Last update 02 Oct 2024
Avatar Group
Last update 02 Oct 2024
Overview
Related
100 Clinical Results associated with Avatar Group
Login to view more data
Login to view more data
01 Mar 2021Supportive care in cancer : official journal of the Multinational Association of Supportive Care in CancerQ2 · MEDICINE
Inherent and modifiable risk factors for peripheral venous catheter failure during cancer treatment: a prospective cohort study
Q2 · MEDICINE
Article
Author: Marsh, Nicole ; O'Brien, Catherine ; Friese, Christopher ; Rickard, Claire M ; Larsen, Emily N ; Monteagle, Emily
PURPOSE:
To identify modifiable and non-modifiable risk factors for peripheral intravenous catheter (PIV) failure among patients requiring intravenous treatment for oncology and haematology conditions.
METHODS:
A single-centre prospective cohort study was conducted between October 2017 and February 2019. Adult in-patients requiring a PIV for therapy were prospectively recruited from two cancer units at a tertiary hospital in Queensland, Australia. The primary outcome was a composite of complications leading to PIV failure (local and bloodstream infection; occlusion; infiltration/extravasation; leakage; dislodgement; and/or phlebitis). Secondary outcomes were (i) PIV dwell time; (ii) insertion and (iii) failure of a CVAD; (iv) adverse events; (v) length of hospital stay. Outcomes were investigated using Bayesian multivariable linear regression modelling and survival analysis.
RESULTS:
Of 200 participants, 396 PIVs were included. PIV failure incidence was 34.9%; the most common failure type was occlusion/infiltration (n = 74, 18.7%), then dislodgement (n = 33, 8.3%), and phlebitis (n = 30, 7.6%). While several patient and treatment risk factors were significant in univariable modelling, in the final multivariable model, only the use of non-sterile tape (external to the primary dressing) was significantly associated with decreased PIV dislodgement (hazard ratio 0.06, 95% confidence interval 0.01, 0.48; p = 0.008).
CONCLUSION:
PIV failure rates among patients receiving cancer treatment are high, the sequelae of which may include delayed treatment and infection. Larger studies on risk factors and interventions to prevent PIV failure in this population are needed; however, the use of secondary securements (such as non-sterile tape) to provide further securement to the primary PIV dressing is particularly important.
TRIAL REGISTRATION:
Study methods were registered prospectively with the Australian New Zealand Clinical Trials Registry on the 27th March 2017 (ACTRN12617000438358); https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=372191&isReview=true.
01 Jun 2020PediatricsQ2 · MEDICINE
Developing Pediatric Appropriateness Criteria for Intravenous Catheters
Q2 · MEDICINE
Review
Author: Chopra, Vineet ; Ullman, Amanda
* Abbreviations:
IV — : intravenous
MAGIC — : Michigan Appropriateness Guide for Intravenous Catheters
miniMAGIC — : mini Michigan Appropriateness Guide for Intravenous Catheters
Consider this scenario: an 8-month-old infant with osteomyelitis needs intravenous (IV) access for 3 weeks of antibiotics; what device will best ensure successful therapy and low risk of complications? Or consider this: a teenager with cystic fibrosis is hospitalized for the third time this year with an acute exacerbation. Despite multiple efforts by experienced clinicians, an IV catheter cannot be successfully placed in a peripheral vein. Frustrated, the nurse says, “Let’s just put in a peripherally inserted central catheter.” Is this the best choice for the patient?
These scenarios, and many more like them, occur for hundreds of pediatric patients in hospitals every day. Yet, the approach to these decisions is far from consistent.1 Ask a provider why they choose a specific device or consult a certain specialist for an IV access procedure, and you may hear, “That’s how I have always done it,” or “This is how I was trained.” In part, these monocentric styles have evolved as a result of evidence gaps in pediatric vascular access. Compared with adult populations, the evidence base for risk, benefits, and alternatives of IV …
Address correspondence to Amanda Ullman, PhD, RN, Menzies Health Institute Queensland, Griffith University, Kessels Rd, Nathan, QLD4111, Australia. E-mail: a.ullman@griffith.edu.au
01 Jan 2020Journal of paediatrics and child healthQ4 · MEDICINE
Flushing of peripheral intravenous catheters: A pilot, factorial, randomised controlled trial of high versus low frequency and volume in paediatrics
Q4 · MEDICINE
Article
Author: Mihala, Gabor ; Schults, Jessica ; Kleidon, Tricia M ; Rickard, Claire M ; Flynn, Julie ; Keogh, Samantha
Aim:
To test the feasibility of an efficacy trial comparing different flushing frequencies and volumes to reduce peripheral intravenous cannula (PIVC) failure in paediatric inpatients.
