Request Demo
Last update 06 Dec 2025
BCMA CAR-T Cells(Hebei Senlangbio Biotechnology)
Last update 06 Dec 2025
Overview
Basic Info
Drug Type CAR-T |
Synonyms- |
Target |
Action modulators |
Mechanism BCMA modulators(B-cell maturation protein modulators) |
Therapeutic Areas |
Active Indication |
Inactive Indication |
Originator Organization |
Active Organization |
Inactive Organization- |
License Organization- |
Drug Highest PhaseClinical |
First Approval Date- |
Regulation- |
Login to view timeline
Related
3
Clinical Trials associated with BCMA CAR-T Cells(Hebei Senlangbio Biotechnology)NCT05618041
The Safety and Efficay Investigation of CAR-T Cell Therapy for Patients With Hematological Malignancies
NCT04447573
Immunotherapy With BCMA CAR-T Cells in Treating Patients With Relapsed or Refractory Multiple Myeloma
NCT04626752
An Open, Uncontrolled, Multicenter Clinical Trial to Explore the Safety, Efficacy, and Remission Phase of Chimeric Antigen Receptor T Cell (CAR-T) in the Treatment of Relapsed Refractory (R/R) Multiple Myeloma (MM)
100 Clinical Results associated with BCMA CAR-T Cells(Hebei Senlangbio Biotechnology)
Login to view more data
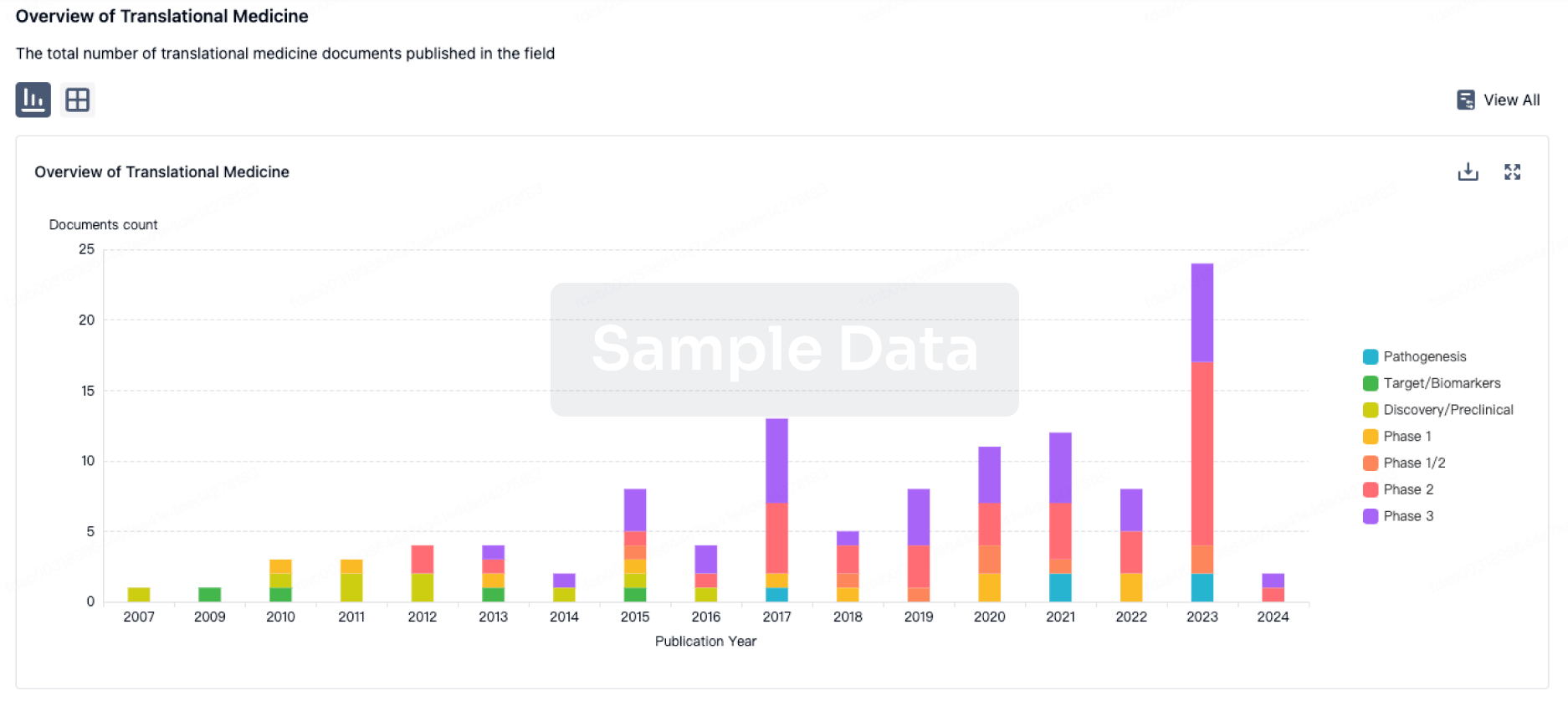
100 Translational Medicine associated with BCMA CAR-T Cells(Hebei Senlangbio Biotechnology)
Login to view more data
100 Patents (Medical) associated with BCMA CAR-T Cells(Hebei Senlangbio Biotechnology)
Login to view more data
22
Literatures (Medical) associated with BCMA CAR-T Cells(Hebei Senlangbio Biotechnology)23 Sep 2025Blood Advances
Efficacy and safety of BCMA nanobody CAR T-cell therapy in relapsed or refractory plasma cell myeloma
Article
Author: Wang, Hui ; Wang, Qinglong ; Hu, Xiaona N. ; Zhang, Xian ; Yang, Junfang ; Zhou, Xiaoge ; Wang, Lin ; Lu, Pei H. ; Zhang, Lina N. ; Liu, Ying
Abstract:
B-cell maturation antigen (BCMA) chimeric antigen receptor (CAR) T-cell therapy has demonstrated promising therapeutic efficacy in relapsed or refractory (R/R) multiple myeloma. However, distinct CAR T-cell constructs exhibit varying therapeutic outcomes. As the antigen-recognition domain, nanobodies offer a small, stable, single-domain structure with enhanced affinity and specificity compared with conventional single-chain variable fragments. We explored the use of nanobody-based BCMA(S103) CAR T-cell therapy for R/R plasma cell myeloma. The CAR construct incorporates dual-nanobody variable domain of the heavy chain of heavy chain antibody (VHHs) targeting BCMA. A cohort of 27 patients was treated with S103 CAR T-cell therapy, which included 4 patients of plasma cell leukemia, and 1 patient of anaplastic plasma cell myeloma. Eleven patients had