Last update 01 Nov 2024
Uw Solutions
Last update 01 Nov 2024
Overview
Related
100 Clinical Results associated with Uw Solutions
Login to view more data
0 Patents (Medical) associated with Uw Solutions
Login to view more data
4
News (Medical) associated with Uw Solutions11 Jun 2024
TUESDAY, June 11, 2024 -- A test used to gauge whether a college athlete has suffered a concussion is right only half the time and may be useless, new research finds.
The test used by the NCAA, which oversees college sports, measures an athlete's cognitive skills, and is one of three tests (symptoms and balance tests being the other two) that doctors use to identify concussion.
“If you don’t do well on the cognitive exam, it suggests you have a concussion. But many people who are concussed do fine on the exam,” said study lead author
Dr. Kimberly Harmon
. She is a professor of family medicine and section head of sports medicine at the University of Washington School of Medicine.
Harmon said she was prompted to conduct the study by firsthand experience working on the sidelines as team physician for the UW Huskies.
"Some people were concussed and they did well on the recall tests. Some people weren’t concussed and they didn’t do well. So I thought we should study it,” she explained in a UW news release.
The test itself is one part of what's known as the Sport Concussion Assessment Tool (SCAT). In the cognitive skills section of SCAT, the patient is asked "orientation" questions (What day is it? What month is it?), then a memory test (recite back a list of words), then a concentration challenge (repeat a series of numbers in reverse order).
Tests for a range of
concussion symptoms
, plus a balance test, make up the other two-thirds of the SCAT exam.
The new study involved 92 NCAA Division I athletes who sustained a concussion between mid-July of 2020 and the end of 2022. All had undergone a concussion evaluation within 48 hours of injury.
Their SCAT results were compared to those of 92 (non-injured) teammates.
Harmon's team found no difference in cognitive test scores between the injured and non-injured athletes. In fact, 45% of players who were found to have a concussion actually performed better on their cognitive tests than in a "baseline" test before the concussion, researchers noted.
“If you get hit in the head and go to the sideline and say, ‘I have a headache. I’m dizzy. I don’t feel right,’ I can say with pretty good assurance that you have a concussion,” Harmon said.
“I don’t need to do any [cognitive] testing," she reasoned. "The problem is that some athletes don’t want to come out. They don’t report their symptoms or may not recognize their symptoms. So then you need an objective, accurate test to tell you whether you can safely put the athlete back on the field. We don’t have that right now.”
She said that keeping athletes safe requires real teamwork between health care staff and the athletes themselves.
“Although an increase in symptoms is highly suggestive of concussion, this relies on accurate reporting by the athlete who may not report symptoms because of a desire to return to play, a fear of letting teammates down, minimizing the seriousness of concussion, difficulty discerning symptoms, a delay in symptom development, or other reasons," Harmon said.
"We are still short of the holy grail, which is an objective test for concussion,” she said. “For now, this study shows how important it is for athletes to disclose their symptoms.”
The study was published June 11 in
JAMA Network Open
.
Whatever your topic of interest,
subscribe to our newsletters
to get the best of Drugs.com in your inbox.
11 Jun 2024
When college athletes are evaluated for a possible concussion, the diagnosis is based on an athletic trainer or team physician's assessment of three things: the player's symptoms, physical balance and cognitive skills. Research published today suggests that almost half of athletes who are ultimately diagnosed with a concussion will test normally on the recommended cognitive-skills test.
When college athletes are evaluated for a possible concussion, the diagnosis is based on an athletic trainer or team physician's assessment of three things: the player's symptoms, physical balance and cognitive skills.
Research published today suggests that almost half of athletes who are ultimately diagnosed with a concussion will test normally on the recommended cognitive-skills test.
"If you don't do well on the cognitive exam, it suggests you have a concussion. But many people who are concussed do fine on the exam," said Dr. Kimberly Harmon, the study's lead author. She is a professor of family medicine and section head of sports medicine at the University of Washington School of Medicine.
The study findings appear in JAMA Network Open.
Harmon said her sideline experiences as a team physician for the UW Huskies caused her to wonder how to accurately interpret the cognitive-screening portion of the Sport Concussion Assessment Tool (SCAT). Introduced in 2004 by the Concussion in Sport Group, the SCAT (now in its fifth iteration, SCAT5) was intended to standardize the gathering of information from athletes with a potential head injury.
