Request Demo
What is the mechanism of Arformoterol Tartrate?
17 July 2024
Arformoterol tartrate is a long-acting beta-agonist (LABA) commonly used for the maintenance treatment of bronchoconstriction in patients with chronic obstructive pulmonary disease (COPD). Its mechanism of action is primarily centered around its role as a bronchodilator, facilitating easier breathing in individuals with obstructed airways.
The primary mechanism of arformoterol tartrate involves stimulating beta-2 adrenergic receptors located in the smooth muscle lining the bronchial tubes within the lungs. By binding to these receptors, arformoterol initiates a cascade of biochemical events that lead to muscle relaxation. This interaction starts with the activation of the enzyme adenylate cyclase, which converts adenosine triphosphate (ATP) to cyclic adenosine monophosphate (cAMP).
The increase in cAMP levels results in the activation of protein kinase A (PKA). PKA then phosphorylates various target proteins within the cell, leading to a series of downstream effects that ultimately decrease intracellular calcium concentrations. Lower intracellular calcium inhibits the contractile activity of the smooth muscle cells, causing them to relax. This relaxation of the bronchial smooth muscle leads to bronchodilation, reducing airway resistance and making it easier for air to flow through the bronchial tubes.
Arformoterol tartrate is the (R,R)-enantiomer of formoterol, meaning it is one of two mirror-image forms of the molecule. The (R,R)-enantiomer has been shown to have greater potency and selectivity for the beta-2 adrenergic receptors compared to the (S,S)-enantiomer, which contributes to its therapeutic effectiveness.
The pharmacokinetics of arformoterol tartrate also play a crucial role in its efficacy as a long-acting bronchodilator. After inhalation, the drug is absorbed into the bloodstream and distributed throughout the body. It has a rapid onset of action, typically within 5 to 15 minutes, and maintains its bronchodilatory effects for up to 12 hours, which allows for twice-daily dosing. This long duration of action is beneficial for patients with COPD, as it helps maintain open airways throughout the day and night, reducing symptoms such as shortness of breath, wheezing, and chest tightness.
The metabolism of arformoterol tartrate occurs primarily in the liver, where it is broken down by various enzymes, including cytochrome P450 isoenzymes. The metabolites are then excreted through the kidneys. It is important to note that arformoterol tartrate, like other LABAs, should be used with caution and under proper medical guidance, particularly because of the potential risks associated with long-term use, such as an increased risk of asthma-related death if used as monotherapy in asthma patients without an accompanying inhaled corticosteroid.
In summary, the mechanism of arformoterol tartrate revolves around its ability to activate beta-2 adrenergic receptors in bronchial smooth muscle, leading to muscle relaxation and bronchodilation. This action alleviates symptoms of bronchoconstriction in COPD patients, improving their breathing and quality of life. Its pharmacokinetic properties, including rapid onset and prolonged duration of action, make it a valuable component in the management of chronic obstructive pulmonary disease.
The primary mechanism of arformoterol tartrate involves stimulating beta-2 adrenergic receptors located in the smooth muscle lining the bronchial tubes within the lungs. By binding to these receptors, arformoterol initiates a cascade of biochemical events that lead to muscle relaxation. This interaction starts with the activation of the enzyme adenylate cyclase, which converts adenosine triphosphate (ATP) to cyclic adenosine monophosphate (cAMP).
The increase in cAMP levels results in the activation of protein kinase A (PKA). PKA then phosphorylates various target proteins within the cell, leading to a series of downstream effects that ultimately decrease intracellular calcium concentrations. Lower intracellular calcium inhibits the contractile activity of the smooth muscle cells, causing them to relax. This relaxation of the bronchial smooth muscle leads to bronchodilation, reducing airway resistance and making it easier for air to flow through the bronchial tubes.
Arformoterol tartrate is the (R,R)-enantiomer of formoterol, meaning it is one of two mirror-image forms of the molecule. The (R,R)-enantiomer has been shown to have greater potency and selectivity for the beta-2 adrenergic receptors compared to the (S,S)-enantiomer, which contributes to its therapeutic effectiveness.
The pharmacokinetics of arformoterol tartrate also play a crucial role in its efficacy as a long-acting bronchodilator. After inhalation, the drug is absorbed into the bloodstream and distributed throughout the body. It has a rapid onset of action, typically within 5 to 15 minutes, and maintains its bronchodilatory effects for up to 12 hours, which allows for twice-daily dosing. This long duration of action is beneficial for patients with COPD, as it helps maintain open airways throughout the day and night, reducing symptoms such as shortness of breath, wheezing, and chest tightness.
The metabolism of arformoterol tartrate occurs primarily in the liver, where it is broken down by various enzymes, including cytochrome P450 isoenzymes. The metabolites are then excreted through the kidneys. It is important to note that arformoterol tartrate, like other LABAs, should be used with caution and under proper medical guidance, particularly because of the potential risks associated with long-term use, such as an increased risk of asthma-related death if used as monotherapy in asthma patients without an accompanying inhaled corticosteroid.