multiple extramedullary lesions, and 11 patients exhibited high-risk genetic abnormalities, including 4 with TP53 mutations. One month after CAR T-cell infusion, the overall response rate (ORR) was 96.3% (26/27), with a complete response (CR) + very good partial response (VGPR) rate of 59.2% (16/27). At the 3-month follow-up, the ORR increased to 100% (27/27), with a CR + VGPR rate of 81.5% (22/27). The median duration of remission was 11 months (range, 2-36 months). The 1-year overall survival rate was 61.1%, and progression-free survival was 57.2%. In conclusion, BCMA CAR T-cell therapy, utilizing dual-nanobody VHHs targeting BCMA, demonstrates a high ORR and manageable safety profile in treating patients with R/R plasmacytic myeloma, including those with high-risk features such as extramedullary lesions, high-risk cytogenetic abnormalities, plasma cell leukemia, or anaplastic plasmacytoma. This trial was registered at www.ClinicalTrials.gov as #NCT04447573.
01 Dec 2025Transplantation and Cellular Therapy
Impact of Gamma-Secretase Inhibition on Outcomes Following BCMA CAR-T Therapy in Multiple Myeloma: A Comparison of Two Phase 1 Trials
Article
Author: Riddell, Stanley R ; Pont, Margot J ; Blake, Michelle ; Works, Melissa G ; Green, Damian J ; Shadman, Mazyar ; Wu, Vicky Q ; Sather, Blythe D ; Wood, Brent L ; Liang, Emily C ; Gooley, Ted A ; Cowan, Andrew J ; Till, Brian G ; Song, Xiaoling ; Turtle, Cameron J ; Libby, Edward N ; Portuguese, Andrew J ; Chapuis, Aude G ; Coffey, David G ; Voutsinas, Jenna M ; Maloney, David G ; Cole, Gabriel O ; Milano, Filippo ; Tuazon, Sherilyn A ; Thomas, Sushma
BACKGROUND:
BCMA-directed chimeric antigen receptor (CAR)-T cell therapy represents a major therapeutic breakthrough for relapsed/refractory multiple myeloma (RRMM), offering deep and durable responses in heavily pretreated patients. However, a subset of patients experiences early relapse or fail to respond, highlighting the need for strategies to enhance efficacy. Gamma-secretase inhibitors (GSIs) have been shown to increase surface BCMA expression on malignant plasma cells and may potentiate the activity of BCMA CAR-T cells, particularly in patients with low baseline BCMA antigen density. Two contemporaneous phase 1 trials (FH9952 and FH9762) evaluated the fully human BCMA-targeted CAR-T product FCARH143, with FH9952 incorporating GSI co-administration.
OBJECTIVE:
To determine whether GSI use improves clinical outcomes following FCARH143 CAR-T therapy in RRMM, with particular focus on overall survival (OS), progression-free survival (PFS), and subgroup differences based on prior BCMA-targeted therapy and baseline tumor BCMA levels.
