Request Demo
Last update 04 Mar 2026

Bernhardt Laboratories, Inc.
Last update 04 Mar 2026
Overview
Related
100 Clinical Results associated with Bernhardt Laboratories, Inc.
Login to view more data
0 Patents (Medical) associated with Bernhardt Laboratories, Inc.
Login to view more data
4
Literatures (Medical) associated with Bernhardt Laboratories, Inc.01 Apr 2025·AMERICAN JOURNAL OF DERMATOPATHOLOGY
BRCA1-Associated Protein-1 Inactivated Melanoma Arising in a Pre-existing Nevus With ALK Fusion and Low Tumor Mutational Burden
Article
Author: Pradhan, Dinesh ; Niedt, George ; Aung, Phyu P. ; Dumur, Catherine I. ; Sangueza, Omar ; Phelps, Robert ; Patel, Ankush ; Krishnan, Ramakrishnan ; Shaker, Nada ; Prieto, Victor ; Torres-Cabala, Carlos
Abstract::
Breast cancer1-associated protein 1 (BAP-1)-inactivated melanocytic tumors are a group of familial or sporadic lesions with distinctive histology and molecular features. Inherited germline inactivating mutations in BAP1 have been associated with the development of multiple epithelioid melanocytic neoplasms resembling Spitz nevi and increased susceptibility for developing several malignancies, including uveal melanoma, cutaneous melanoma, renal cell carcinoma, mesothelioma, and other tumors. Cutaneous melanoma with loss of BAP1 expression is rare. We present a unique case of BAP1-inactivated melanoma with anaplastic lymphoma kinase (ALK) fusion arising in a pre-existing BAP1-inactivated nevus in a 47-year-old female patient who presented with a dome-shaped red papule on the superior crus of the right antihelix. Histology revealed intradermal melanocytic proliferation with biphenotypic morphology. There was a proliferation of atypical melanocytes showing epithelioid features in the background of nevus. Mitotic figures were identified in the cytologically atypical component of the lesion. Mart-1/Ki67 dual stain demonstrated a higher proliferation index in the larger epithelioid atypical cells, supporting the diagnosis of melanoma. Nuclear BAP-1 expression was lost in the larger atypical cells and associated nevoid cells. Preferentially expressed antigen in melanoma stain demonstrated focal positive staining in 20%–30% of the melanocytes. Immunostaining for B-Raf proto-oncogene, serine/threonine kinase V600E was diffusely positive and ALK demonstrated patchy immunoreactivity in the melanocytic proliferation. Interphase fluorescence in situ hybridization studies showed gains at chromosome 6p25 (Ras responsive element binding protein 1) in the tumor cells. The comprehensive next-generation sequencing revealed B-Raf proto-oncogene, serine/threonine kinase V600E mutation, TP53 mutation, ALK fusion, BAP1 loss (copy number variation = 0.0, potentially germline), and loss of MAP2K7, Von Hippel-Lindau tumor suppressor, FGFR3, CDKN2A, 19q, and telomerase reverse transcriptase. The tumor was microsatellite stable with a low tumor mutational burden (5.76 mutations/Mb). The tumor was completely excised with negative margins. The patient is doing well at 17 months follow-up with no signs of recurrence.
01 Sep 2024·JAAD case reports
Longstanding red, lobular nodule on an elderly male’s thigh
Article
Author: Davis, Cindy L ; Martin, Kiera ; Stepien, Angelia L ; Krishnamurthy, Karthik ; Meckley, Abigail L
A 69-year-old male presented with 2, adjacent lesions on the left thigh (Fig 1). The initial lesion was first noted 9 years prior and was reported to be slow-growing with associated bleeding. Months later, the patient noticed an adjacent asymptomatic lesion. Clinical examination demonstrated a 2.7 × 3.2 centimeter exophytic nodule and a distal flesh-colored, firm, subcutaneous nodule. He denied systemic symptoms. A biopsy of the exophytic nodule showed acrosyringeal cells, ducts, an invasive growth pattern, atypia, mitoses, and necrosis (Fig 2). Immunohistochemical staining for p53 demonstrated focal null phenotype (Fig 3).View Large Image Figure ViewerDownload Hi-res image Download (PPT)View Large Image Figure ViewerDownload Hi-res image Download (PPT) Question 1: What is the most likely diagnosis?A.Juxtaepidermal poromaB.Eccrine porocarcinoma (EPC)C.Malignant mixed tumorD.HidradenocarcinomaE.Eccrine angiomatous hamartoma Answers:A.Juxtaepidermal poroma – Incorrect. Poromas are commonly found on the palms or soles as a solitary papule or nodule with a vascular appearance. A poroma is a benign sweat gland tumor and does not have cytologic atypia or mitoses. When a poroma occurs in the papillary dermis with continuity into the epidermis it is termed juxtaepidermal poroma.B.EPC – Correct. EPC is an uncommon sweat gland malignancy and usually occurs in the elderly.1Le H.M.L. Faugeras L. De Moor V. et al.Eccrine porocarcinoma: a challenging diagnostic and therapeutic tumoral entity.Case Rep Oncol. 2021; 14: 700-705https://doi.org/10.1159/000514984Crossref PubMed Scopus (8) Google Scholar The location of the lesions is helpful to this diagnosis as the lower extremity is the single most common site for porocarcinomas. Histology resembles classic poroma but has infiltrative growth, cytologic atypia, mitoses, and necrosis.C.Malignant mixed tumor – Incorrect. Malignant mixed tumor (malignant chondroid syringoma) is a rare, aggressive tumor that usually occurs on the distal extremities or foot. However, on histology there are malignant epithelial cells and myxoid or chondroid stroma.D.Hidradenocarcinoma – Incorrect. Hidradenocarcinoma is an aggressive tumor that most commonly occurs on the head or neck. Histology shows sweat ducts within the tumor with atypia and mitoses and prominent dermal sclerosis with keloidal collagen.E.Eccrine angiomatous hamartoma – Incorrect. Eccrine angiomatous hamartomas most commonly present in children as a tender, dusky nodule. Histology shows mature sweat glands surrounded by vessels. Question 2: What immunohistochemical staining can help confirm the cell origin of this tumor?A.CD31B.DesminC.SOX10D.Carcinoembryonic antigenE.CK7 Answers:A.CD31 – Incorrect. This tumor originates from eccrine ductal differentiation. CD31 is an endothelial cell marker and helps confirm a tumor of vascular origin.B.Desmin – Incorrect. Desmin is a mesenchymal marker for skeletal and most smooth muscle cells.C.SOX10 – Incorrect. SOX10 is a nuclear marker of melanocytes and Schwann cells and stains positively in melanoma.D.Carcinoembryonic antigen – Correct. EPC is a tumor of eccrine ductal differentiation. Immunohistochemical staining with carcinoembryonic antigen positively stains the neoplastic eccrine cells lining the ducts and clefts. Additional helpful positive stains include epithelial membrane antigen, keratin, p53, and p63.1Le H.M.L. Faugeras L. De Moor V. et al.Eccrine porocarcinoma: a challenging diagnostic and therapeutic tumoral entity.Case Rep Oncol. 