Methods:
Pilot, 2 × 2 factorial, randomised controlled trial comparing PIVC flushing techniques in intervention pairs: (i) low volume (3 mL) versus high volume (10 mL); and (ii) low frequency (24 hourly) versus high frequency (6 hourly). Patients were excluded if: fluids were restricted, weight < 5 kg, PIVC already in situ for >24 h or continuous infusion. The primary end‐point was feasibility (eligibility, recruitment, retention, protocol adherence, missing data and sample size estimates) of a large trial. Secondary end‐points were PIVC failure (composite and individual), bloodstream infection and mortality.
Results:
A total of 919 children were screened from April to November 2015, with 55 enrolled. Screening feasibility criteria were not met, mainly due to continuous infusions and PIVCs in situ >24 h or planned for imminent removal. However, 80% of eligible participants consented, 2% withdrew, protocol adherence was 100%, and there was no missing primary end‐point data. PIVC failure was significantly higher (hazard ratio = 2.90, 95% confidence interval: 1.11–7.54) in the 3 mL compared to the 10 mL group. There was no difference in failure between frequency groups (hazard ratio = 0.91, 95% confidence interval: 0.36–2.33). There was no interaction effect (P = 0.22).
Conclusion:
Trial feasibility proved challenging due to eligibility criteria, which could be improved with additional recruiting staff. Firm conclusions cannot be made based on this small sample, but flush volume may impact PIVC failure.
01 Apr 2024
Cell TherapyAACRGene Therapy

100 Deals associated with Avatar Group
Login to view more data
100 Translational Medicine associated with Avatar Group
Login to view more data
Corporation Tree
Boost your research with our corporation tree data.
login
or
Pipeline
Pipeline Snapshot as of 06 Oct 2024
No data posted
Login to keep update
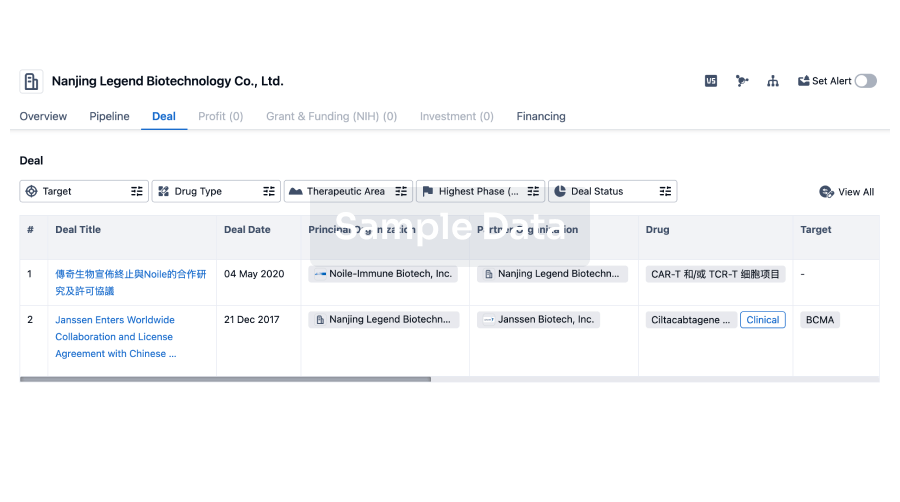
Deal
Boost your decision using our deal data.
