Last update 19 Sep 2024
Atlanta Heart Specialists LLC
Last update 19 Sep 2024
Overview
Related
100 Clinical Results associated with Atlanta Heart Specialists LLC
Login to view more data
0 Patents (Medical) associated with Atlanta Heart Specialists LLC
Login to view more data
1
Literatures (Medical) associated with Atlanta Heart Specialists LLC20 Nov 2012·Circulation
Abstract 318: Potential Primary Prevention Implantable Cardioverter-Defibrillator Patients Lack Understanding, Want More Information and Are Willing to Reconsider Implant Refusal
Author: Singh, Narendra ; Lucas, Essy ; Ramamurthy, Suresh ; Hall, Erin ; Chandra, Sandeep ; Yan, Linda ; Dorsey, Anthony ; Song, David ; Suh, David
1
News (Medical) associated with Atlanta Heart Specialists LLC14 Mar 2024
VALID-ECG Study will Form the Basis of the Company’s Upcoming FDA 510(k) Submission
SANTA CLARA, Calif.--(BUSINESS WIRE)-- HeartBeam, Inc. (NASDAQ: BEAT), a medical technology company focused on transforming cardiac care through the power of personalized insights, announced today that it has enrolled the first patients in the VALID-ECG (Clinical Validation of the AIMIGo 12-Lead ECG Synthesis Software for Arrhythmia Detection) pivotal study. The first patients were enrolled at Atlanta Heart Specialists, a top cardiology physician practice in Atlanta, GA.
The VALID-ECG study will evaluate the performance of a 12-lead ECG synthesized from its credit card-sized HeartBeam AIMIGo™ system compared to that of a standard hospital-based 12-lead ECG using both quantitative and qualitative methodologies for assessment of arrhythmias. HeartBeam AIMIGo leverages HeartBeam’s proprietary 3D vectorelectrocardiography (3D VECG) technology to capture signals in three projections (X, Y, Z) and synthesize a 12-lead ECG.
“We are thrilled to be part of this important study as AIMIGo represents a significant leap in cardiac monitoring technology. It brings the power of 3D VECG into a familiar 12-lead ECG waveform which is used to evaluate a range of cardiac conditions on a daily basis,” said David D. Suh, MD, FACC, Director of Research at Atlanta Heart Specialists. “The attractive, small form factor of AIMIGo makes it easy for patients to use the device whenever necessary. In addition, the clinical implications of 3D VECG technology could be potentially broad-ranging and extend to a variety of applications.”
More About the VALID-ECG Study and FDA Submissions
The VALID-ECG Study will enroll a total of 198 patients presenting with a variety of underlying cardiac conditions at up to five US sites. All patients enrolled in the study will receive simultaneously recorded ECGs from a standard 12-lead ECG machine and the HeartBeam AIMIGo system.
The primary objective of the study is to demonstrate the equivalence of ECG waveforms between the AIMIGo synthesized 12-lead ECG and a standard 12-lead ECG by analyzing key ECG parameters called amplitudes and intervals. The study will also examine the accuracy of physician diagnosis for various arrhythmias with the AIMIGo synthesized 12-lead ECG, compared to a standard 12-lead ECG.
HeartBeam’s 510(k) submission for the credit card-sized AIMIGo system is currently being reviewed by FDA. This application is for the entire 3D VECG system, which consists of the AIMIGo device, the patient application, the physician portal, and the wireless communications between them. The company expects that, when cleared, this would be the first FDA clearance for a handheld VECG system.
The VALID-ECG study will be a component of HeartBeam’s subsequent 510(k) submission, which will focus on the algorithms that take the 3D VECG signal and synthesize a 12-lead ECG, providing physicians with a visual representation of the gold standard ECG output. HeartBeam expects enrollment of the VALID-ECG study to be complete in Q2 2024.
“The initiation of the VALID-ECG study is a major milestone for the company and a reflection of our commitment to provide a strong foundation of clinical data as we strive to provide patients and physicians with the ability to accurately monitor cardiac disease outside of a medical facility,” said Branislav Vajdic, PhD, CEO and Founder of HeartBeam. “In addition, our product pipeline includes coupling AI with our data-rich 3D VECG technology which will enable us to extract unique information and longitudinal insights to transform how cardiac care is monitored in the future.”