2021; 14: 700-705https://doi.org/10.1159/000514984Crossref PubMed Scopus (8) Google ScholarE.CK7 – Incorrect. CK7 stains glandular epithelium and helps determine the origin of metastatic carcinoma when used in conjunction with CK20. It is also positive in Paget's disease and extramammary Paget's disease. It is not specific to eccrine cells. Question 3: What is the initial treatment of choice?A.Wide local excision of the lesionB.PembrolizumabC.ChemotherapyD.AcitretinE.Radiation Answers:A.Wide local excision of the lesion – Correct. Given the rarity of this tumor there are no work-up or treatment guidelines, however wide local excision is currently considered the mainstay of treatment for EPC.1Le H.M.L. Faugeras L. De Moor V. et al.Eccrine porocarcinoma: a challenging diagnostic and therapeutic tumoral entity.Case Rep Oncol. 2021; 14: 700-705https://doi.org/10.1159/000514984Crossref PubMed Scopus (8) Google Scholar,2Nazemi A. Higgins S. Ly A. Wysong A. Porocarcinoma: a literature review.J Am Acad Dermatol. 2017; 76https://doi.org/10.1016/j.jaad.2017.04.781Abstract Full Text Full Text PDF Google Scholar Use of Mohs micrographic surgery for treatment of EPC is increasing and its use can be considered for tumors with high-risk features.3Tidwell J. Mayer J. Malone J. Schadt C. Brown T. Treatment of eccrine porocarcinoma with Mohs micrographic surgery: a case series.J Am Acad Dermatol. 2015; 72 (Supplement 1. https://doi.org/10.1016/j.jaad.2015.02.1054)Google Scholar Radiologic staging should be considered to evaluate for lymph node involvement or metastasis. EPC holds a high risk of recurrence and mortality, and multistep management is frequently required for successful treatment.2Nazemi A. Higgins S. Ly A. Wysong A. Porocarcinoma: a literature review.J Am Acad Dermatol. 2017; 76https://doi.org/10.1016/j.jaad.2017.04.781Abstract Full Text Full Text PDF Google ScholarB.Pembrolizumab – Incorrect. Immunotherapy with pembrolizumab is not currently considered a primary treatment for EPC. There are reports of successful pembrolizumab use for metastatic porocarcinoma; however further research is necessary to elucidate its safety and effectiveness for EPC.4Singh A. Nguyen L. Everest S. Vinogradov M. Metastatic porocarcinoma effectively managed by pembrolizumab.Cureus. 2021; 13e20004https://doi.org/10.7759/cureus.20004Crossref Google ScholarC.Chemotherapy – Incorrect. Chemotherapy has been used for EPC management as an adjunct therapy, for metastasic disease, or recurrence of disease. However, no standardized regimen exists and evidence of its effectiveness is lacking.1Le H.M.L. Faugeras L. De Moor V. et al.Eccrine porocarcinoma: a challenging diagnostic and therapeutic tumoral entity.Case Rep Oncol. 2021; 14: 700-705https://doi.org/10.1159/000514984Crossref PubMed Scopus (8) Google ScholarD.Acitretin – Incorrect. Acitretin is still being studied as a treatment for certain nonmelanoma skin cancers and is not currently used to treat EPCs.E.Radiation – Incorrect. Although radiation has been used concomitantly with wide local excision, radiation alone is not considered first-line treatment of EPCs. High metastasis rates have been seen in patients treated with radiotherapy for EPC.2Nazemi A. Higgins S. Ly A. Wysong A. Porocarcinoma: a literature review.J Am Acad Dermatol. 2017; 76https://doi.org/10.1016/j.jaad.2017.04.781Abstract Full Text Full Text PDF Google Scholar None disclosed.
Frontiers in molecular neuroscienceQ2 · MEDICINE
Cross-Species Co-analysis of Prefrontal Cortex Chronic Ethanol Transcriptome Responses in Mice and Monkeys
Q2 · MEDICINE
ArticleOA
Author: Smith, Maren L ; Farris, Sean P ; Becker, Howard C ; Dumur, Catherine I ; Grant, Kathleen A ; Lopez, Marcelo F ; Miles, Michael F ; Bogenpohl, James W
Despite recent extensive genomic and genetic studies on behavioral responses to ethanol, relatively few new therapeutic targets for the treatment of alcohol use disorder have been validated. Here, we describe a cross-species genomic approach focused on identifying gene networks associated with chronic ethanol consumption. To identify brain mechanisms underlying a chronic ethanol consumption phenotype highly relevant to human alcohol use disorder, and to elucidate potential future therapeutic targets, we conducted a genomic study in a non-human primate model of chronic open-access ethanol consumption. Microarray analysis of RNA expression in anterior cingulate and subgenual cortices from rhesus macaques was performed across multiple cohorts of animals. Gene networks correlating with ethanol consumption or showing enrichment for ethanol-regulated genes were identified, as were major ethanol-related hub genes within these networks. A subsequent consensus module analysis was used to co-analyze monkey data with expression data from a chronic intermittent ethanol vapor-exposure and consumption model in C57BL/6J mice. Ethanol-related gene networks conserved between primates and rodents were enriched for genes involved in discrete biological functions, including; myelination, synaptic transmission, chromatin modification, Golgi apparatus function, translation, cellular respiration, and RNA processing. The myelin-related network, in particular, showed strong correlations with ethanol consumption behavior and displayed marked network reorganization between control and ethanol-drinking animals. Further bioinformatics analysis revealed that these networks also showed highly significant overlap with other ethanol-regulated gene sets. Altogether, these studies provide robust primate and rodent cross-species validation of gene networks associated with chronic ethanol consumption. Our results also suggest potential novel focal points for future therapeutic interventions in alcohol use disorder.
100 Deals associated with Bernhardt Laboratories, Inc.
Login to view more data
100 Translational Medicine associated with Bernhardt Laboratories, Inc.
Login to view more data
Corporation Tree
Boost your research with our corporation tree data.
login
or
Pipeline
Pipeline Snapshot as of 12 Mar 2026
No data posted
Login to keep update
Deal
Boost your decision using our deal data.
login
or

