Request Demo
Last update 08 May 2025
Tc-94m Sestamibi
Last update 08 May 2025
Overview
Basic Info
Originator Organization |
Active Organization- |
Inactive Organization |
License Organization- |
Drug Highest PhasePendingPhase 2 |
First Approval Date- |
Regulation- |

Login to view timeline
Related
3
Clinical Trials associated with Tc-94m SestamibiNCT05042687
Comparative Performance of Molecular Breast Imaging (MBI) to Magnetic Resonance Imaging (MRI) of the Breast in Identifying and Excluding Breast Carcinoma in Women at High Risk for Breast Cancer

NCT02324387
Assessment of the Tumor Response to Neoadjuvant Chemotherapy in Women With Locoregional Invasive Breast Cancer Using Tc99m Sestamibi Molecular Breast Imaging: A Prospective Study
NCT00082368
A Pilot Study of Tc-94m Sestamibi PET MDR Imaging
100 Clinical Results associated with Tc-94m Sestamibi
Login to view more data
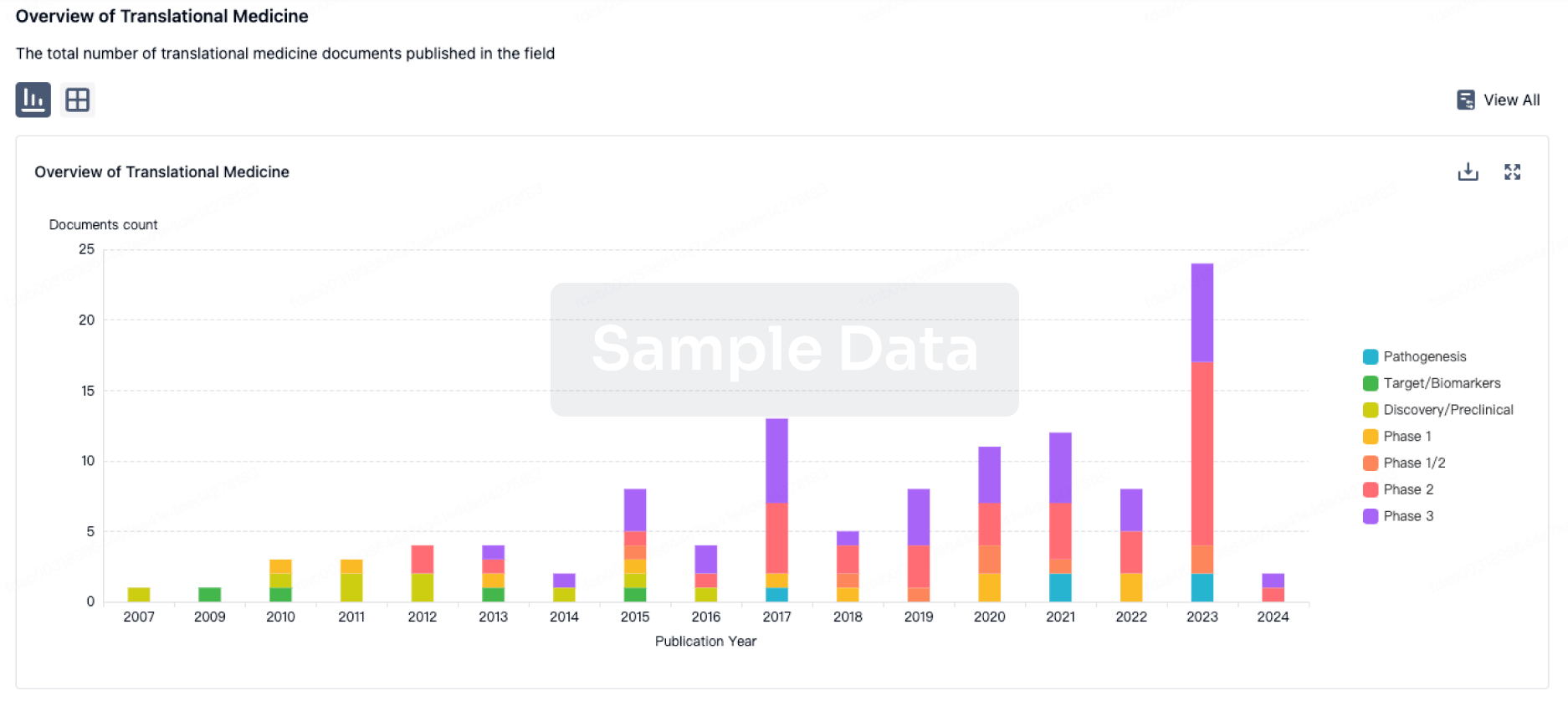
100 Translational Medicine associated with Tc-94m Sestamibi
Login to view more data
100 Patents (Medical) associated with Tc-94m Sestamibi
Login to view more data
34
Literatures (Medical) associated with Tc-94m Sestamibi01 Aug 2024JAMA Otolaryngology–Head & Neck Surgery
A Diagnostic Randomized Clinical Trial
Article
Author: Grellard, Jean-Michel ; Quak, Elske ; Ciappuccini, Renaud ; Bastit, Vianney ; Christy, François ; Roudaut, Nathalie ; Lireux, Barbara ; Guery, Clémence ; Clarisse, Bénédicte ; Legrand, Bérénice ; Lasne-Cardon, Audrey ; Bardet, Stéphane ; Estienne, Adrien ; Salaun, Pierre-Yves ; Devillers, Anne ; Esvant, Annabelle ; Jegoux, Franck ; Keromnes, Nathalie ; Lasnon, Charline ; Vaduva, Patricia ; Potard, Gaël ; Cavarec, Marie ; de Crouy-Chanel, Olivier