login
or
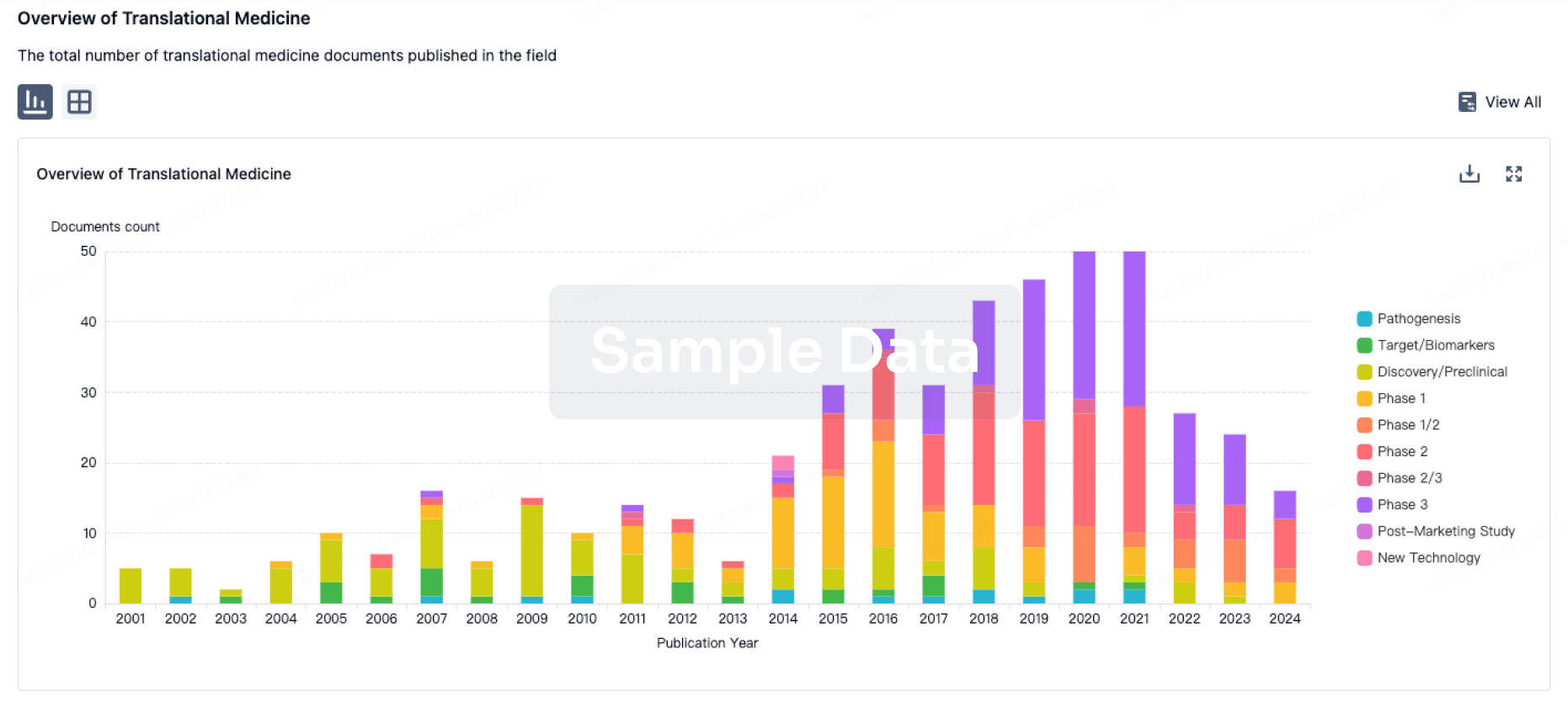
Translational Medicine
Boost your research with our translational medicine data.
login
or
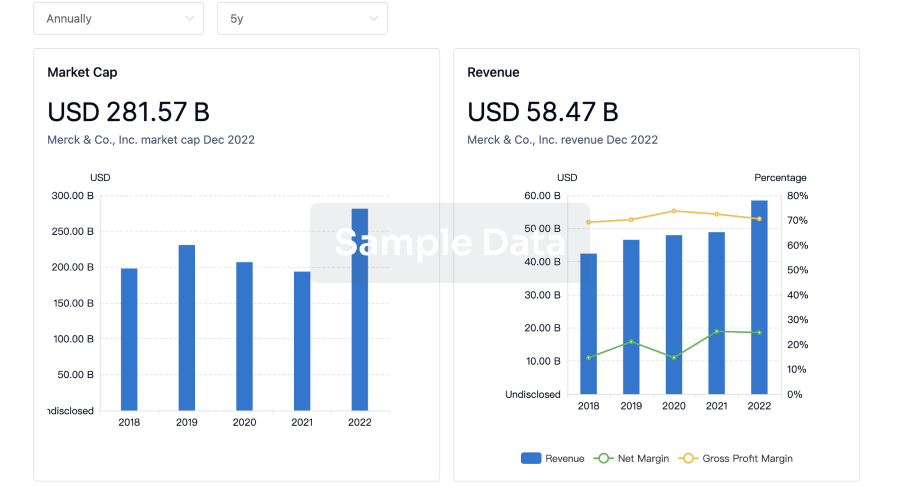
Profit
Explore the financial positions of over 360K organizations with Synapse.