Translational Medicine
Boost your research with our translational medicine data.
login
or

Profit
Explore the financial positions of over 360K organizations with Synapse.
login
or

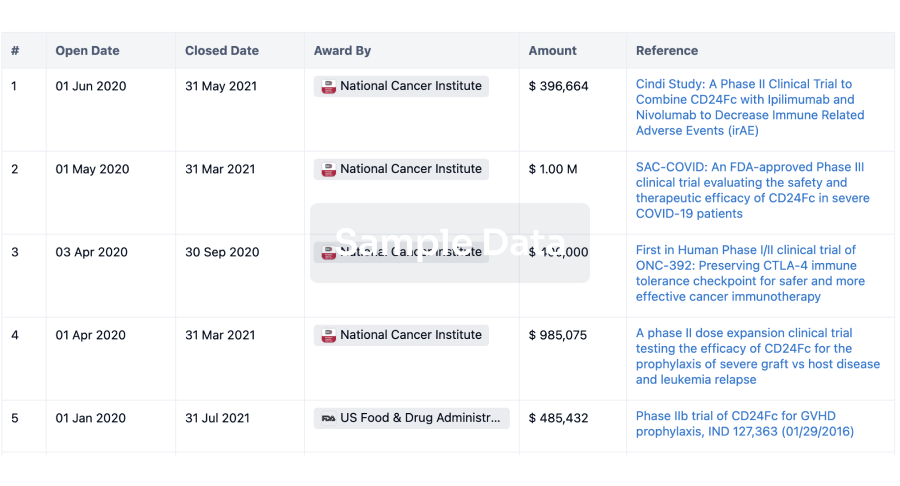
Grant & Funding(NIH)
Access more than 2 million grant and funding information to elevate your research journey.
login
or
Investment
Gain insights on the latest company investments from start-ups to established corporations.
login
or

Financing
Unearth financing trends to validate and advance investment opportunities.
login
or

AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free