Request Demo
Last update 08 May 2025

Taab Biostudy Services
Last update 08 May 2025
Overview
Related
CTRI/2012/01/002340
A Multicentric, Comparative Controlled, Randomized, Parallel-Group, Phase III Study to Evaluate the Safety and Efficacy of FDC Containing Rosuvastatin Calcium and Telmisartan on Mild to Moderate Hypertension in Dyslipidemic Patients.

CTRI/2012/01/002334
A Multicentric, Comparative Controlled, Open Label, Randomized, Parallel-Group, Phase III Study to Evaluate the Safety and Efficacy of FDC containing Orlistat and Metformin with Metformin alone in Obese Type II Diabetic Patients.
CTRI/2011/10/002054
A Multicentric, Comparative Controlled, Open Label, Randomized, Parallel-Group, Phase III Study to Evaluate the Safety and Efficacy of FDC containing Montelukast plus Acebrophylline and Montelukast alone in Patients Suffering From Chronic Asthama
100 Clinical Results associated with Taab Biostudy Services
Login to view more data
Login to view more data
World Journal of Pharmaceutical Research
Evaluation of efficacy of teneligliptin by quantification with active glucagon like peptide-1 (GLP-1) from indian human plasma using novel bioanalytical method in LC-ESI-MS/MS
Author: Pal, Tapan Kumar ; Mandal, Pallab ; Chakraborty, Soumya ; Shaharyar, Adil Md. ; Karmakar, Sanmoy ; Mandal, Avishek ; Sarkar, Arnab ; Bhowmik, Rudranil
Materials Chemistry Frontiers
β-Cyclodextrin based pH and thermo-responsive biopolymeric hydrogel as a dual drug carrier
Author: Maity, Priti Prasanna ; Dhara, Santanu ; Bose, Anirbandeep ; Roy, Arpita ; Pal, Sagar
Herein, a novel biocompatible and stimuli-responsive network gel has been developed by grafting and crosslinking poly(
World Journal of Pharmaceutical Research
Evaluation of potentiality of antimicrobial activity of triazapentacyclo piperidine containing broad spectrum antibiotic rifabutin by minimal inhibitory concentration to treat Mycobacterium avium complex infection in HIV patient and quantification of pharmacokinetics parameters in Indian human plasma by liquid chromatography tandem quadruple mass spectrometry (API-4000)
Author: Saha, Chiranjit ; Karmakar, Sanmoy ; Mandal, Pallab ; Chakraborty, Soumya ; Pal, Tapan Kumar ; Chakraborty, Nilendra
100 Deals associated with Taab Biostudy Services
Login to view more data
100 Translational Medicine associated with Taab Biostudy Services
Login to view more data
Corporation Tree
Boost your research with our corporation tree data.
login
or
Pipeline
Pipeline Snapshot as of 16 Jul 2025
No data posted
Login to keep update
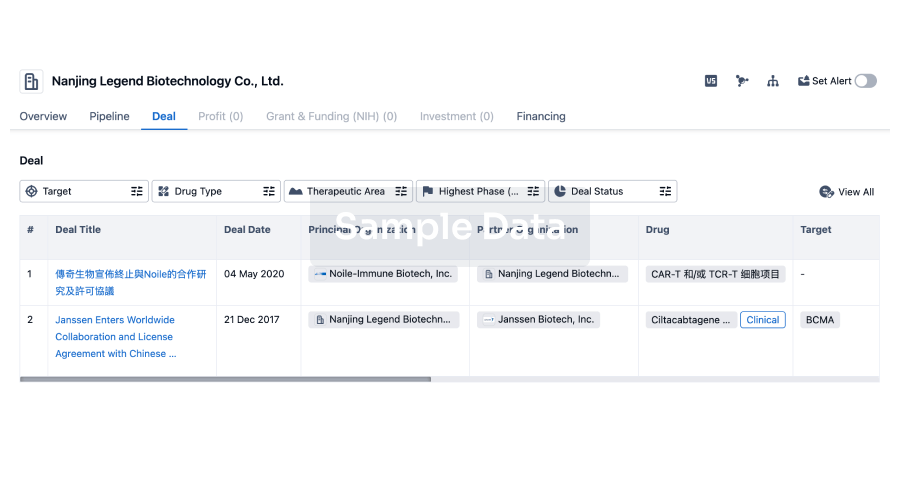
Deal
Boost your decision using our deal data.
