Request Demo
Last update 15 Jul 2026
Amivantamab-VMJM
Last update 15 Jul 2026
Overview
Basic Info
Drug Type Bispecific antibody |
Synonyms Amivantamab, amivantamab-vmjw, Amivantamab(Genetical Recombination) + [15] |
Target |
Action antagonists, inhibitors |
Mechanism EGFR antagonists(Epidermal growth factor receptor erbB1 antagonists), c-Met inhibitors(Hepatocyte growth factor receptor inhibitors) |
Therapeutic Areas |
Inactive Indication |
Originator Organization |
Inactive Organization |
License Organization |
Drug Highest PhaseApproved |
First Approval Date United States (21 May 2021), |
RegulationBreakthrough Therapy (United States), Accelerated Approval (United States), Orphan Drug (South Korea), Breakthrough Therapy (China), Priority Review (United States) |


Login to view timeline
Structure/Sequence
Sequence Code 143885L
Source: *****
Sequence Code 13387733H
Source: *****
Sequence Code 13387743H
Source: *****
Sequence Code 13387747L
Source: *****
Related
51
Clinical Trials associated with Amivantamab-VMJMNCT07586202
A Phase 2 Study Evaluating the Safety and Efficacy of Neoadjuvant Amivantamab in Combination With Lazertinib or Chemotherapy in Resectable EGFR-Mutated Non-Small Cell Lung Cancer
NCT07507188
Collaborative Clinical-translational Cohort of Amivantamab Plus Lazertinib and Amivantamab Plus Chemotherapy in Patients With EGFR-mutant, Locally Advanced or Metastatic/Recurrent Non-Small Cell Lung Cancer (INSTAR Study)
NCT07062354
A Phase II Study of Combined Amivantamab, Carboplatin and Paclitaxel in Unresectable Locally Recurrent or Metastatic Head and Neck Cancer
100 Clinical Results associated with Amivantamab-VMJM
Login to view more data
100 Translational Medicine associated with Amivantamab-VMJM
Login to view more data
100 Patents (Medical) associated with Amivantamab-VMJM
Login to view more data
300
Literatures (Medical) associated with Amivantamab-VMJM31 Dec 2026JOURNAL OF MEDICAL ECONOMICS
Cost comparison of osimertinib plus platinum-pemetrexed versus amivantamab plus lazertinib for the first-line treatment of patients with locally advanced or metastatic epidermal growth factor receptor-mutated non-small cell lung cancer
Article
Author: Upton, Elysia ; Hearmon, Natalie ; Procter, Emily ; Nieva, Jorge J. ; Rattigan-Brown, Yanique ; Freeman, Harry ; Lopes, Gilberto de Lima ; Karia, Pritesh
OBJECTIVES:
Novel first-line (1L) combination regimens offer improved efficacy for patients with epidermal growth factor receptor-mutated (EGFRm) locally advanced or metastatic non-small cell lung cancer (NSCLC) versus the standard of care, but their costs have not been comprehensively evaluated. Total and differential costs of 1L osimertinib plus platinum-pemetrexed, intravenous (IV) amivantamab plus lazertinib, and subcutaneous (SC) amivantamab plus lazertinib were estimated from a United States (US) payer perspective.
METHODS:
A cost of care model was developed to assess treatment acquisition, administration, disease management, and adverse event (AE) management costs for osimertinib plus platinum-pemetrexed versus IV and SC amivantamab plus lazertinib for patients with EGFRm NSCLC. A one-year time horizon was chosen to allow for direct treatment comparison; a one-year treatment duration was assumed for treat-to-progression regimen components.
RESULTS:
The total first-year cost per-patient for osimertinib plus platinum-pemetrexed (all-payer perspective: $172,600; private perspective: $253,529; Medicare perspective: $84,926) was over twofold lower than for IV amivantamab plus lazertinib (all-payer perspective: $418,176; private perspective: $618,240; Medicare perspective: $201,441) and for SC amivantamab plus lazertinib (all-payer perspective: $419,718; private perspective: $621,166; Medicare perspective: $201,482). This translated to per-patient cost savings of $245,577; $364,711; and $116,514 for osimertinib plus platinum-pemetrexed versus IV amivantamab plus lazertinib and $247,118; $367,637; and $116,555 versus SC amivantamab plus lazertinib for the all-payer, private, and Medicare perspectives, respectively.
LIMITATIONS:
Limited data availability necessitated cost conversions across payer perspectives and assumptions for select inputs, including specific concomitant medication durations. Additionally, as any payer-negotiated discounts for treatment are confidential, model treatment acquisition costs reflected list prices. These data limitations contributed to uncertainty surrounding model inputs.
CONCLUSIONS:
From a US payer perspective, osimertinib plus platinum-pemetrexed was associated with substantially lower overall costs compared with IV and SC amivantamab plus lazertinib for the 1L treatment of patients with EGFRm locally advanced or metastatic NSCLC.
01 Sep 2026ORAL ONCOLOGY
Intravenous amivantamab after cetuximab failure in recurrent or metastatic head and neck squamous cell carcinoma: a single-centre retrospective real-world cohort study
Article
Author: Lin, Fengjuan ; Xue, Liqiong ; Guo, Ye ; Zhao, Wei ; Tang, Wenbo ; Zhou, Jiuli
BACKGROUND:
Patients with recurrent or metastatic head and neck squamous cell carcinoma (R/M HNSCC) who exhaust platinum, immune checkpoint inhibitors (ICIs), and cetuximab lack standard options. The OrigAMI-4 trial showed subcutaneous amivantamab activity in anti-EGFR-naïve patients; real-world intravenous (IV) amivantamab data after cetuximab failure are absent.
METHODS:
