Request Demo
What is the mechanism of Berotralstat Hydrochloride?
17 July 2024
Berotralstat Hydrochloride is an innovative pharmaceutical agent that has garnered attention for its efficacy in managing hereditary angioedema (HAE). To understand its mechanism, it's crucial to delve into the biological underpinnings of both HAE and the pharmacodynamics of Berotralstat Hydrochloride.
HAE is a rare genetic disorder characterized by recurrent episodes of severe swelling in various parts of the body, including the extremities, face, gastrointestinal tract, and airways. The disorder is primarily linked to a deficiency or dysfunction of C1 esterase inhibitor (C1-INH), which leads to the overproduction of bradykinin, a peptide that increases vascular permeability and causes edema.
Berotralstat Hydrochloride works as a potent and selective inhibitor of plasma kallikrein, an enzyme that plays a pivotal role in the kallikrein-kinin system. Plasma kallikrein is responsible for the cleavage of high-molecular-weight kininogen to produce bradykinin. By inhibiting plasma kallikrein, Berotralstat Hydrochloride effectively reduces the levels of bradykinin, thereby preventing the episodes of swelling associated with HAE.
The molecular structure of Berotralstat Hydrochloride allows it to bind with high specificity to the active site of plasma kallikrein, blocking its enzymatic activity. This binding is reversible, meaning that the drug can effectively modulate the activity of plasma kallikrein without permanently deactivating it. The selectivity of Berotralstat Hydrochloride ensures that it does not interfere with other proteases, minimizing potential side effects and enhancing its safety profile.
Pharmacokinetically, Berotralstat Hydrochloride is administered orally, providing convenience over other treatments that require intravenous or subcutaneous routes. Upon ingestion, the drug is absorbed through the gastrointestinal tract and reaches peak plasma concentrations within a few hours. Its bioavailability is influenced by food intake, with a high-fat meal increasing the absorption rate. Once in the bloodstream, Berotralstat Hydrochloride distributes relatively evenly across tissues, maintaining therapeutic concentrations.
Metabolism of Berotralstat Hydrochloride occurs primarily in the liver, where it undergoes biotransformation through pathways involving cytochrome P450 enzymes, specifically CYP3A4. This metabolism results in the formation of inactive metabolites, which are then excreted via urine and feces. The half-life of Berotralstat Hydrochloride is conducive to once-daily dosing, enhancing patient compliance and ensuring a consistent therapeutic effect.
Clinical trials have demonstrated the efficacy of Berotralstat Hydrochloride in reducing the frequency and severity of HAE attacks. Patients treated with this drug have shown significant improvement in symptom control, which translates to a better quality of life. Moreover, the adverse effects associated with Berotralstat Hydrochloride are generally mild to moderate, with the most common being gastrointestinal disturbances, such as nausea and diarrhea.
In summary, Berotralstat Hydrochloride offers a targeted approach to managing hereditary angioedema by inhibiting plasma kallikrein and subsequently reducing bradykinin levels. Its oral administration, selective mechanism of action, and favorable safety profile make it a valuable addition to the therapeutic options available for HAE patients. Understanding its mechanism provides insights into how modern pharmacological interventions can effectively address the underlying causes of genetic disorders, paving the way for more tailored and efficient treatments.
HAE is a rare genetic disorder characterized by recurrent episodes of severe swelling in various parts of the body, including the extremities, face, gastrointestinal tract, and airways. The disorder is primarily linked to a deficiency or dysfunction of C1 esterase inhibitor (C1-INH), which leads to the overproduction of bradykinin, a peptide that increases vascular permeability and causes edema.
Berotralstat Hydrochloride works as a potent and selective inhibitor of plasma kallikrein, an enzyme that plays a pivotal role in the kallikrein-kinin system. Plasma kallikrein is responsible for the cleavage of high-molecular-weight kininogen to produce bradykinin. By inhibiting plasma kallikrein, Berotralstat Hydrochloride effectively reduces the levels of bradykinin, thereby preventing the episodes of swelling associated with HAE.
The molecular structure of Berotralstat Hydrochloride allows it to bind with high specificity to the active site of plasma kallikrein, blocking its enzymatic activity. This binding is reversible, meaning that the drug can effectively modulate the activity of plasma kallikrein without permanently deactivating it. The selectivity of Berotralstat Hydrochloride ensures that it does not interfere with other proteases, minimizing potential side effects and enhancing its safety profile.
Pharmacokinetically, Berotralstat Hydrochloride is administered orally, providing convenience over other treatments that require intravenous or subcutaneous routes. Upon ingestion, the drug is absorbed through the gastrointestinal tract and reaches peak plasma concentrations within a few hours. Its bioavailability is influenced by food intake, with a high-fat meal increasing the absorption rate. Once in the bloodstream, Berotralstat Hydrochloride distributes relatively evenly across tissues, maintaining therapeutic concentrations.
Metabolism of Berotralstat Hydrochloride occurs primarily in the liver, where it undergoes biotransformation through pathways involving cytochrome P450 enzymes, specifically CYP3A4. This metabolism results in the formation of inactive metabolites, which are then excreted via urine and feces. The half-life of Berotralstat Hydrochloride is conducive to once-daily dosing, enhancing patient compliance and ensuring a consistent therapeutic effect.