login
or
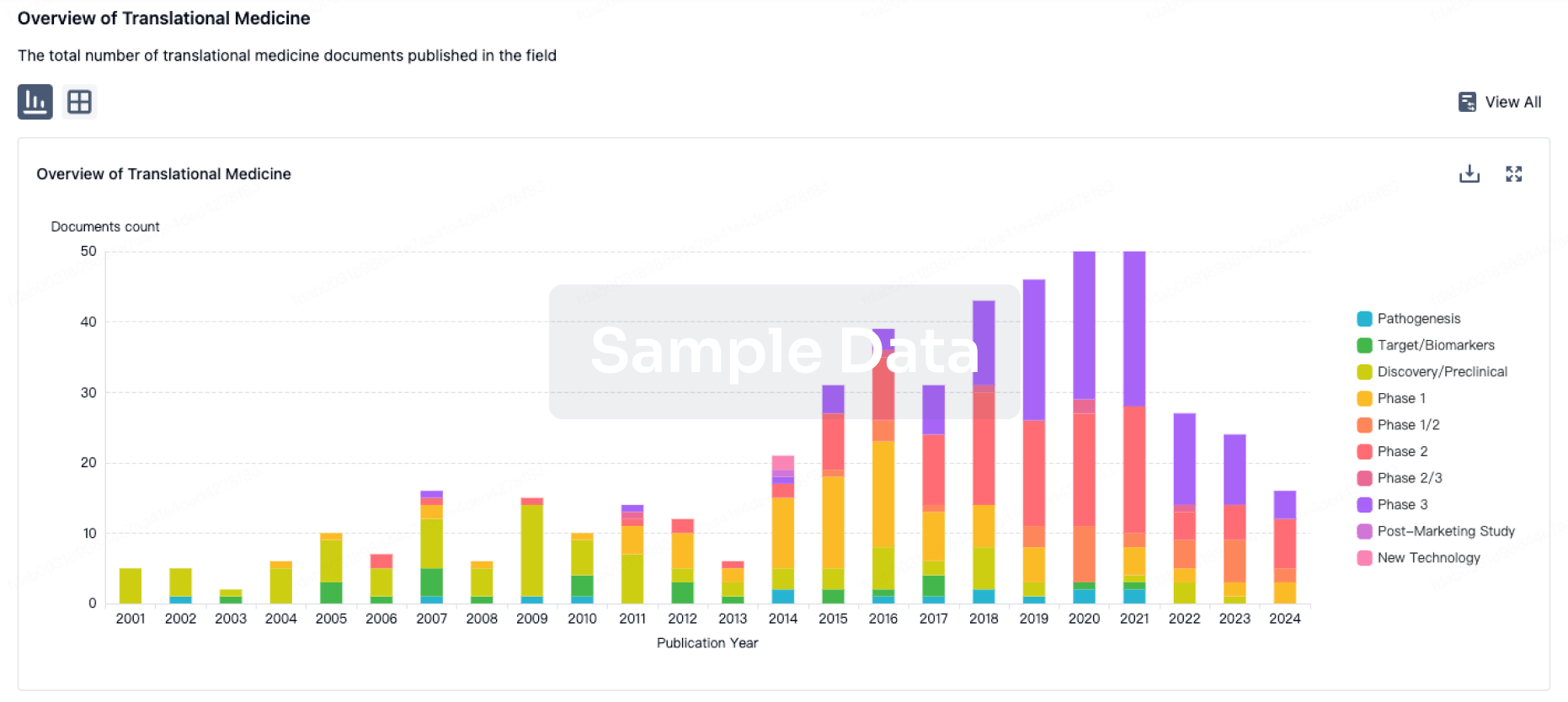
Translational Medicine
Boost your research with our translational medicine data.
login
or
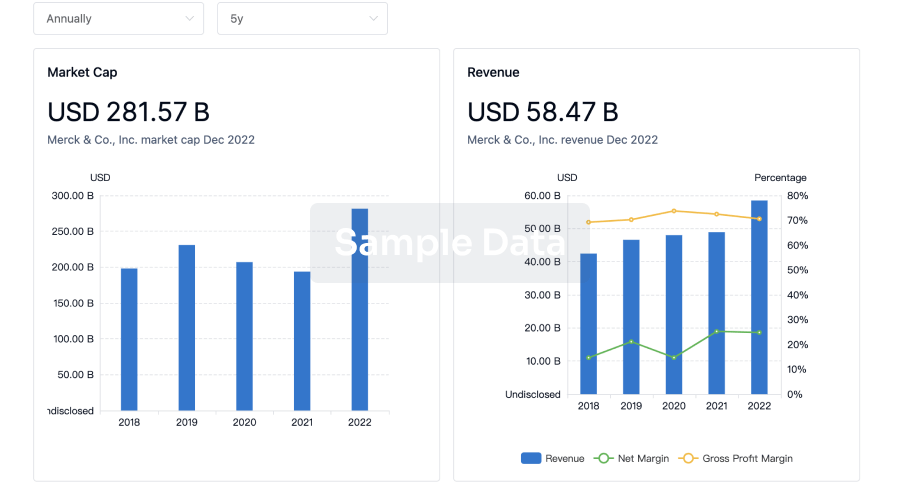
Profit
Explore the financial positions of over 360K organizations with Synapse.