In summary, the mechanism of arformoterol tartrate revolves around its ability to activate beta-2 adrenergic receptors in bronchial smooth muscle, leading to muscle relaxation and bronchodilation. This action alleviates symptoms of bronchoconstriction in COPD patients, improving their breathing and quality of life. Its pharmacokinetic properties, including rapid onset and prolonged duration of action, make it a valuable component in the management of chronic obstructive pulmonary disease.
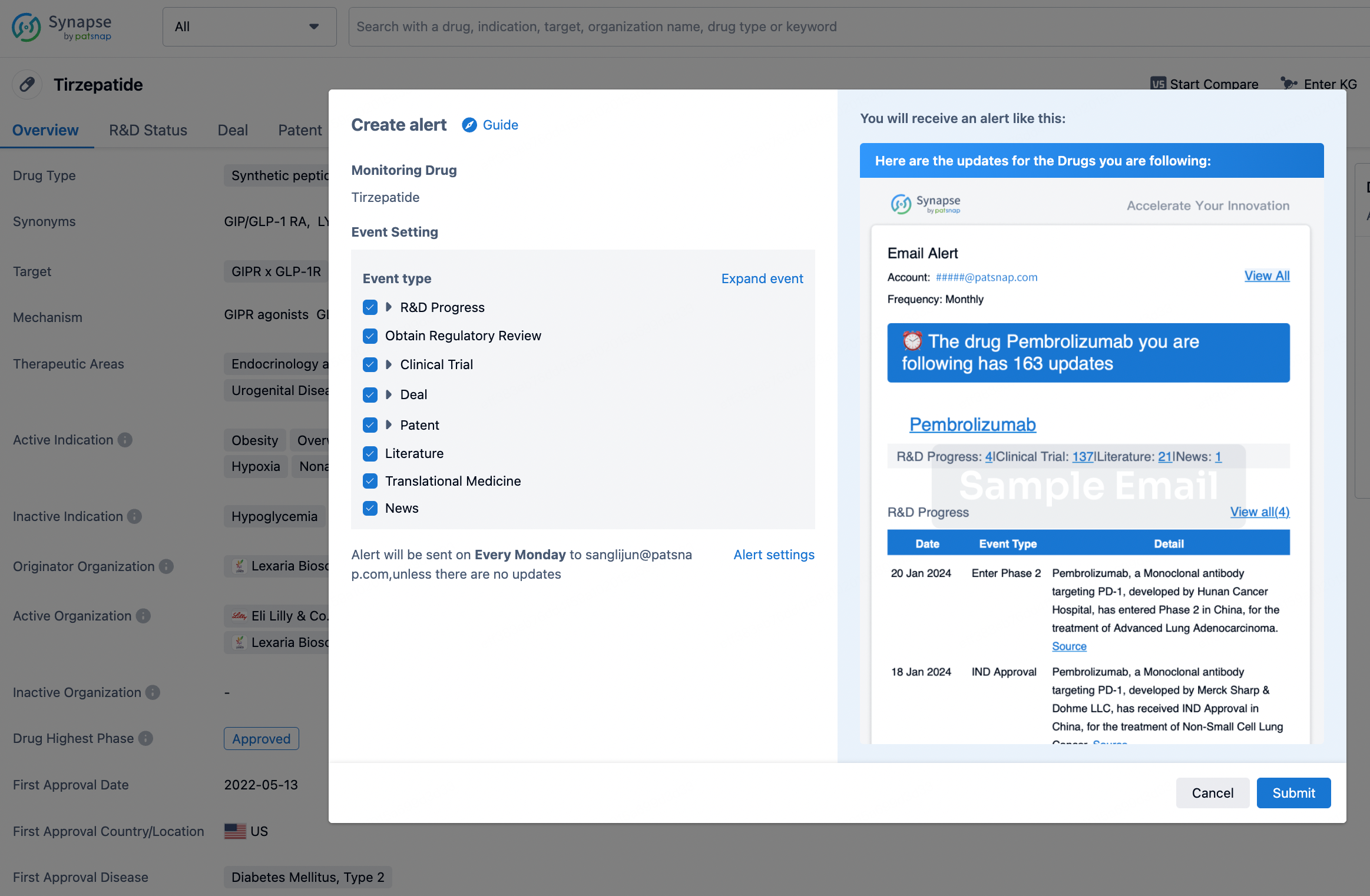
How to obtain the latest development progress of all drugs?
In the Synapse database, you can stay updated on the latest research and development advances of all drugs. This service is accessible anytime and anywhere, with updates available daily or weekly. Use the "Set Alert" function to stay informed. Click on the image below to embark on a brand new journey of drug discovery!
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.