01 Jan 2023Acta Clinica Croatica
Parathyroid Carcinoma: Ultrasonographic and Clinical Experience
Article
Author: Huić, Dražen ; Jadrešić, Marina ; Kusačić Kuna, Sanja ; Tomić Brzac, Hrvojka ; Baretić, Maja
01 Jun 2022IJC Heart & Vasculature
Mechanical dispersion combined with global longitudinal strain estimated by three dimensional speckle tracking in patients with ST elevation myocardial infarction
Article
Author: Tamura, Kouichi ; Iwahashi, Noriaki ; Minamimoto, Yugo ; Hibi, Kiyoshi ; Okada, Kozo ; Takahashi, Hironori ; Horii, Mutsuo ; Kirigaya, Jin ; Kirigaya, Hidekuni ; Ebina, Toshiaki ; Gohbara, Masaomi ; Kosuge, Masami ; Toya, Noriko ; Hanajima, Yohei ; Matsuzawa, Yasushi ; Kimura, Kazuo ; Kimura, Yuichiro ; Abe, Takeru
100 Deals associated with Tc-94m Sestamibi
Login to view more data
R&D Status
10 top R&D records. to view more data
Login
| Indication | Highest Phase | Country/Location | Organization | Date |
|---|---|---|---|---|
| Neoplasms | Phase 2 | United States | 16 May 2004 |
Login to view more data
Clinical Result
Clinical Result
Indication
Phase
Evaluation
View All Results
Phase 2 | 12 | zmhuexvlaf(junjfbtgaz) = tusfzifocv aasmagppnm (hdeoruqdyv, zmwrvpglat - ucyrcfwrgs) View more | - | 04 May 2015 |
Login to view more data
Translational Medicine
Boost your research with our translational medicine data.
login
or
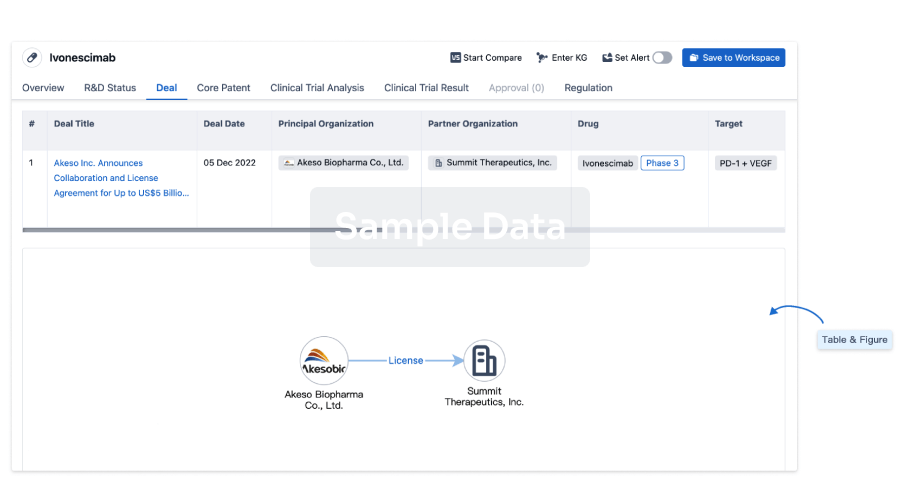
Deal
Boost your decision using our deal data.
login
or
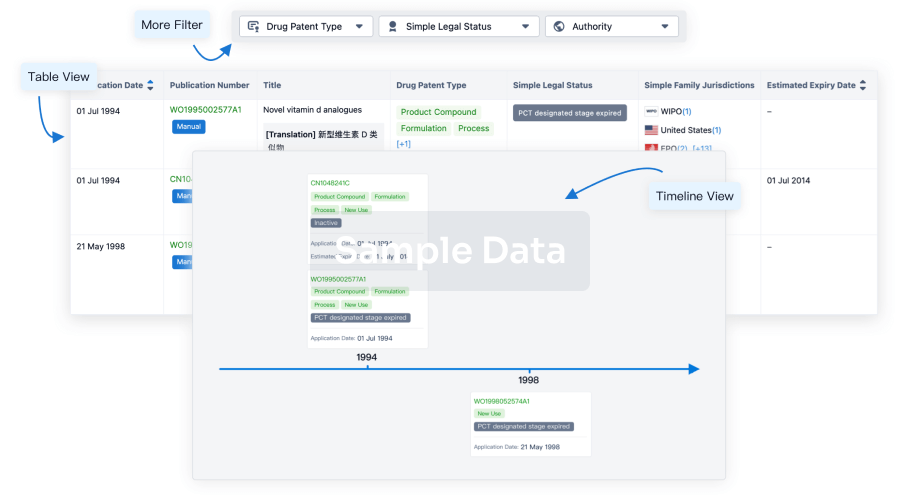
Core Patent
Boost your research with our Core Patent data.