The SCAT first prompts an athlete about whether they are experiencing any of 22 symptoms such as headache, nausea or blurred vision, and symptom severity. Then the tool tests the athlete's cognition in several ways.
First come questions of orientation. (What day is it? What month is it?) Then a test of immediate memory, in which a list of 10 words is read aloud to the athlete, who is asked to restate the list. This sequence is repeated three times. Then the athlete's concentration is tested by having to repeat short sequences of numbers in reverse order. Then comes a prescribed evaluation of the athlete's balance, after which the athlete is again asked to recall the 10 words from the first list.
In Harmon's experience as a team physician, she saw that "some people were concussed and they did well on the recall tests. Some people weren't concussed and they didn't do well. So I thought we should study it," she said.
The study involved 92 NCAA Division I athletes who sustained a concussion between July 13, 2020, and Dec. 31, 2022, and who had a concussion evaluation within 48 hours. The investigators also recruited 92 of the concussed players' teammates as matched control subjects, each of whom was given the SCAT5 screening within two weeks of the incident concussion.
All athletes in the study had previously completed NCAA-required baseline concussion screenings. The investigators found no significant differences in baseline scores between the athletes with and without concussion.
Harmon and colleagues analyzed the study participants' SCAT5 responses and found that the word-recall tests had little predictive value for concussion. In fact, almost half (45%) of the concussed athletes performed at or above their baseline cognitive-test results, the researchers reported.
Instead, the study showed that the most accurate predictor of concussion were the athletes' responses to questions about their symptoms.
"If you get hit in the head and go to the sideline and say, 'I have a headache. I'm dizzy. I don't feel right,' I can say with pretty good assurance that you have a concussion," Harmon said. "I don't need to do any testing. The problem is that some athletes don't want to come out. They don't report their symptoms or may not recognize their symptoms. So then you need an objective, accurate test to tell you whether you can safely put the athlete back on the field. We don't have that right now."
During in-game evaluations for a concussion, team trainers and physicians must quickly synthesize the available evidence and make their best clinical judgment about a player's health. The responsibility for a safety-first decision, though, also lies in part with the athletes, the study's authors wrote:
"Although an increase in symptoms is highly suggestive of concussion, this relies on accurate reporting by the athlete who may not report symptoms because of a desire to return to play, a fear of letting teammates down, minimizing the seriousness of concussion, difficulty discerning symptoms, a delay in symptom development, or other reasons."
"We are still short of the holy grail, which is an objective test for concussion," Harmon said. "For now, this study shows how important it is for athletes to disclose their symptoms."
The study was funded in part by the Jack and Luellen Cherneski and the Chisholm Foundation.
Clinical Result
25 Apr 2024
According to UW’s Baker Lab, their AI constructed ring-shaped peptides the researchers say have the potential to interrupt the body’s pain signals, disrupt viral infections or interfere with growing tumors.
In recent years, artificial intelligence programs for drug design have steadily shown they can help explore far beyond just small-molecule drugs—by illuminating how proteins fold and interact, all the way up to large antibodies. Get ready to add another category to the list.
Researchers at the University of Washington’s Institute for Protein Design have put forward a paper showing its AI algorithms can help create millions of never-before-seen drug-like peptides—chains of amino acids that are much smaller than your typical protein, but still capable of delivering potent effects within the human body.
Peptides have formed the basis of dozens of drugs and treatments—including insulin, for example—and serve as the “P” in the hormone GLP-1, the target of today’s blockbusters Ozempic and Wegovy.
According to researchers in UW’s Baker Lab, their AI programs were able to construct ring-shaped peptides known as macrocycles—a group they say has the potential to cross tricky cell membranes to interrupt the body’s pain signals, disrupt viral infections or interfere with growing tumors, while possibly being delivered as an oral pill.
“Certain snails, sponges and other marine animals produce macrocycles with potent activities, and scientists have had some success turning these natural products into medicines,” said Patrick Salveson, who helped lead the study while at the Baker Lab, which was published this week in the journal Science.
“But until now, there hasn’t been a way to systematically create new macrocycles that might treat specific diseases. Our work shows that this promising class of chemicals can be systematically explored using computational design,” said Salveson, who currently serves as co-founder and chief technology officer of Vilya Therapeutics, a UW spinout that made its debut in 2022 and has licensed the tech for development.
