Request Demo
Last update 08 May 2025
The Ohio State University College of Pharmacy
Last update 08 May 2025
Overview
Related
100 Clinical Results associated with The Ohio State University College of Pharmacy
Login to view more data
0 Patents (Medical) associated with The Ohio State University College of Pharmacy
Login to view more data
284
Literatures (Medical) associated with The Ohio State University College of Pharmacy01 May 2025·Research in Social and Administrative Pharmacy
Return on investment of pharmacists’ services among non-hospitalized patients: A scoping review
Review
Author: Murphy, E Michael ; Almodovar, Armando Silva ; Blankenship, Bella ; Miller, Julia ; Trombetta, Mallory
21 Apr 2025·Cancer Research
Abstract 2296: Ascertainment of uterine cancer surgery in the Surveillance, Epidemiology, End Results (SEER)-Medicare linked database: Comparison of SEER and claims data
Author: Padamsee, Tasleem J. ; Doll, Kemi M. ; Vable, Anusha M. ; Sinnott, Jennifer A. ; Felix, Ashley S. ; Hu, Qinhan ; Donneyong, Marcarius ; Meade, Caitlin E.
16 Apr 2025·American Journal of Health-System Pharmacy
Effectiveness of rasburicase 4.5 mg in the treatment of tumor lysis syndrome–related hyperuricemia
Article
Author: Eisinger, Gregory ; Shirk, Mary Beth ; Schlueter, Callahan ; Stojova, Emilija ; Rozycki, Elizabeth ; Westfield, Jaelyn
1
News (Medical) associated with The Ohio State University College of Pharmacy21 Oct 2022
LOS ANGELES, Oct. 21, 2022 /PRNewswire/ -- Kroger/Ralphs, as part of Kroger Health, and Cardinal Health will be working together again to host their annual drug take back events at more than 150 local pharmacy locations across the country. These events will take place on Saturday, October 29, the Drug Enforcement Administration's National Prescription Drug Take Back Day.
In recent years, the rate of U.S. adults taking prescription drugs has steadily increased, with the most recent data from the Health Policy Institute showing about 66% of U.S. adults are taking prescription drugs1. With these increases in prescription drug usage, misuse of expired or unused medications is always a concern.
"Ralphs Pharmacy is beyond excited to once again collaborate with Cardinal Health and local law enforcement agencies to provide anonymous, safe and convenient locations to safely dispose of any unused or expired prescription drugs," said Dr. Linh Lee, Pharm.D., Director of Pharmacy for Ralphs. "This step is one we can all take to help strengthen our communities and help people live healthier lives."
"At Cardinal Health, it's always a priority for us to help lead the fight against prescription medication misuse," said Jessie Cannon, vice president of community relations at Cardinal Health. "We are honored to work with like-minded organizations such as Kroger Health/Ralphs who are committed to improving the health of our communities and reducing prescription medication misuse. By providing centralized locations for community members to dispose of medication safely, we are helping keep our communities safe."
The Drug Take Back event ladders up to Cardinal Health's Generation Rx program, an evidence-informed prevention education program which offers age-appropriate resources to teach others about using medications safely. Generation Rx was founded at The Ohio State University College of Pharmacy and has been powered through a partnership with Cardinal Health since 2009.
In the Southern California area, drug take back events are scheduled from 10 a.m. to 2 p.m. Local law enforcement officers will be on site to accept unused, unwanted or expired pills, liquids, gels, over-the-counter (OTC) medications and patches (no medications will be accepted inside stores).
Ralphs locations hosting the event include:
Ralphs #21 located at 1745 Garfield Avenue, South Pasadena, CA 91030
Ralphs #147 located at 27760 N. McBean Parkway, Valencia, CA 91354
Ralphs #284 located at 10772 Jefferson Boulevard, Culver City, CA 90230
Ralphs #604 located at 12470 Seal Beach Boulevard, Seal Beach, CA 90740
Every day, Kroger Health/Ralphs pharmacists are available at store locations to educate customers about proper medication use and disposal. In-store pharmacies also offer naloxone – the life-saving medication that helps reverse opioid overdose – and free DisposeRx at-home disposal packets for customers with qualifying prescriptions.
