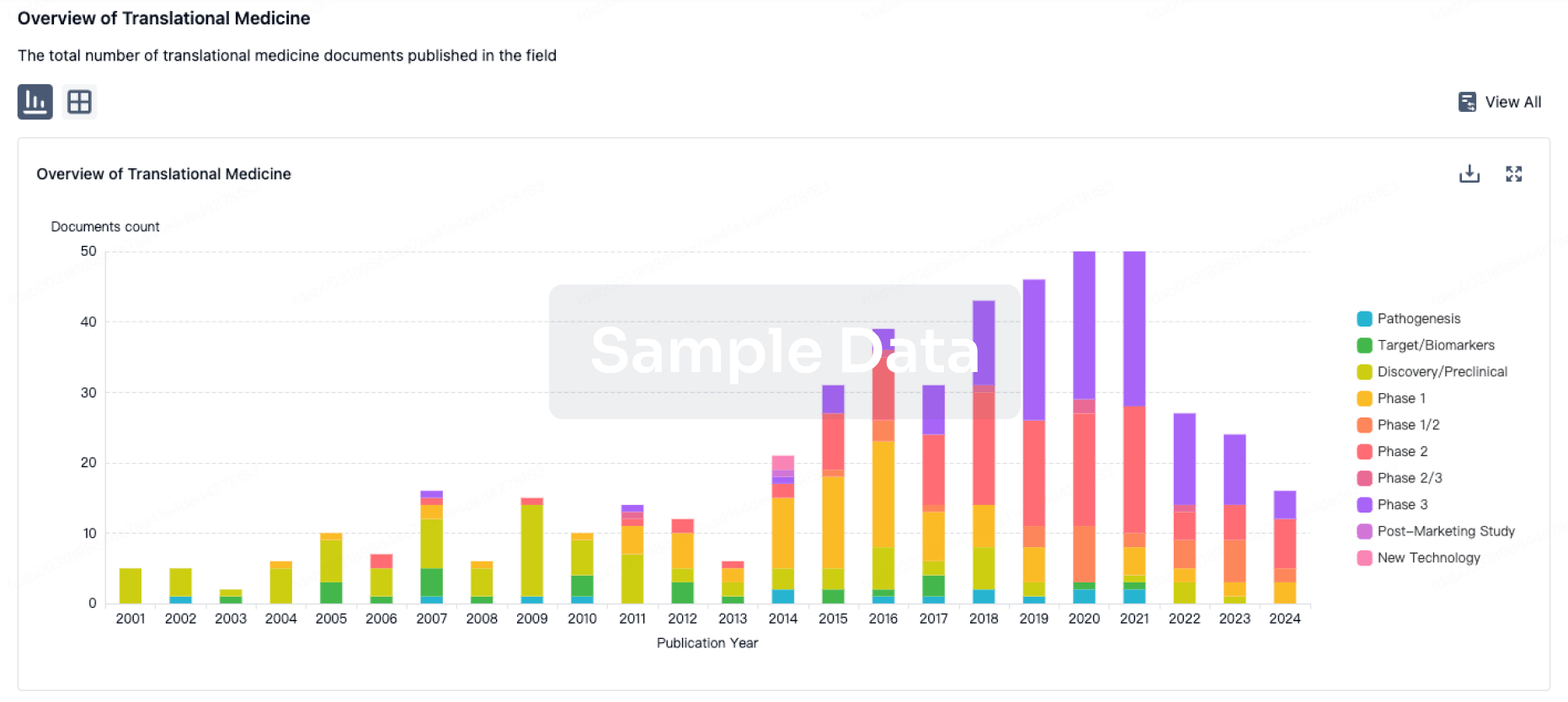
Translational Medicine
Boost your research with our translational medicine data.
login
or
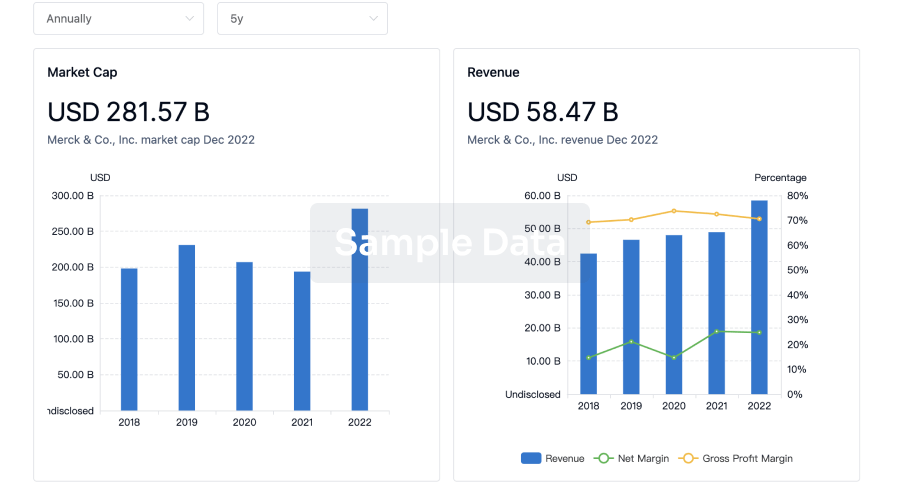
Profit
Explore the financial positions of over 360K organizations with Synapse.
login
or
Grant & Funding(NIH)
Access more than 2 million grant and funding information to elevate your research journey.
login
or

Investment
Gain insights on the latest company investments from start-ups to established corporations.
login
or
Financing
Unearth financing trends to validate and advance investment opportunities.
login
or
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free