Request Demo
Last update 21 Mar 2026
SAR-441255
Last update 21 Mar 2026
Overview
Basic Info
Drug Type Synthetic peptide |
Synonyms SAR 441255, SAR441255 |
Target |
Action agonists |
Mechanism GCGR agonists(Glucagon receptor agonists), GIPR agonists(Gastric inhibitory polypeptide receptor agonists), GLP-1R agonists(Glucagon-like peptide 1 receptor agonists) |
Therapeutic Areas |
Active Indication- |
Inactive Indication |
Login to view timeline
Structure/Sequence
Sequence Code 1322846633
Related
1
Clinical Trials associated with SAR-441255NCT04521738
A Randomized, Double-blind, Placebo-controlled Study to Assess the Safety, Tolerability, Pharmacokinetics and Pharmacodynamics of Single Ascending Subcutaneous Doses of SAR441255 in Lean to Overweight Adult Subjects
100 Clinical Results associated with SAR-441255
Login to view more data
100 Translational Medicine associated with SAR-441255
Login to view more data
100 Patents (Medical) associated with SAR-441255
Login to view more data
6
Literatures (Medical) associated with SAR-44125501 Dec 2025EBioMedicine
Positron emission tomography to assess drug occupancy at peripheral and central incretin receptors
Article
Author: Velikyan, Irina ; Khalil, Amina ; Eriksson, Olof ; Wagner, Michael ; Bossart, Martin ; Xiong, Mengfei
BACKGROUND:
Incretin mimetics, especially dual/triple agonists, are effective for type 2 diabetes and obesity, though mechanisms remain unclear. This study applied PET using [68Ga]Ga-DO3A-Exendin-4 and [68Ga]S02-GIP-T4 to assess GLP-1R and GIPR occupancy of SAR441255 (a GLP-1R, GIPR, and GCGR agonist) and tirzepatide in pig pancreas and CNS.
METHODS:
In vitro binding assays on frozen HEK293 cell sections overexpressing human GLP-1R, GIPR, or GCGR assessed [68Ga]Ga-DO3A-Exendin-4 specificity and competition with tirzepatide and SAR441255, and [68Ga]S02-GIP-T4 with SAR441255. In vivo, the GLP-1R occupancy by SAR441255 and tirzepatide, and GIPR occupancy by SAR441255, was evaluated in healthy pigs using PET/CT initiated at tracer injection. A subcutaneous dose of the study drug was then administered, and a second scan was performed 2.5 h later. Occupancy was determined by comparing pancreatic and CNS tracer SUV before and after dosing. Two animals were used to compare the tracers directly.
FINDINGS:
[68Ga]Ga-DO3A-Exendin-4 and [68Ga]S02-GIP-T4 showed high specificity for GLP-1R and GIPR, respectively, and competed with the study drugs in vitro. In vivo, SAR441255 induced dose-dependent GLP-1R occupancy (>70%) in pancreas and pituitary and (>60%) in CNS, while tirzepatide showed lower occupancy. SAR441255 also reduced pancreatic [68Ga]S02-GIP-T4 uptake by 23 ± 8.5%, indicating GIPR engagement.
INTERPRETATION:
PET imaging in pigs demonstrated in vivo GLP-1R engagement by SAR441255 and tirzepatide, and GIPR engagement by SAR441255 in the pancreas. SAR441255 exhibited dose-dependent GLP-1R occupancy in the pancreas and brain regions linked to appetite regulation.
FUNDING:
The study was funded by Uppsala Diabetes Center, Diabetesfonden, ExoDiab, Diabetes Wellness Sweden, Barndiabetesfonden, Science for Life Laboratory, and the Swedish Research Council.