login
or
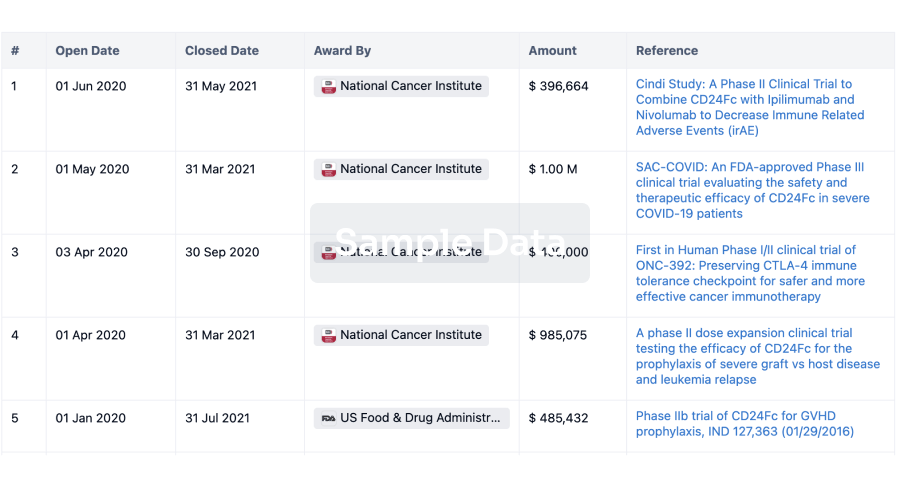
Grant & Funding(NIH)
Access more than 2 million grant and funding information to elevate your research journey.
login
or
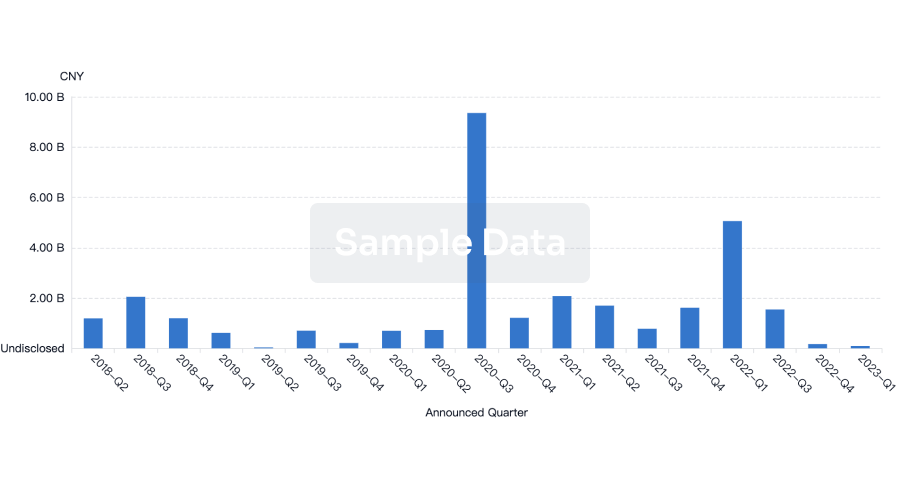
Investment
Gain insights on the latest company investments from start-ups to established corporations.
login
or
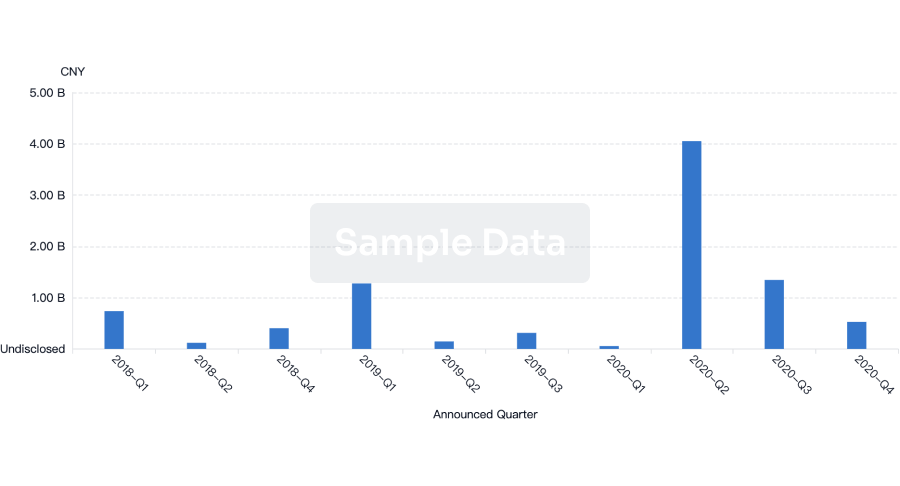
Financing
Unearth financing trends to validate and advance investment opportunities.
login
or
Chat with Hiro
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free