The company has already completed an 80-patient pilot study using the same protocol as the VALID-ECG study. The company anticipates presenting the results of the pilot study at a scientific meeting in the second half of 2024. HeartBeam will also present data on its deep learning algorithm at two prestigious Electrophysiology conferences in Q2 2024.
About HeartBeam, Inc.
HeartBeam, Inc. (NASDAQ: BEAT) is a medical technology company that is dedicated to transforming cardiac care through the power of personalized insights. The company’s proprietary vectorelectrocardiography (VECG) technology collects 3D signals of the heart’s electrical activity and converts them into a 12-lead ECG. This platform technology is designed to be used on portable, patient-friendly devices such as a credit-card sized monitor, watch or patch. Physicians will be able to identify cardiac health trends and acute conditions and direct patients to the appropriate care – all outside of a medical facility, thus redefining how cardiac health is managed in the future. For additional information, visit HeartBeam.com.
Forward-Looking Statements
All statements in this release that are not based on historical fact are "forward-looking statements." While management has based any forward-looking statements included in this release on its current expectations, the information on which such expectations were based may change. Forward-looking statements involve inherent risks and uncertainties which could cause actual results to differ materially from those in the forward-looking statements, as a result of various factors including those risks and uncertainties described in the Risk Factors and in Management’s Discussion and Analysis of Financial Condition and Results of