The work to develop deep-learning programs for generating peptides has been slow in part because there haven’t been enough molecule models in the relevant size range to help train the algorithms.
“The challenge here was to come up with an efficient way to model these chemicals on the computer,” said study author Adam Moyer, formerly of the Baker Lab, and now director of molecular design and co-founder of Vilya.
“We found a solution that combines the accuracy of AIMNet, which is an AI-powered tool for simulating quantum mechanics, with the speed of a more traditional software approach. We optimized these steps to create a new way to quickly build ring-shaped compounds,” Moyer said.
Previously, members of the Baker Lab, Vilya and others also showed that they could build on the work of DeepMind’s AlphaFold protein-computing network and adapt it for smaller cyclic peptide chains, to help custom design new potential drugs for a variety of diseases.
Now, the researchers have demonstrated that they can systematically generate and manufacture small macrocycles with four or fewer amino acids—with subsequent X-ray and nuclear magnetic resonance tests showing that they come close to aligning with the original AI blueprints.
To start, they picked one that could potentially inhibit a protein from the coronavirus behind COVID-19, as well as additional macrocycles capable of blocking a protein essential to the survival of cancer cells without affecting healthier pathways.
Almost all were able to cross artificial cell membranes in preclinical experiments and could survive enzymatic degradation processes for more than 24 hours, according to the researchers.
Another Baker Lab spinout made headlines earlier this week, with the antibody-focused Xaira Therapeutics posting a $1 billion debut fundraising—led by Arch Venture Partners, which also backed Vilya.
Meanwhile, drugmakers such as Merck & Co. have called macrocyclic peptides “the next wave of drug discovery,” and earlier this year inked a $220 million deal with the AI designer Unnatural Products. And last year, Roche’s Genentech signed a $1 billion pact with the Japanese biotech PeptiDream, which is developing a peptide discovery platform.
100 Deals associated with Uw Solutions
Login to view more data
100 Translational Medicine associated with Uw Solutions
Login to view more data
Corporation Tree
Boost your research with our corporation tree data.
login
or
Pipeline
Pipeline Snapshot as of 16 Nov 2024
No data posted
Login to keep update
Deal
Boost your decision using our deal data.
login
or
Translational Medicine
Boost your research with our translational medicine data.
login
or
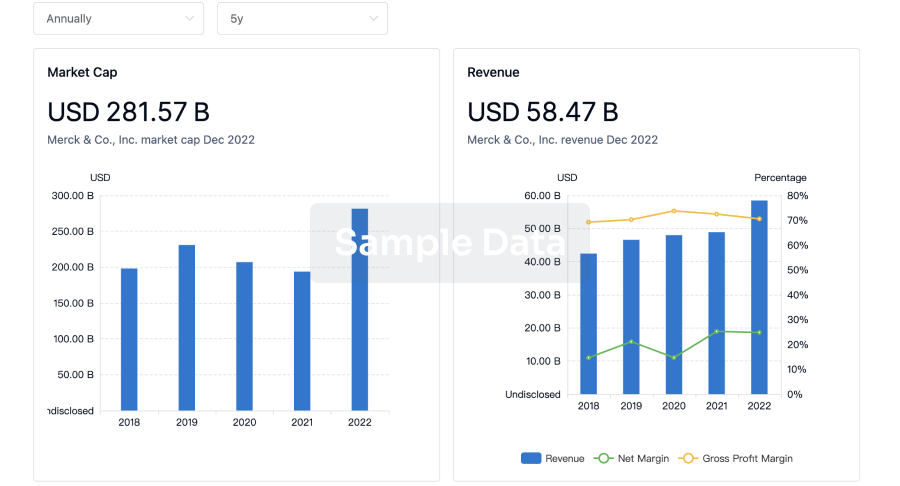
Profit
Explore the financial positions of over 360K organizations with Synapse.