Clinical trials have demonstrated the efficacy of Berotralstat Hydrochloride in reducing the frequency and severity of HAE attacks. Patients treated with this drug have shown significant improvement in symptom control, which translates to a better quality of life. Moreover, the adverse effects associated with Berotralstat Hydrochloride are generally mild to moderate, with the most common being gastrointestinal disturbances, such as nausea and diarrhea.
In summary, Berotralstat Hydrochloride offers a targeted approach to managing hereditary angioedema by inhibiting plasma kallikrein and subsequently reducing bradykinin levels. Its oral administration, selective mechanism of action, and favorable safety profile make it a valuable addition to the therapeutic options available for HAE patients. Understanding its mechanism provides insights into how modern pharmacological interventions can effectively address the underlying causes of genetic disorders, paving the way for more tailored and efficient treatments.
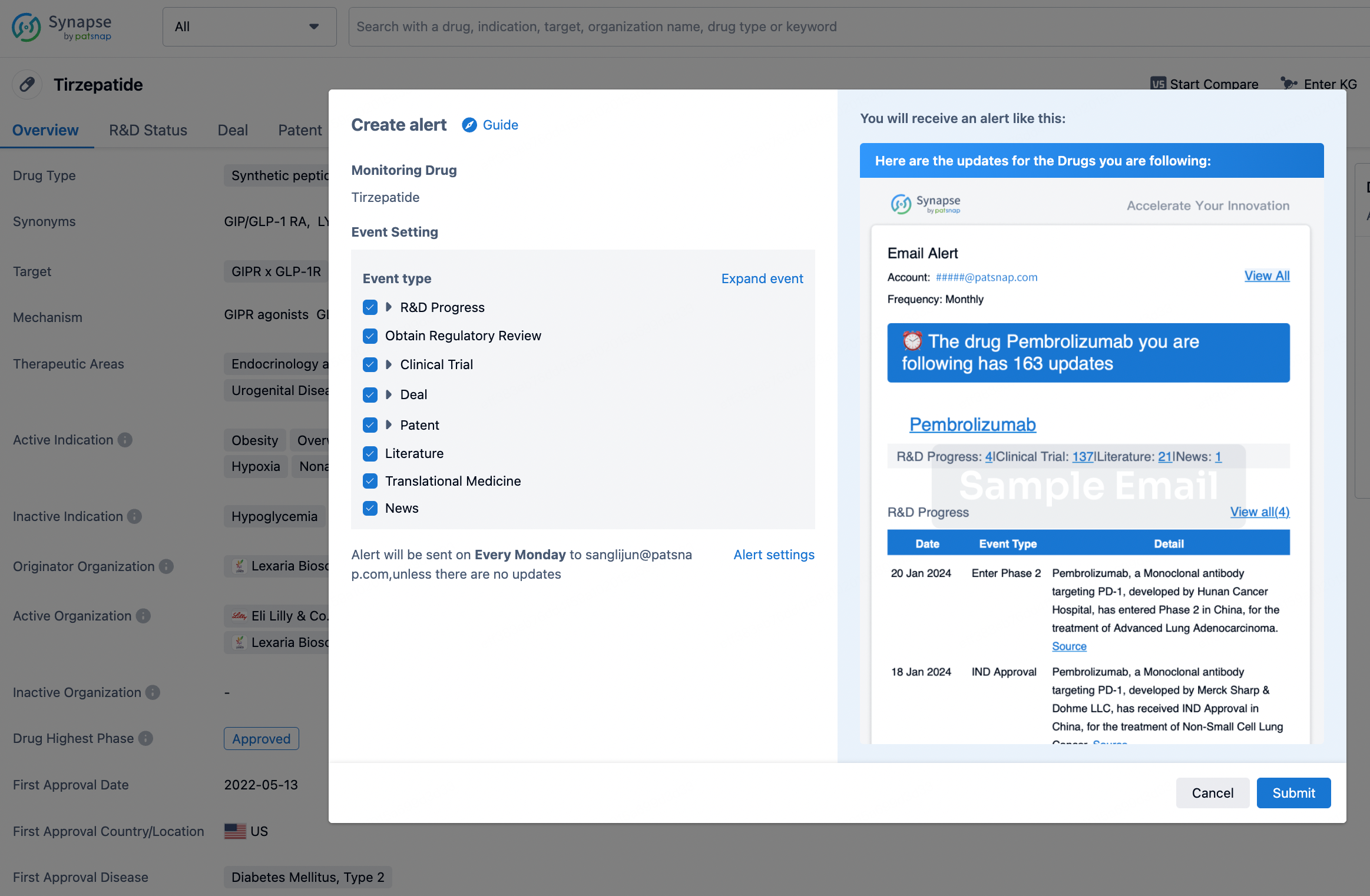
How to obtain the latest development progress of all drugs?
In the Synapse database, you can stay updated on the latest research and development advances of all drugs. This service is accessible anytime and anywhere, with updates available daily or weekly. Use the "Set Alert" function to stay informed. Click on the image below to embark on a brand new journey of drug discovery!
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.