Last update 09 Dec 2024
Beth Israel Deaconess Medical Center
Last update 09 Dec 2024
Overview
Tags
Immune System Diseases
Infectious Diseases
Urogenital Diseases
Monoclonal antibody
Disease domain score
A glimpse into the focused therapeutic areas

Technology Platform
Most used technologies in drug development
Targets
Most frequently developed targets
Related
Target |
Mechanism |
Active Org. |
Originator Org. |
Active Indication |
Inactive Indication |
Drug Highest Phase |
First Approval Ctry. / Loc. |
First Approval Date |

100 Clinical Results associated with Beth Israel Deaconess Medical Center
Login to view more data
Login to view more data
01 Mar 2025JPRAS open
From Novel Facial Measurements to Facial Implantology: A Systematic Review
Review
Author: Knoedler, Leonard ; Remy, Katya ; Sherwani, Khalil ; Kauke-Navarro, Martin ; Scheiflinger, Alexandra ; Baecher, Helena ; Deniz, Can ; Straub, Niklas ; Knoedler, Samuel ; Heiland, Max ; Maheta, Bhagvat ; Safi, Ali-Farid
Background:
Facial implants have emerged as pivotal tools for both reconstructive and aesthetic skull bone augmentation. Contemporary manufacturing techniques, such as computer-aided design and manufacturing (CAD-CAM) systems, have revolutionized facial implants production, providing the advantages of high-level individualization. However, the absence of standardized facial measurements complicates the ability to accurately compare outcomes across various techniques. This systematic review investigates the strengths and limitations of various facial measurements employed in facial implants, with a particular focus on their impact on aesthetic outcomes and potential complications.
Methods:
We identified 13 studies in our comprehensive search across PubMed/MEDLINE, Web of Science, EMBASE, and CENTRAL databases.
Results:
In total, 620 patients were included. The majority of the chosen studies focused on aesthetic purposes (69%). Primarily, mandibular (46%) or nasal regions (23%) were investigated, with porous polyethylene (31%), silicone (23%), and polyetheretherketone (23%) being the most utilized materials. Despite considerable heterogeneity in measurement approaches, including variations in reference points and angles, complications such as surgical site infections and nerve-related injuries were reported in the included studies.
Conclusion:
Our review highlights the importance of standardized facial analysis for optimal implant planning. Future research should prioritize the development of uniform measurement concepts tailored to diverse implant applications to enhance outcomes and patient satisfaction in facial implantation.
01 Feb 2025CARDIOLOGY CLINICS
Cardiotoxicity of Anthracyclines
Review
Author: Hoeger, Christopher W. ; Ariza, Abul ; Asnani, Aarti ; Balough, Elizabeth ; Hoeger, Christopher W
Anthracycline chemotherapy is associated with cardiotoxicity, predominantly manifesting as left ventricular systolic dysfunction within the first year of treatment. Early detection is possible through biomarkers and cardiovascular imaging before clinical symptoms develop. Comprehensive cardiovascular risk assessment is essential for all patients prior to anthracycline therapy to stratify their risk of cardiotoxicity. Preventive measures, including cardiovascular risk optimization, as well as anthracycline dose adjustments, the use of liposomal anthracyclines, and dexrazoxane in high-risk patients, are crucial to mitigate the risk of cardiotoxicity. Long-term follow-up and cardiovascular risk optimization are critical for cancer survivors to optimize cardiovascular outcomes.
01 Feb 2025Thoracic Surgery Clinics
Management of Tracheal Surgery Complications and Redo Tracheal Surgery
Review
Author: Wilson, Jennifer L. ; Mathew, Fleming ; Carpenter, Sandra L. ; Wilson, Jennifer L ; Gangadharan, Sidhu P ; Carpenter, Sandra L ; Gangadharan, Sidhu P.
Tracheal surgery is associated with low mortality but substantial morbidity. Major complications after tracheal and laryngotracheal resection and reconstruction may affect a significant percentage of patients. Anastomotic complications include granulations, dehiscence, and recurrent stenoses. Breakdown of the airway anastomosis may lead to catastrophic complications such as tracheoinnominate and tracheoesophageal fistulas. Nonanastomotic complications include recurrent laryngeal nerve injury, glottic dysfunction, and respiratory infections. This article discusses complications occurring after tracheal surgery and offers strategies for optimizing patient outcomes based on current evidence. The final sections provide a summary of best practices for redo tracheal surgery and current challenges.