login
or
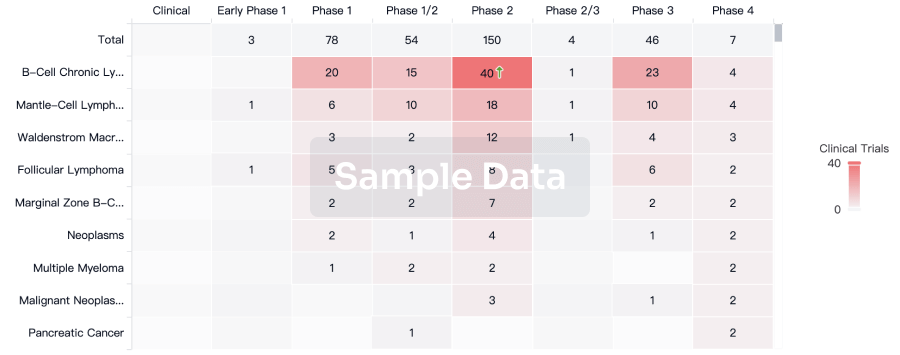
Clinical Trial
Identify the latest clinical trials across global registries.
login
or
Approval
Accelerate your research with the latest regulatory approval information.
login
or
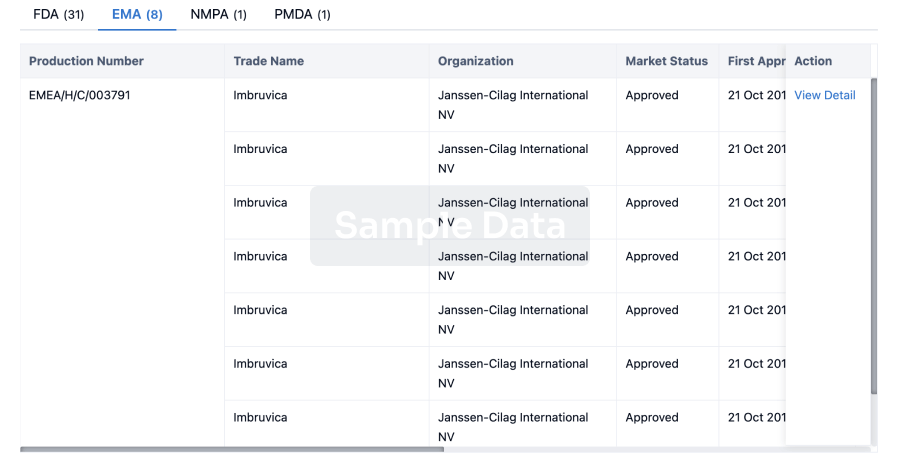
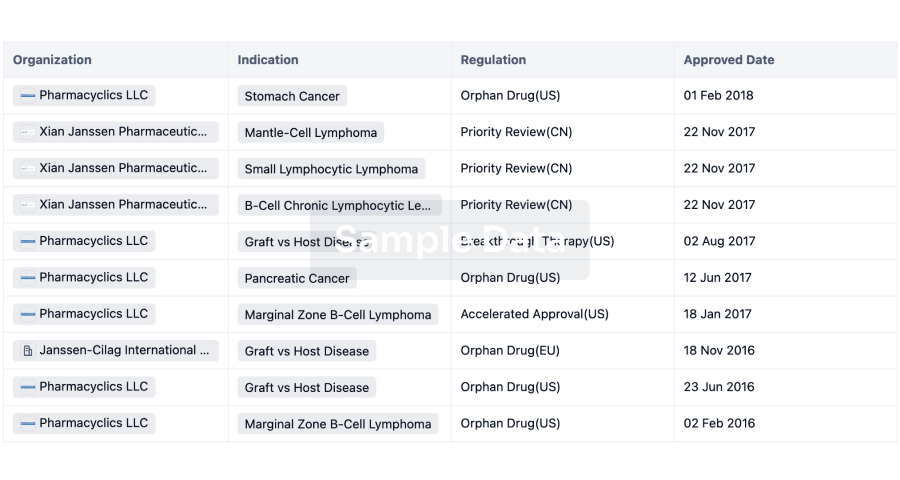
Regulation
Understand key drug designations in just a few clicks with Synapse.
login
or
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free