During the events, Kroger Health/Ralphs pharmacy associates will distribute free reusable totes with DisposeRx at-home medication disposal packets, mental health resources and Generation Rx materials (note: quantities are limited).
Cardinal Health has joined Kroger Health in hosting drug take back events across the U.S. for several years. More than 115,000 pounds of unused prescription drugs have been collected for safe disposal during these events. To view the complete list of Kroger Health drug take back event locations across the country, visit Kroger.com.
About Ralphs
Ralphs Grocery Company is dedicated to our purpose: to
Feed the Human Spirit™. We are more than 18,000 associates serving customers in 184 supermarkets across Southern California. From the company's headquarters in Los Angeles County, Ralphs is a recognized leader in community service and giving. The company supports Kroger's Zero Hunger | Zero Waste initiative aimed at ending hunger in our communities and eliminating waste within our company by the year 2025. Ralphs is a subsidiary of The Kroger Co., (NYSE:KR), one of the world's largest retailers, based in Cincinnati, Ohio. For more about Ralphs, please visit our website at .
About Kroger Health:
Kroger Health, the healthcare division of The Kroger Co., is one of America's leading retail healthcare organizations, with over 2,200 pharmacies and 220 clinics in 35 states serving more than 14 million customers. Our team of 22,000 healthcare practitioners - from pharmacists and nurse practitioners to dietitians and technicians – are committed to helping people live healthier lives. We believe in practicing at the top of our licenses and enabling "food as medicine" to help prevent or manage certain diseases. For more information, visit .