login
or
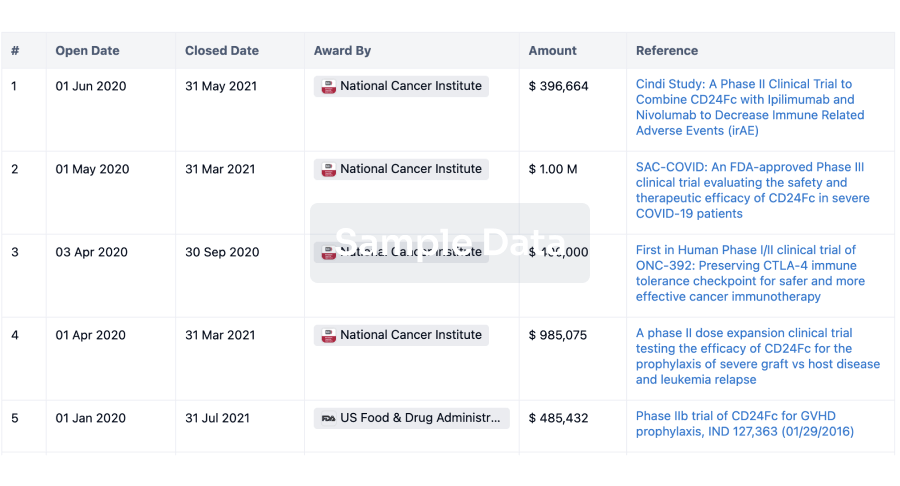
Grant & Funding(NIH)
Access more than 2 million grant and funding information to elevate your research journey.
login
or
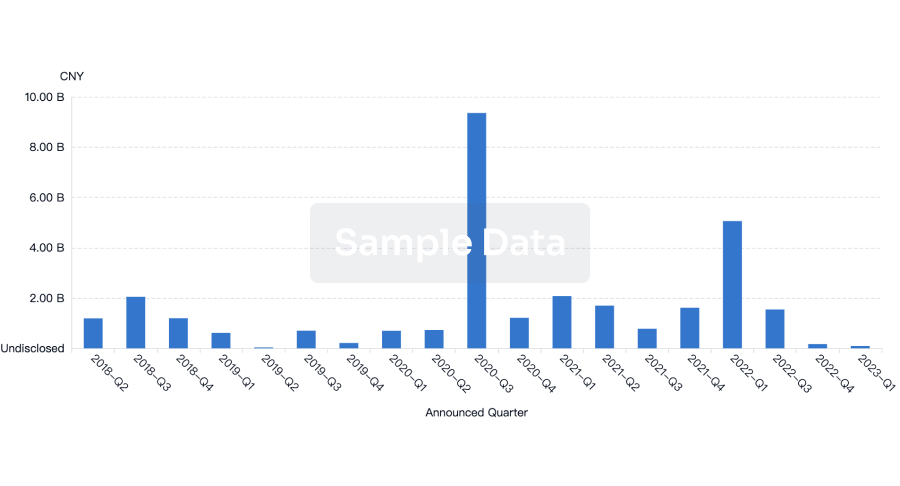
Investment
Gain insights on the latest company investments from start-ups to established corporations.
login
or
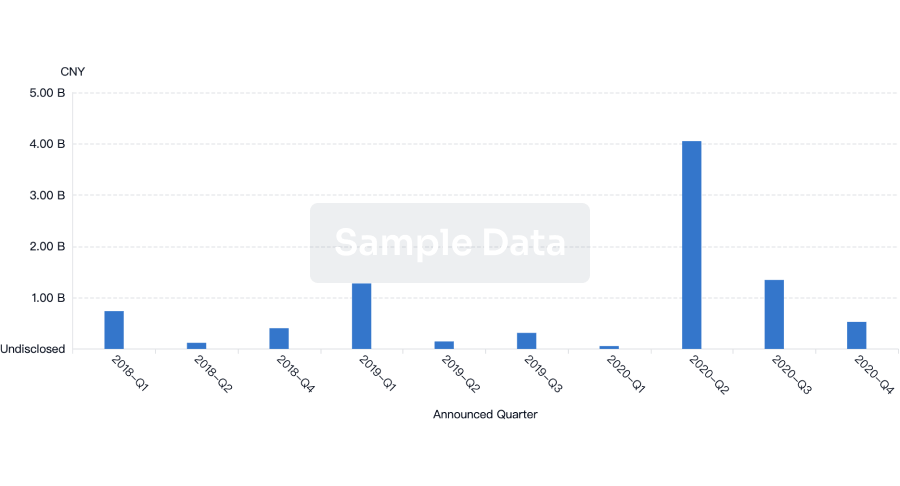
Financing
Unearth financing trends to validate and advance investment opportunities.
login
or
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free