Request Demo
What is the mechanism of Eprosartan Mesylate?
17 July 2024
Eprosartan Mesylate is an antihypertensive medication classified as an angiotensin II receptor blocker (ARB). Its primary mechanism of action involves the inhibition of the renin-angiotensin-aldosterone system (RAAS), which plays a crucial role in regulating blood pressure and fluid balance.
Angiotensin II is a potent vasoconstrictive peptide that exerts its effects by binding to angiotensin II type 1 (AT1) receptors located on the surface of various cell types, including vascular smooth muscle cells, adrenal gland cells, and renal cells. When angiotensin II binds to AT1 receptors, it triggers a cascade of events leading to vasoconstriction, aldosterone secretion, sodium retention, and water reabsorption. These actions collectively contribute to an increase in blood pressure.
Eprosartan Mesylate functions by selectively blocking the binding of angiotensin II to AT1 receptors. By occupying these receptors, eprosartan prevents angiotensin II from exerting its vasoconstrictive effects. Consequently, this leads to vasodilation, or the widening of blood vessels, which lowers peripheral vascular resistance and ultimately reduces blood pressure.
In addition to vasodilation, the blockade of AT1 receptors by eprosartan decreases aldosterone secretion from the adrenal cortex. Aldosterone is a hormone that promotes sodium and water retention in the kidneys. By reducing aldosterone levels, eprosartan facilitates the excretion of sodium and water, thereby decreasing blood volume and further contributing to the lowering of blood pressure.
Unlike angiotensin-converting enzyme (ACE) inhibitors, which also target the RAAS but inhibit the conversion of angiotensin I to angiotensin II, ARBs like eprosartan do not interfere with the breakdown of bradykinin. Bradykinin is a peptide that promotes vasodilation and can cause side effects such as a persistent dry cough when its breakdown is inhibited. As a result, eprosartan and other ARBs tend to have a lower incidence of cough and angioedema compared to ACE inhibitors.
Eprosartan Mesylate is typically administered orally and has a favorable pharmacokinetic profile. After ingestion, it is absorbed into the bloodstream and reaches peak plasma concentrations within a few hours. The drug is metabolized primarily in the liver and excreted via the bile and urine. It has a relatively long half-life, which allows for once-daily dosing in most patients.
Clinical trials have demonstrated the efficacy of eprosartan in reducing blood pressure in patients with hypertension. It is often prescribed as monotherapy or in combination with other antihypertensive agents, such as diuretics or calcium channel blockers, to achieve optimal blood pressure control. Moreover, eprosartan has shown beneficial effects on cardiovascular outcomes, including a reduction in the risk of stroke and myocardial infarction in high-risk individuals.
In summary, Eprosartan Mesylate exerts its antihypertensive effects by selectively blocking the AT1 receptors, thereby inhibiting the actions of angiotensin II. This leads to vasodilation, reduced aldosterone secretion, and decreased blood volume, all of which contribute to lower blood pressure. Its favorable side effect profile and efficacy make it a valuable option in the management of hypertension and the prevention of cardiovascular events.
Angiotensin II is a potent vasoconstrictive peptide that exerts its effects by binding to angiotensin II type 1 (AT1) receptors located on the surface of various cell types, including vascular smooth muscle cells, adrenal gland cells, and renal cells. When angiotensin II binds to AT1 receptors, it triggers a cascade of events leading to vasoconstriction, aldosterone secretion, sodium retention, and water reabsorption. These actions collectively contribute to an increase in blood pressure.
Eprosartan Mesylate functions by selectively blocking the binding of angiotensin II to AT1 receptors. By occupying these receptors, eprosartan prevents angiotensin II from exerting its vasoconstrictive effects. Consequently, this leads to vasodilation, or the widening of blood vessels, which lowers peripheral vascular resistance and ultimately reduces blood pressure.
In addition to vasodilation, the blockade of AT1 receptors by eprosartan decreases aldosterone secretion from the adrenal cortex. Aldosterone is a hormone that promotes sodium and water retention in the kidneys. By reducing aldosterone levels, eprosartan facilitates the excretion of sodium and water, thereby decreasing blood volume and further contributing to the lowering of blood pressure.
Unlike angiotensin-converting enzyme (ACE) inhibitors, which also target the RAAS but inhibit the conversion of angiotensin I to angiotensin II, ARBs like eprosartan do not interfere with the breakdown of bradykinin. Bradykinin is a peptide that promotes vasodilation and can cause side effects such as a persistent dry cough when its breakdown is inhibited. As a result, eprosartan and other ARBs tend to have a lower incidence of cough and angioedema compared to ACE inhibitors.
Eprosartan Mesylate is typically administered orally and has a favorable pharmacokinetic profile. After ingestion, it is absorbed into the bloodstream and reaches peak plasma concentrations within a few hours. The drug is metabolized primarily in the liver and excreted via the bile and urine. It has a relatively long half-life, which allows for once-daily dosing in most patients.