We retrospectively analysed consecutive R/M HNSCC patients treated with IV amivantamab monotherapy (November 2024-July 2025) after progression on standard therapies. Response was assessed per RECIST 1.1; toxicity per CTCAE v5.0.
RESULTS:
Twenty patients were included (median age 54 years; 70.0% male; median four prior systemic lines). All received prior platinum and ICIs; 18 (90.0%) progressed on cetuximab. At a median follow-up of 6.8 months, confirmed ORR was 30.0% (6/20; 95% CI 11.9-54.3) ; DCR at first reassessment (6 weeks) was 80.0% (16/20; 95% CI 56.3-94.3) and confirmed DCR at 12 weeks was 45.0% (9/20; 95% CI 23.1-68.5). Median PFS was 3.0 months (95% CI 2.3 to not reached) and median OS 9.7 months (95% CI 6.8 to not reached). The most frequent treatment-related adverse events were hypoalbuminaemia (90.0%), rash (70.0%), and infusion-related reactions (45.0%; all grade 1-2); two patients had grade 3 events, none discontinued treatment.
CONCLUSION:
In this small retrospective cohort, IV amivantamab showed antitumour activity in heavily pretreated, cetuximab-exposed R/M HNSCC, with a 30% confirmed ORR, 45% confirmed 12-week DCR, 9.7-month median OS, and no treatment discontinuations for toxicity. These data suggest that dual EGFR-MET targeting may retain clinical utility after anti-EGFR failure, and support prospective evaluation with biomarker stratification.
01 Aug 2026CRITICAL REVIEWS IN ONCOLOGY HEMATOLOGY
Immunotherapeutic strategies in HPV-positive and HPV-negative recurrent/metastatic oropharyngeal squamous cell carcinoma: From PD-1 blockade to EGFR-directed bispecifics and therapeutic HPV vaccines
Review
Author: Del Mastro, Lucia ; Gili, Riccardo ; Caterino, Marianna ; Di Bello, Armando ; Cassano, Alessandra ; Bassolino, Antonio ; Fasano, Morena ; Polidori, Sara ; Falcicchia, Renato ; Tortora, Giampaolo
Oropharyngeal squamous cell carcinoma (OPSCC) comprises two biologically distinct entities, HPV-positive and HPV-negative disease, which differ in etiology, immune microenvironment, molecular drivers, and clinical behavior. This narrative review summarizes current evidence on immunotherapeutic strategies in OPSCC, focusing on subtype-specific biological rationale and emerging treatment approaches. A literature search of PubMed/MEDLINE, Embase, Cochrane Library, ClinicalTrials.gov, and major oncology meeting abstracts was conducted for studies published from January 2000 to February 2026. PD-1/PD-L1 inhibitors represent the current standard of care in recurrent/metastatic disease, with HPV-positive tumors generally showing more favorable outcomes, likely reflecting a more inflamed and antigen-rich tumor microenvironment. However, HPV status remains primarily a prognostic rather than a validated predictive biomarker for checkpoint inhibitor benefit. In contrast, HPV-negative OPSCC is more frequently characterized by immune exclusion, EGFR dependence, hypoxia, and activation of MET/HGF and TGF-β pathways, supporting the development of EGFR-centered and bifunctional strategies to overcome resistance. Emerging agents such as ficerafusp alfa, petosemtamab, and amivantamab have demonstrated promising early clinical activity, particularly in biomarker-enriched or post-immunotherapy settings. In HPV-positive disease, therapeutic vaccines targeting E6/E7 oncoproteins have shown encouraging immunogenicity and preliminary antitumor activity, especially when combined with PD-1 blockade. Overall, the immunotherapeutic landscape of OPSCC is evolving toward a biomarker-driven framework integrating viral status, immune contexture and pathway activation to enable more precise and personalized treatment strategies.
361
News (Medical) associated with Amivantamab-VMJM14 Jul 2026
License out/inDrug ApprovalPhase 3
22 Jun 2026
Phase 3Drug ApprovalCell TherapyImmunotherapyPhase 2
100 Deals associated with Amivantamab-VMJM
Login to view more data
External Link
| KEGG | Wiki | ATC | Drug Bank |
|---|---|---|---|
| - | Amivantamab-VMJM | - |
R&D Status
Approved
10 top approved records. to view more data
Login
| Indication | Country/Location | Organization | Date |
|---|---|---|---|
| EGFR positive non-small cell lung cancer | Japan | 27 Mar 2025 | |
| EGFR exon 19 Deletions Mutant Non-small Cell Lung Cancer | United States | 19 Aug 2024 | |
| EGFR exon 21 Substitution Mutant Non-small Cell Lung Cancer | United States | 19 Aug 2024 | |
| Non-Small Cell Lung Cancer | Canada | 30 Mar 2022 | |
| EGFR ex20ins mutation in non-small cell lung cancer | United States | 21 May 2021 |
Developing
10 top R&D records. to view more data
Login
| Indication | Highest Phase | Country/Location | Organization | Date |
|---|---|---|---|---|
| EGFR-mutated non-small Cell Lung Cancer | NDA/BLA | China | 26 Jan 2024 | |
| EGFR-mutated non-small Cell Lung Cancer | NDA/BLA | China | 26 Jan 2024 | |
| EGFR-mutated non-small Cell Lung Cancer | NDA/BLA | China | 26 Jan 2024 | |
| Recurrent Squamous Cell Carcinoma of the Head and Neck | Phase 3 | United States | 03 Dec 2025 | |
| Recurrent Squamous Cell Carcinoma of the Head and Neck | Phase 3 | China | 03 Dec 2025 | |
| Recurrent Squamous Cell Carcinoma of the Head and Neck | Phase 3 | Japan | 03 Dec 2025 | |
| Recurrent Squamous Cell Carcinoma of the Head and Neck | Phase 3 | Australia | 03 Dec 2025 | |
| Recurrent Squamous Cell Carcinoma of the Head and Neck | Phase 3 | Austria | 03 Dec 2025 | |
| Recurrent Squamous Cell Carcinoma of the Head and Neck | Phase 3 | Belgium | 03 Dec 2025 | |
| Recurrent Squamous Cell Carcinoma of the Head and Neck | Phase 3 | Brazil | 03 Dec 2025 |