STUDY DESIGN:
This retrospective analysis compared outcomes from two single-arm, single-center phase 1 trials of the fully human BCMA-targeted CAR-T cell product FCARH143 in RRMM: FH9952 (n = 18), which incorporated the GSI crenigacestat, and FH9762 (n = 25), which did not. Both studies had extended follow-up beyond previously published reports. Eligible patients had measurable RRMM with ≥10% bone marrow plasma cell involvement and confirmed BCMA expression. BCMA-naïve patients were defined as those without prior exposure to BCMA-targeted therapies (e.g., BCMA CAR-T, bispecific antibodies, or antibody-drug conjugates); BCMA-exposed patients had received at least one such therapy. All participants received lymphodepletion with fludarabine and cyclophosphamide followed by infusion of FCARH143. In FH9952, crenigacestat (25 mg orally, three times weekly) was administered from day 0 through day +18. Outcomes included response rates, adverse events, OS, and PFS. Cox proportional hazards models were used for survival analysis.
RESULTS:
With extended follow-up (median 5.8 years), the overall cohort (n = 43) had a median OS of 2.7 years (95% CI 1.9-4.8) and median PFS of 1.1 years (95% CI 0.72-2.2). Baseline characteristics were generally similar, though BCMA-exposed status was more frequent in FH9952 (39% versus 8%). Rates of cytokine release syndrome, immune effector cell-associated neurotoxicity, and early immune effector cell-associated hematotoxicity were comparable between trials. Among BCMA-naïve patients (n = 34), GSI use was associated with improved OS (not reached versus 2.3 years; adjusted HR 0.30, 95% CI 0.10-0.88, P = .028) and a trend toward improved PFS (2.6 versus 1.3 years; adjusted HR 0.47, 95% CI 0.22-1.04, P = .062). No benefit was observed among BCMA-exposed patients. Exploratory spline modeling suggested GSI mitigated the adverse impact of low tumor BCMA levels, with inferior outcomes at low BCMA expression observed only in the non-GSI cohort.
CONCLUSIONS:
Co-administration of a GSI with BCMA CAR-T therapy was associated with improved survival in BCMA-naïve RRMM patients, particularly those with low baseline tumor BCMA levels. These findings suggest GSI modulation of BCMA surface expression may enhance CAR-T efficacy in select patients and support further prospective investigation.
01 Jun 2025NATURE MEDICINE
BCMA CAR T cells in a patient with relapsing idiopathic inflammatory myositis after initial and repeat therapy with CD19 CAR T cells
Article
Author: Müller, Fabian ; Wirsching, Andreas ; Grieshaber-Bouyer, Ricardo ; Spörl, Silvia ; Völkl, Simon ; Schett, Georg ; Hagen, Melanie ; Atzinger, Armin ; Böltz, Sebastian ; Zhang, Liang ; Bucci, Laura ; Kretschmann, Sascha ; Taubmann, Jule ; Mackensen, Andreas ; Raimondo, Maria Gabriella ; Tur, Carlo ; Eckstein, Markus ; Aigner, Michael ; Kharboutli, Soraya ; Munoz, Luis
Abstract:
CD19 chimeric antigen receptor (CD19 CAR) T cell therapy has been shown to induce stable drug-free remission in patients with refractory autoimmune disease. The management of potential relapses is currently unclear. Here we report on a 45-year-old woman with treatment-refractory Jo-1-associated anti-synthetase syndrome, who initially achieved disease remission after CD19 CAR T cell therapy but then experienced disease relapse after 9 months. After reinfusion of the same product, CAR T cells failed to expand and T cells targeting the CD19 CAR were detected. Despite full-dose lymphodepletion, no clinical response was observed. After bridging with anti-CD38 antibody daratumumab, which was efficacious with limited durability, plasma-cell-targeting B-cell maturation antigen (BCMA) CAR T cell therapy was performed. BCMA CAR T cells expanded, cleared plasma cells in lymphoid tissue, reduced autoantibody levels and re-induced stable drug-free remission. This case highlights the challenges in CAR T cell reinfusion, the potential of alternative targets and products, and suggests that the depletion of plasma cells may enhance therapeutic outcomes in patients who become treatment-refractory.