Operations sections of our Forms 10-K, 10-Q and other reports filed with the SEC and available at . We urge you to consider those risks and uncertainties in evaluating our forward-looking statements. We caution readers not to place undue reliance upon any such forward-looking statements, which speak only as of the date made. Except as otherwise required by the federal securities laws, we disclaim any obligation or undertaking to publicly release any updates or revisions to any forward-looking statement contained herein (or elsewhere) to reflect any change in our expectations with regard thereto or any change in events, conditions or circumstances on which any such statement is based.
Clinical Study
100 Deals associated with Atlanta Heart Specialists LLC
Login to view more data
100 Translational Medicine associated with Atlanta Heart Specialists LLC
Login to view more data
Corporation Tree
Boost your research with our corporation tree data.
login
or
Pipeline
Pipeline Snapshot as of 05 Oct 2024
No data posted
Login to keep update
Deal
Boost your decision using our deal data.
login
or
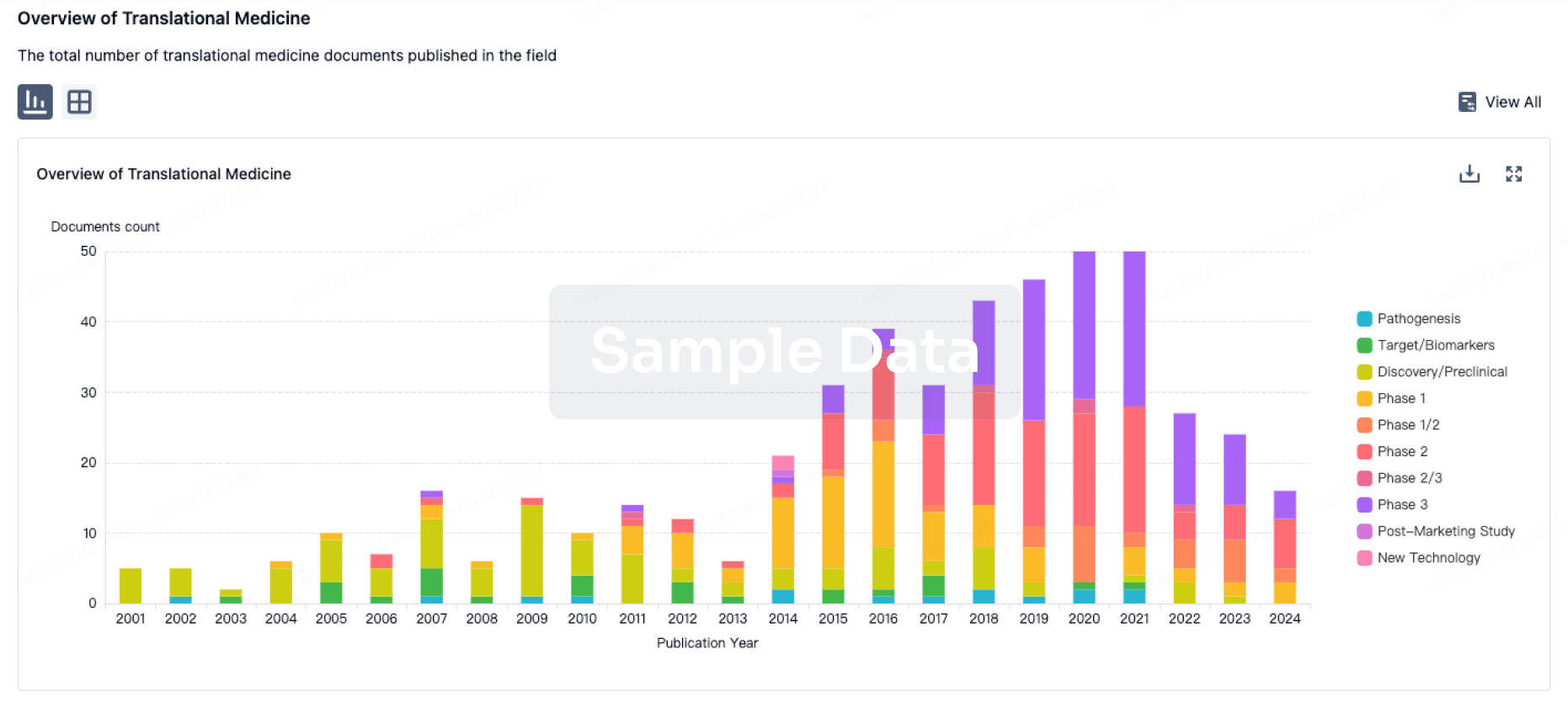
Translational Medicine
Boost your research with our translational medicine data.
login
or
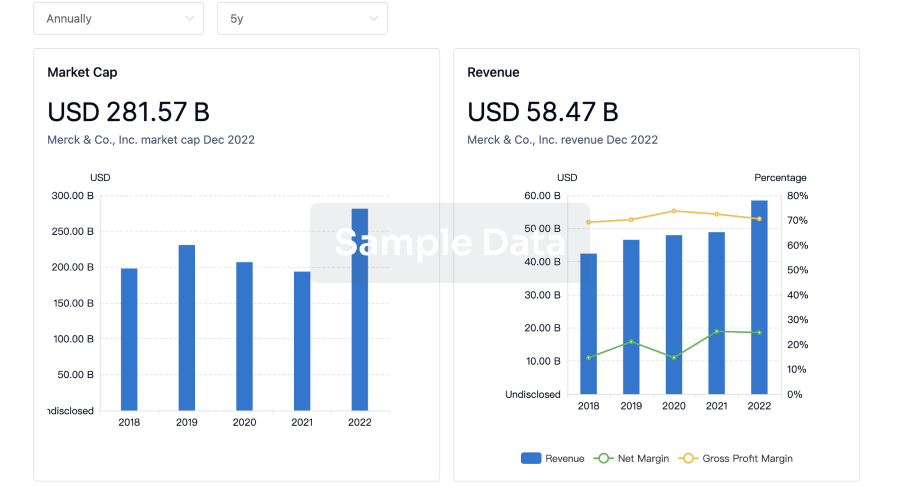
Profit
Explore the financial positions of over 360K organizations with Synapse.
login
or
Grant & Funding(NIH)
Access more than 2 million grant and funding information to elevate your research journey.
login
or
Investment
Gain insights on the latest company investments from start-ups to established corporations.
login
or
Financing
Unearth financing trends to validate and advance investment opportunities.
login
or
Chat with Hiro
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free