Login to view more data
Clinical Result
Clinical Result
Indication
Phase
Evaluation
View All Results
Phase 1/2 | RAS/BRAF Wild Type Colorectal Cancer Third line RAS / BRAF / EGFR ectodomain wild-type | ERBB2/HER2 amplification | 94 | (cohort A) | wphcwnekxa(rusfkwgncp) = lrajyqcxoe veclbuybhl (ydjbvwoqpd ) View more | Positive | 10 Jun 2026 | |
(cohort B) | wphcwnekxa(rusfkwgncp) = ceivsbbule veclbuybhl (ydjbvwoqpd ) View more | ||||||
Phase 1/2 | 102 | vjyafxgdnp(xvctgwdngy) = ivnvuclwse ofviciruly (qzywqfklzh, 37 - 57) View more | Positive | 29 May 2026 | |||
Phase 1 | 49 | ybmctkuhea(bvzodlyhew) = enjduuyteq qjnzdwcozs (gfhvxzqnnw, 27.7 - NE) View more | Positive | 29 May 2026 | |||
Not Applicable | EGFR positive non-small cell lung cancer Second line | 22 | Amivantamab monotherapy | bafsaendyv(agsofyvdhp) = sizssrsnji dawpyboozo (xxflrcfspq, 36.1 - 80.9) View more | Positive | 29 May 2026 | |
Amivantamab monotherapy (classical EGFR) | bafsaendyv(agsofyvdhp) = cmylhpletw dawpyboozo (xxflrcfspq ) View more | ||||||
Phase 2 | 70 | (advanced or recurrent non-squamous NSCLC with uncommon or compound EGFR mutations + treatment-naïve) | dyjoilpdrx(buurogongo) = pbqsaaswyq jyxdirjwua (fmeymgoyzg ) View more | Positive | 29 May 2026 | ||
(advanced or recurrent non-squamous NSCLC with uncommon or compound EGFR mutations + treatment-naïve) | dyjoilpdrx(buurogongo) = gehtgdhkbk jyxdirjwua (fmeymgoyzg ) View more | ||||||
Phase 1/2 | RAS/BRAF Wild Type Colorectal Cancer RAS/BRAF wild-type | 73 | (CMS2) | cmclzqusrt(sbdgpnjnwr) = ywbgmuurei qxsbwawwwb (gtvfjsjgki ) View more | Positive | 29 May 2026 | |
(CMS4) | cmclzqusrt(sbdgpnjnwr) = shdugbjtup qxsbwawwwb (gtvfjsjgki ) View more | ||||||
Phase 2 | 190 | kiimpqzwly(xposgzyvdc) = fipqnmwkoj uesggfutbp (fhxpgrwrps ) View more | Positive | 29 May 2026 | |||
Not Applicable | 4,909 | nnbpvdcrfu(itgmjsiqcb): HR = 1.92 View more | Positive | 29 May 2026 | |||
immunotherapy +Chemo (IC) | |||||||
Not Applicable | - | 15 | hmbbznlyhp(ubdiwzsswo) = rnkchdmbpi ygpdunsmhm (warbwstghy ) View more | Positive | 29 May 2026 | ||
Phase 2 | 21 | buumylpecq = fpgtdiuspz dlykphbuqt (xkfmughcaf, xvmzgrhohv - ycipjuwsjc) View more | - | 08 May 2026 |
Login to view more data
Translational Medicine
Boost your research with our translational medicine data.
login
or