100 Deals associated with Beth Israel Deaconess Medical Center
Login to view more data
100 Translational Medicine associated with Beth Israel Deaconess Medical Center
Login to view more data
Corporation Tree
Boost your research with our corporation tree data.
login
or
Pipeline
Pipeline Snapshot as of 29 Dec 2024
The statistics for drugs in the Pipeline is the current organization and its subsidiaries are counted as organizations,Early Phase 1 is incorporated into Phase 1, Phase 1/2 is incorporated into phase 2, and phase 2/3 is incorporated into phase 3
Preclinical
1
Login to view more data
Current Projects
Login to view more data
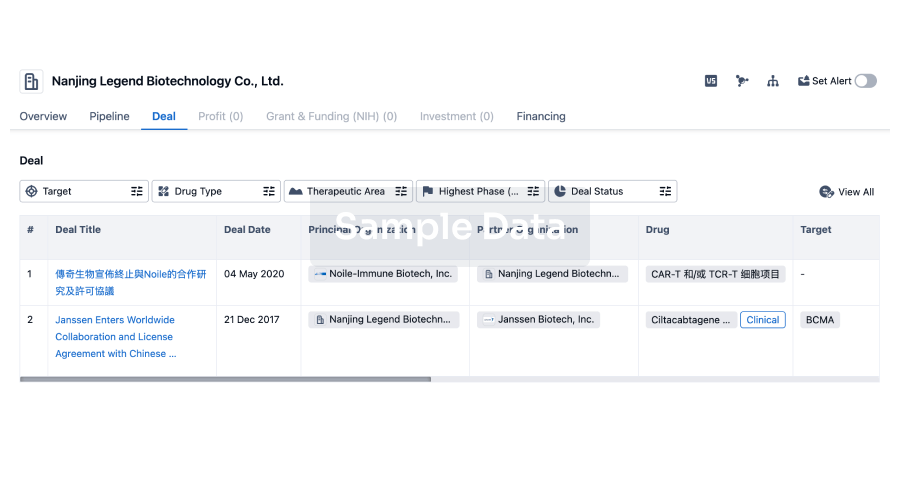
Deal
Boost your decision using our deal data.
login
or
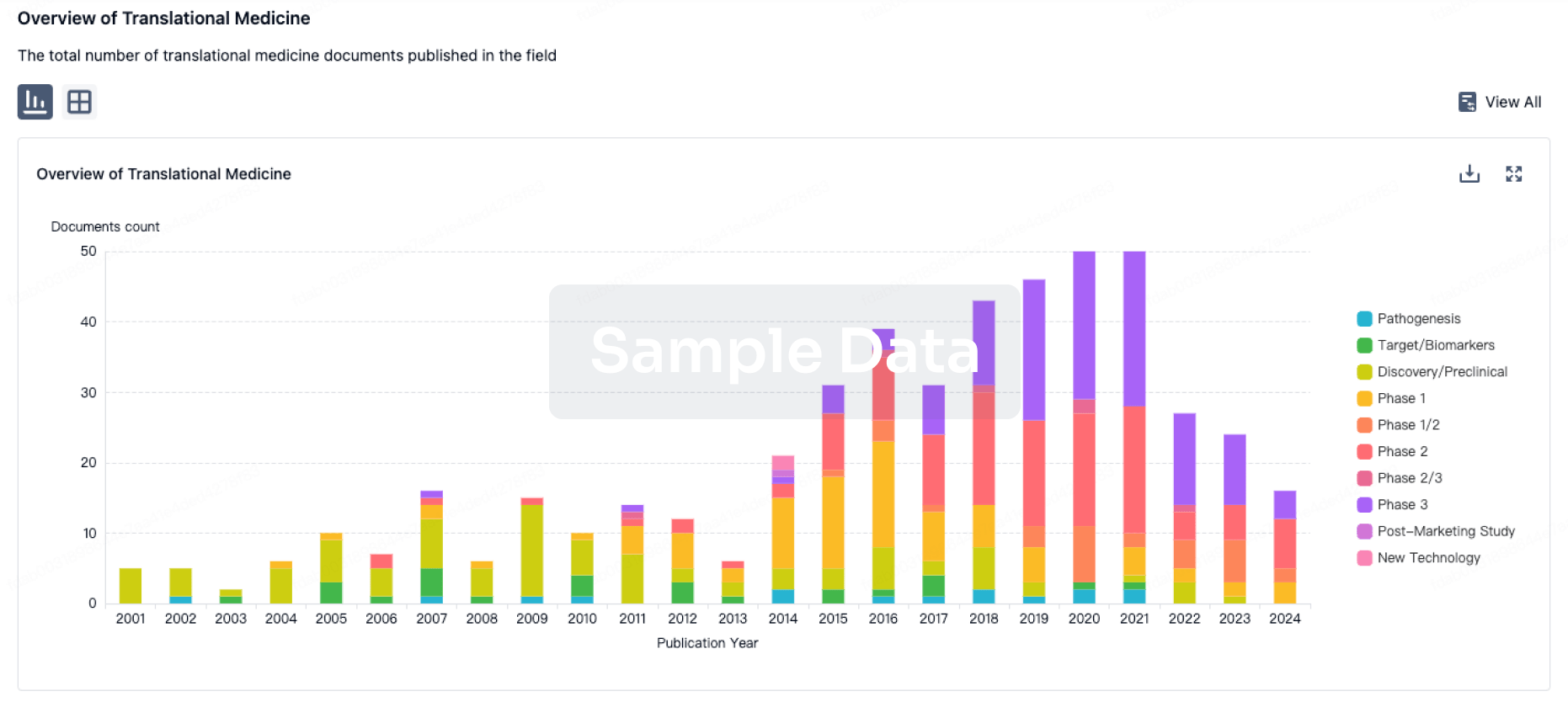
Translational Medicine
Boost your research with our translational medicine data.