Clinical trials have demonstrated the efficacy of eprosartan in reducing blood pressure in patients with hypertension. It is often prescribed as monotherapy or in combination with other antihypertensive agents, such as diuretics or calcium channel blockers, to achieve optimal blood pressure control. Moreover, eprosartan has shown beneficial effects on cardiovascular outcomes, including a reduction in the risk of stroke and myocardial infarction in high-risk individuals.
In summary, Eprosartan Mesylate exerts its antihypertensive effects by selectively blocking the AT1 receptors, thereby inhibiting the actions of angiotensin II. This leads to vasodilation, reduced aldosterone secretion, and decreased blood volume, all of which contribute to lower blood pressure. Its favorable side effect profile and efficacy make it a valuable option in the management of hypertension and the prevention of cardiovascular events.
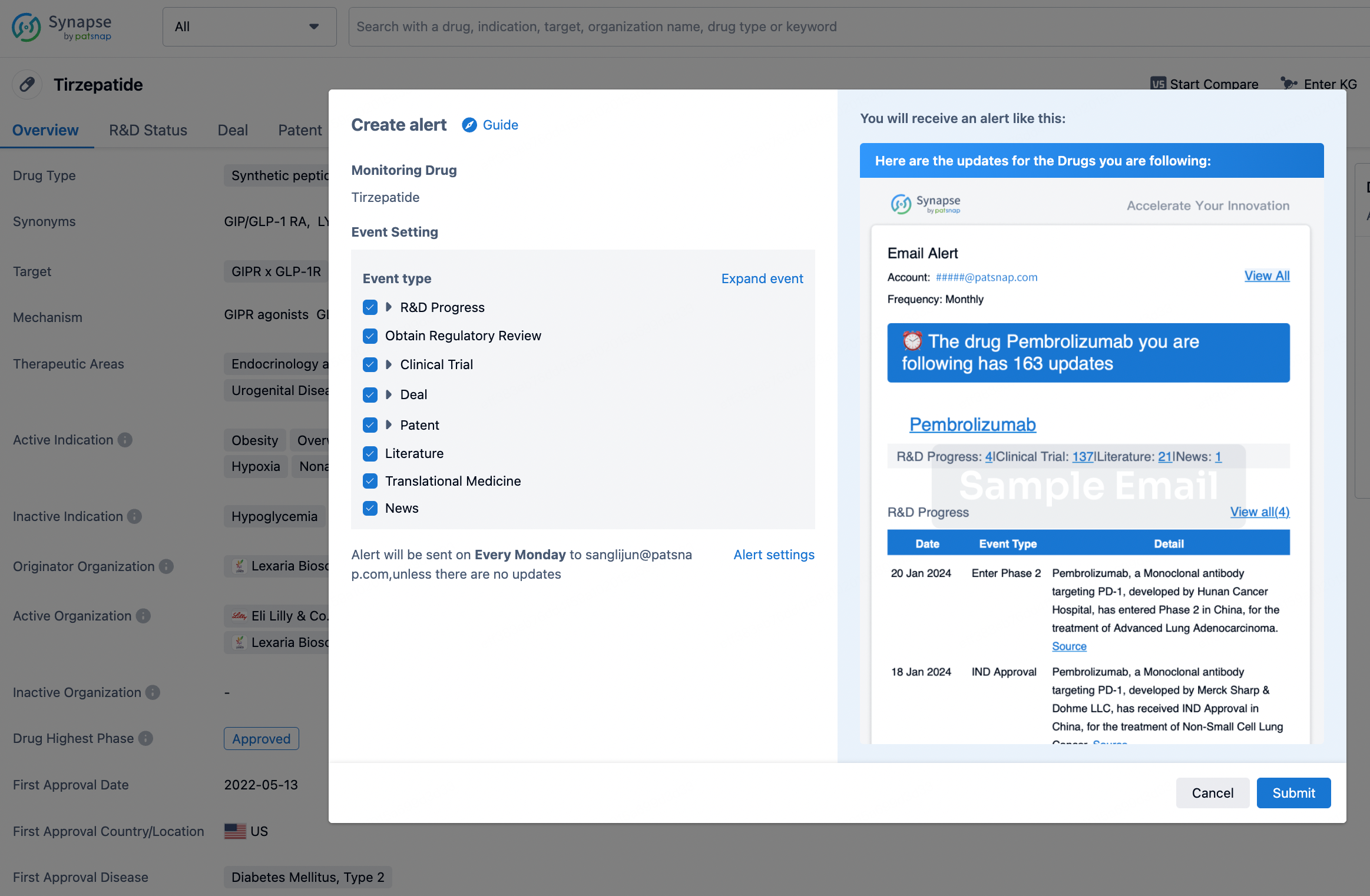
How to obtain the latest development progress of all drugs?
In the Synapse database, you can stay updated on the latest research and development advances of all drugs. This service is accessible anytime and anywhere, with updates available daily or weekly. Use the "Set Alert" function to stay informed. Click on the image below to embark on a brand new journey of drug discovery!
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.