Deal
Boost your decision using our deal data.
login
or

Core Patent
Boost your research with our Core Patent data.
login
or

Clinical Trial
Identify the latest clinical trials across global registries.
login
or

Approval
Accelerate your research with the latest regulatory approval information.
login
or

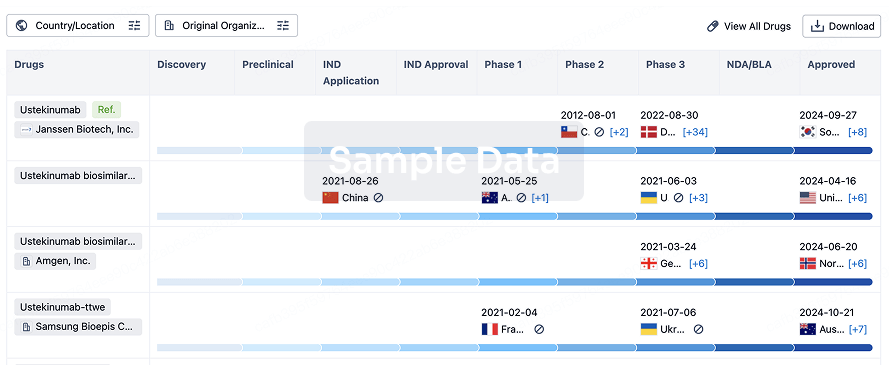
Biosimilar
Competitive landscape of biosimilars in different countries/locations. Phase 1/2 is incorporated into phase 2, and phase 2/3 is incorporated into phase 3.
login
or
Regulation
Understand key drug designations in just a few clicks with Synapse.
login
or

AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free