About Cardinal Health
Cardinal Health is a distributor of pharmaceuticals, a global manufacturer and distributor of medical and laboratory products, and a provider of performance and data solutions for health care facilities. With 50 years in business, operations in more than 30 countries and approximately 46,500 employees globally, Cardinal Health is essential to care. Information about Cardinal Health is available at cardinalhealth.com.
1 Prescription drugs. Health Policy Institute. (2019, February 13). Retrieved September 8, 2022, from
SOURCE Ralphs Grocery Company
Collaborate
100 Deals associated with The Ohio State University College of Pharmacy
Login to view more data
100 Translational Medicine associated with The Ohio State University College of Pharmacy
Login to view more data
Corporation Tree
Boost your research with our corporation tree data.
login
or
Pipeline
Pipeline Snapshot as of 07 Dec 2025
No data posted
Login to keep update
Deal
Boost your decision using our deal data.
login
or
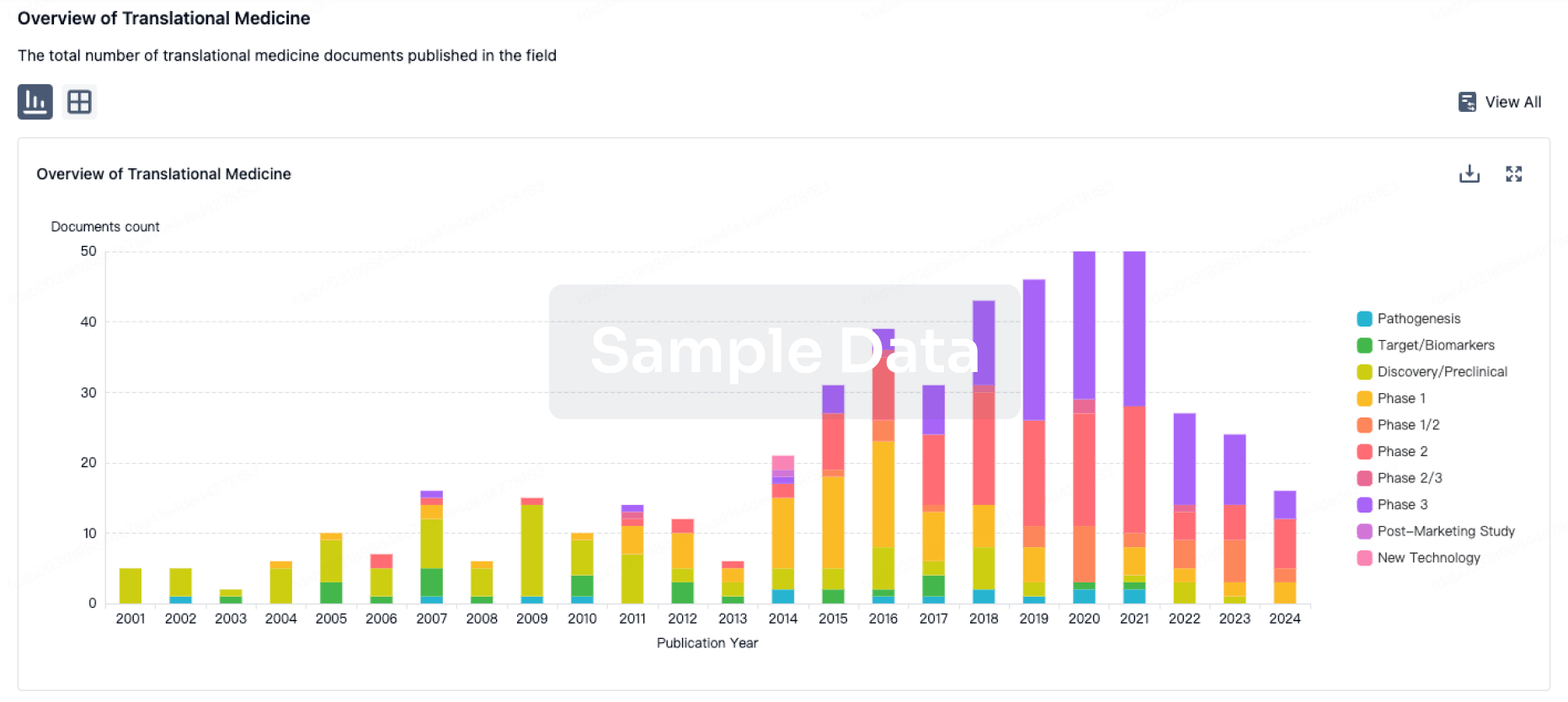
Translational Medicine
Boost your research with our translational medicine data.
login
or
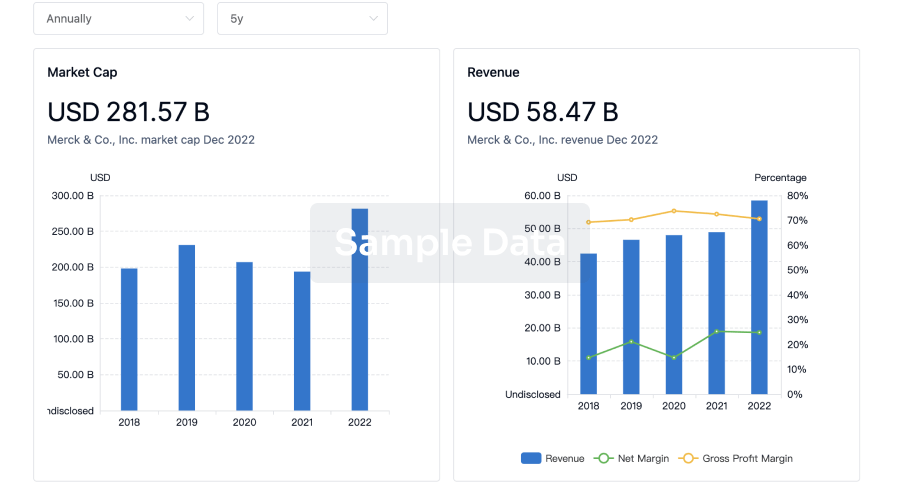
Profit
Explore the financial positions of over 360K organizations with Synapse.
login
or
Grant & Funding(NIH)
Access more than 2 million grant and funding information to elevate your research journey.
login
or

Investment
Gain insights on the latest company investments from start-ups to established corporations.
login
or
Financing
Unearth financing trends to validate and advance investment opportunities.
login
or
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free