Request Demo
Last update 08 May 2025

Care New England Health System, Inc.
Last update 08 May 2025
Overview
Related
NCT06842875
Effect of a Technology-based Collaborative Model on Persistent Hypertension and Preventive Care Attendance Among Postpartum People With Hypertensive Disorders of Pregnancy

NCT04188041
Improving Rhode Island's Tuberculosis Preventive Services in Primary Care: A Mixed-Methods Evaluation of an Innovative Telementoring Model

NCT02579915
Phase 2 Randomized Controlled Trial of Attention and Interpretation Modification (AIM) for Anxiety Disorders in Primary Care

100 Clinical Results associated with Care New England Health System, Inc.
Login to view more data
Login to view more data
17 Mar 2025Clinical Infectious Diseases
A 34-Year-Old Man With a Pustular Rash, Subjective Fever, and Foot Pain
Article
Author: Tesson, Sophie ; Abdelrahman, Houda ; Kensey, Nicholas ; Higgs, James ; Chan, Angelica
11 Mar 2025Circulation
Abstract P1093: Race, Sex, and SES Differences in Heart Failure Incidence: A Cross-Cohort Collaboration
Author: Allen, Norrina ; Howe, Chanelle ; Min, Nancy ; Kucharska-Newton, Anna ; Ahmad, Faraz ; Newburg, James ; LaMonte, Michael ; Jacobs, David ; Hsieh, Tiffany ; KIZER, JORGE ; Roberts, Mary ; Xanthakis, Vanessa ; Levitan, Emily ; Forman, Daniel ; Rosamond, Wayne ; Eaton, Charles ; Moafi-Madani, Miremad
01 Feb 2025Journal of Clinical Oncology
The impact of prediabetes on cerebrovascular risk among patients with gastrointestinal malignancies.
Author: Agrawal, Siddharth Pravin ; Sharma, Tanuj ; Raval, Maharshi ; Chintakuntlawar, Ashish V. ; Uttam Chandani, Kanishka ; Kondapally, Apoorva ; Siddiq, Sajid ; Nadeem, Ahmed ; Sait, Mohamed Ayaan ; Ijaz, Ambreen ; Mittal, Kriti
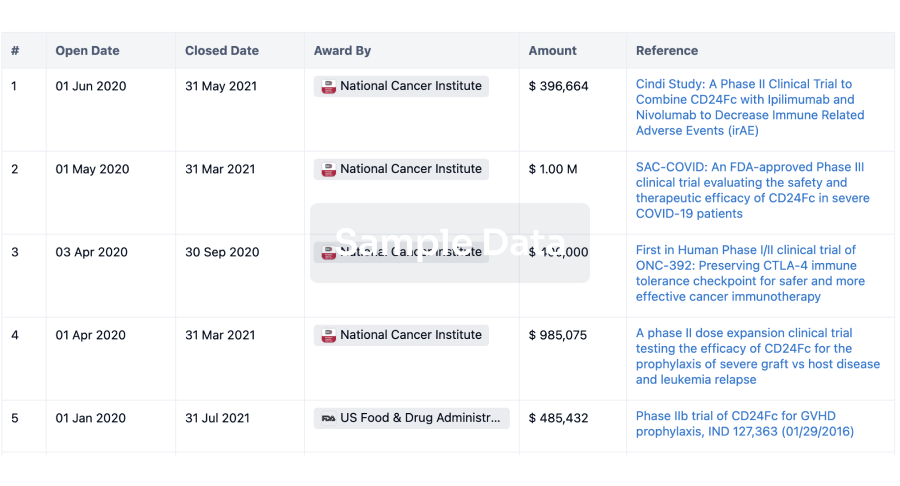
100 Deals associated with Care New England Health System, Inc.
Login to view more data
100 Translational Medicine associated with Care New England Health System, Inc.
Login to view more data
Corporation Tree
Boost your research with our corporation tree data.
login
or
Pipeline
Pipeline Snapshot as of 05 Mar 2026
No data posted
Login to keep update
Deal
Boost your decision using our deal data.
login
or

Translational Medicine
Boost your research with our translational medicine data.
login
or

Profit
Explore the financial positions of over 360K organizations with Synapse.
login
or

Grant & Funding(NIH)
Access more than 2 million grant and funding information to elevate your research journey.
login
or
Investment
Gain insights on the latest company investments from start-ups to established corporations.
login
or

Financing
Unearth financing trends to validate and advance investment opportunities.
login
or

AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free