login
or
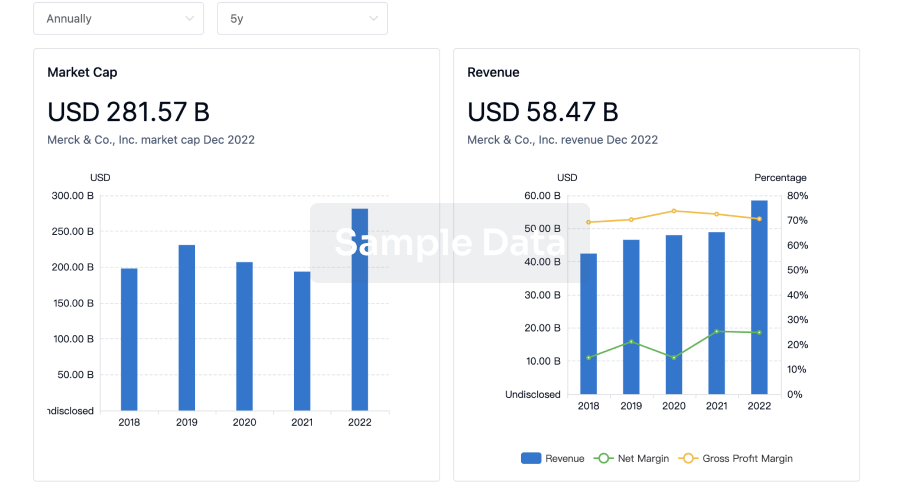
Profit
Explore the financial positions of over 360K organizations with Synapse.
login
or
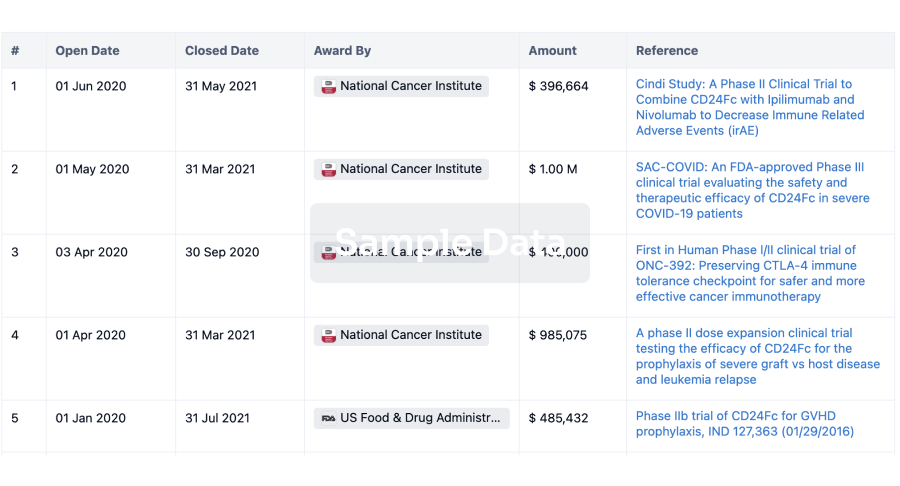
Grant & Funding(NIH)
Access more than 2 million grant and funding information to elevate your research journey.
login
or
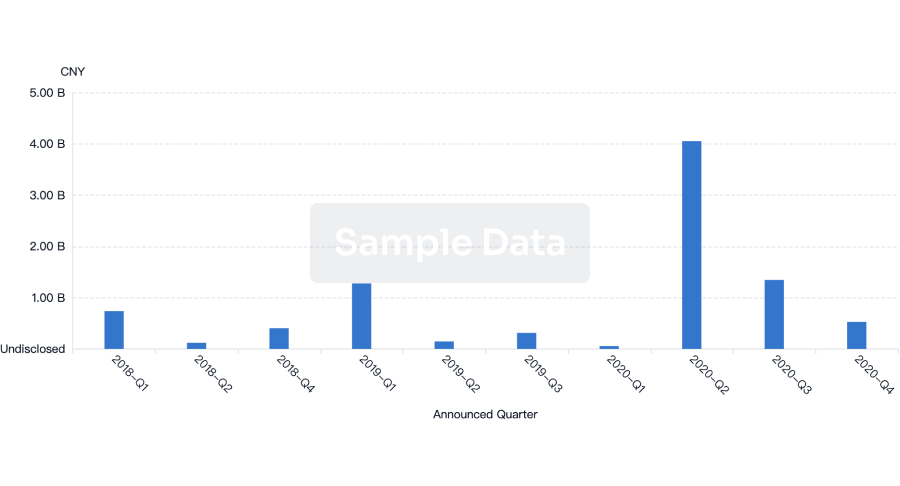
Investment
Gain insights on the latest company investments from start-ups to established corporations.
login
or

Financing
Unearth financing trends to validate and advance investment opportunities.
login
or
Chat with Hiro
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free