login
or
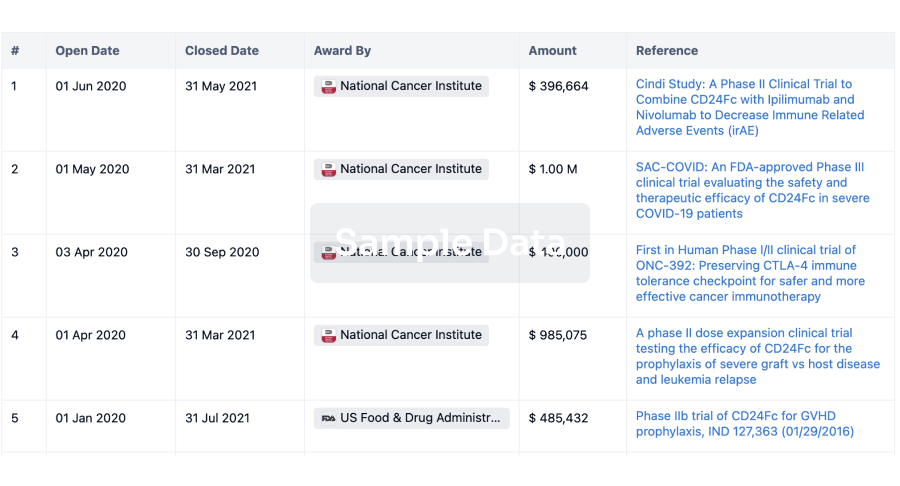
Grant & Funding(NIH)
Access more than 2 million grant and funding information to elevate your research journey.
login
or
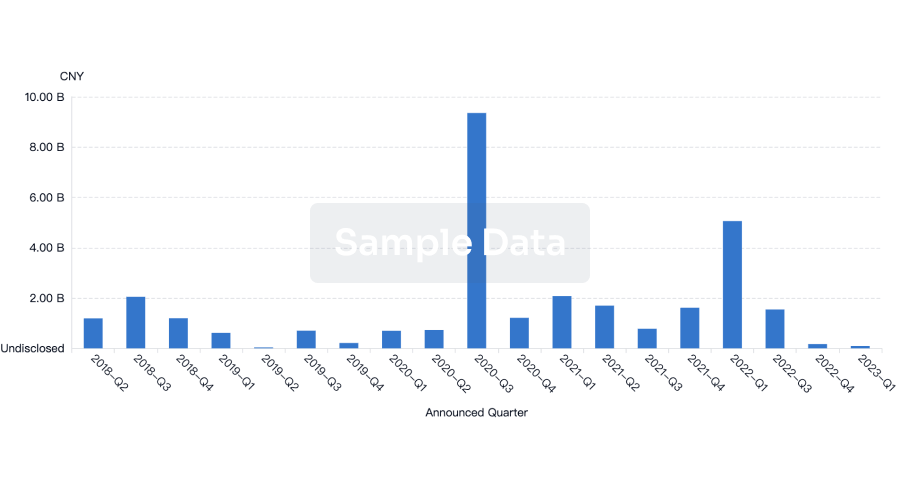
Investment
Gain insights on the latest company investments from start-ups to established corporations.
login
or
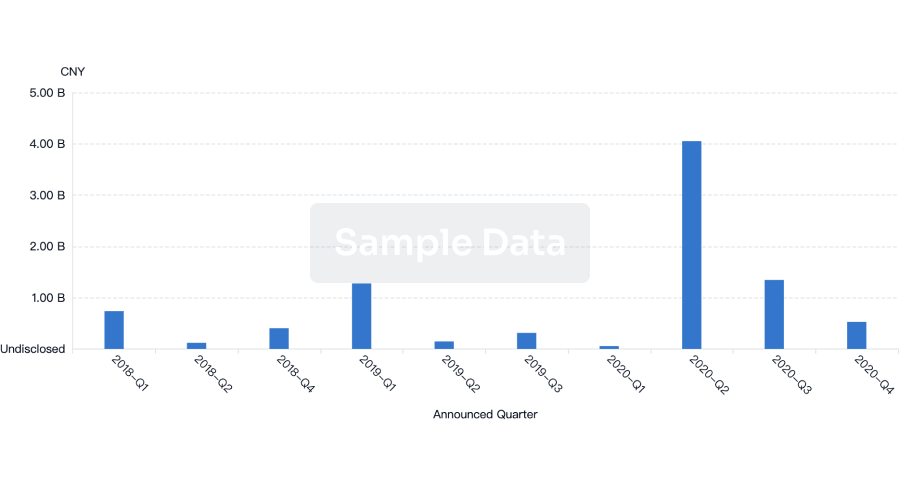
Financing
Unearth financing trends to validate and advance investment opportunities.
login
or
Chat with Hiro
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free