100 Deals associated with BCMA CAR-T Cells(Hebei Senlangbio Biotechnology)
Login to view more data
R&D Status
10 top R&D records. to view more data
Login
| Indication | Highest Phase | Country/Location | Organization | Date |
|---|---|---|---|---|
| Refractory Multiple Myeloma | Phase 1 | China | 01 Apr 2020 | |
| Relapse multiple myeloma | Phase 1 | China | 01 Apr 2020 | |
| Acute Lymphoblastic Leukemia | Clinical | China | 07 Sep 2022 |
Login to view more data
Clinical Result
Clinical Result
Indication
Phase
Evaluation
View All Results
Phase 1 | 27 | BCMA CAR T-cell therapy | ooyvhntwai(osmqxnlskz) = fcygtcdluw aasybruibq (jzaozevvcx ) View more | Positive | 23 Sep 2025 |

Login to view more data
Translational Medicine
Boost your research with our translational medicine data.
login
or
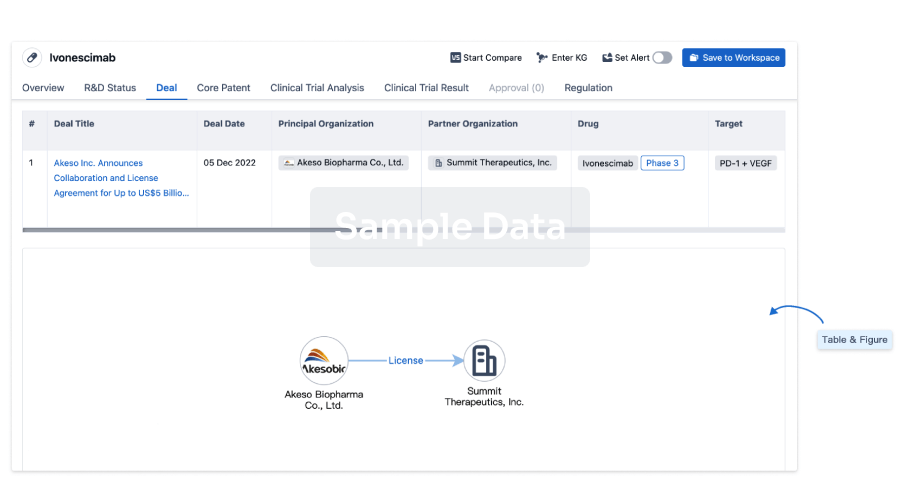
Deal
Boost your decision using our deal data.
login
or
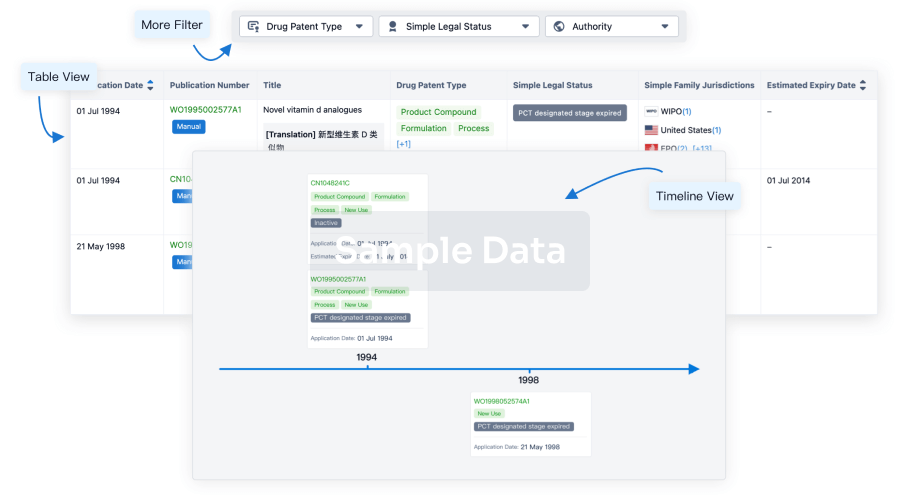
Core Patent
Boost your research with our Core Patent data.
login
or
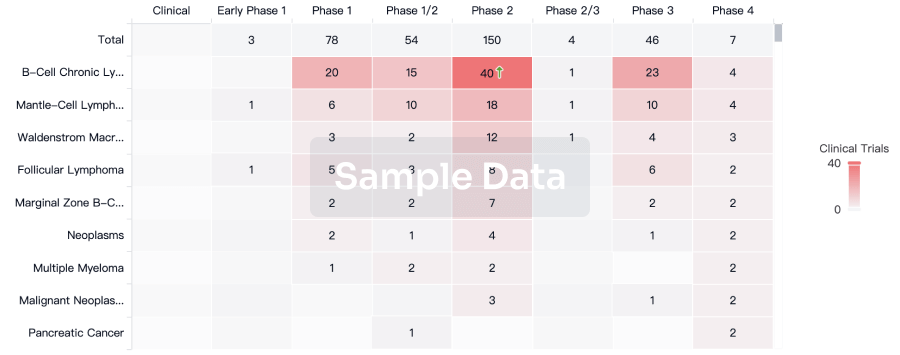
Clinical Trial
Identify the latest clinical trials across global registries.
login
or
Approval
Accelerate your research with the latest regulatory approval information.
login
or
Regulation
Understand key drug designations in just a few clicks with Synapse.
login
or
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free