01 Jul 2023Journal of diabetes
A diabetes update
Author: Bloomgarden, Zachary
Understanding of diabetes and its treatment is ever-increasing. We summarize a variety of relevant studies – all potentially suggesting new approaches to the treatment of our patients. Interrelationships between obesity and type 2 diabetes are the focus of a recent review, elegantly summarizing the effects of obesity-related increase in diacyl glycerol and fatty acids on adipose tissue, on the liver, on skeletal muscle, and on the beta cell, with resistance to insulin action, abnormal vagal tone, and, perhaps, the gut microbiome as central players.1 In addition to obesity being associated both with diabetes and with cardiovascular disease (CVD), body weight variability is associated with development of diabetes, particularly among people with diabetes both with microvascular disease outcomes and, as shown in a recent review, with CVD outcomes. Such studies suggest that we should focus both on measures to reduce weight and to stabilize weight among people with diabetes, with glucagon-like peptide (GLP)-1 receptor activators and related medications offering a dual approach to both weight loss and weight stabilization.2 A review by Tschöp and colleagues of the various gut hormone combinations with potential for metabolic disease therapy illustrates current approaches with GLP-1 plus glucose-dependent insulinotropic polypeptide (GIP) receptor dual agonists such as tirzepatide (with high homology to exenatide), GLP-1 plus glucagon receptor dual agonists such as cotadutide and SAR425899 and GLP-1, GIP, and glucagon receptor triple agonists SAR441255 and LY3437943. In addition, GLP-1 or glucagon receptor agonists have been linked to hormones acting at nuclear receptors for estrogen, thyroid hormone, and glucocorticoids, with intriguing evidence of potentiation of weight loss, and L-cell secretagogues are being explored in combination with dipeptidyl peptidase-4 inhibitors.3 An interesting post hoc study of 5378 participants with type 2 diabetes in phase 3 trials of tirzepatide analyzed the relationship found "modest (correlation coefficients 0.1438-0.3130) association between HbA1c reduction and the effect on body weight,"4 suggesting that the two effects are at least partially independent. A study of the GLP-1/GIP receptor activator tirzepatide administration in comparison to placebo in 2539 nondiabetic persons with obesity (mean body mass index 38) showed weight loss of 15%, 20%, and 21% versus 3% with 5 mg, 10 mg, and 15 mg weekly vs placebo, with the expected greater likelihoods of nausea, diarrhea, constipation, and dyspepsia, as well as alopecia in 5%–6% vs 1% with placebo, dizziness in 4%–6% vs 2% with placebo, severe depression in 0.3% versus none, gallbladder disease in 1%–2% vs 1%, hypoglycemia (glucose<54 mg/dL) in 1.5% vs none, cholecystitis in ~0.5% vs none, and pancreatitis in 0.2% of the treated vs placebo groups.5 An oral small molecule GLP-1RA, danuglipron, was compared with placebo in 411 persons with type 2 diabetes, leading at the highest dose to placebo-adjusted reduction in HbA1c by 1.16%, in fasting glucose by 33 mg/dL, and in body weight by 4.17 kg among completers, although with gastrointestinal symptoms of nausea and diarrhea, and with 14% of the participants withdrawing because of adverse events.6 A meta-analysis of nine trials of 11 005 people with type 2 diabetes randomized to intensive blood pressure (BP) control (mean 125/73) vs conventional treatment (mean 134/79) showed 36% reduction in stroke and 32% reduction in progression to macroalbuminuria, although CVD and all-cause mortality rates were similar at the two BP levels7; a similar meta-analysis of six open-label randomized controlled trials including 20 985 patients both having and not having diabetes showed reduction in CVD mortality and congestive heart failure as well as stroke.8 Studies of this sort imply that a BP target of <140/90 is insufficient for persons with diabetes having CVD; CVD risk factors; or Stage 3, 4, or 5 chronic kidney disease, for whom BP should be <130/80.9 Implementing such a target, however, must be tempered by the recognition that in-office BP readings show high visit-to-visit variability and, as such, may not be appropriate in guiding management, leaving us with the dilemma of not having a practical gold standard to use in this crucial aspect of CVD management.10 Once-weekly insulin icodec was compared with once-daily insulin glargine U100 with 2–4 daily bolus insulin aspart injections in 582 persons with type 2 diabetes treated for 26 weeks, finding similar 1.2% reductions in HbA1c from 8.3% baseline, 32 vs 29 mg/dL reduction in fasting glucose, 2.7 vs 2.2 kg increases in body weight, and similar 37% vs 45% rates of level 1 hypoglycemia and 19% vs 25% rates of level 2 or 3 hypoglycemia.11 Reports of insulin icodec in type 1 diabetes12 and in insulin-naïve type 2 diabetes13 also show improvement in glycemia similar to that with once daily insulin degludec, suggesting that it may soon be possible to use once weekly gut hormone-based treatment and once weekly insulin, an approach likely to greatly improve the acceptability of such approaches to our patients. It has been suggested that carbohydrate-counting methods to estimate prandial insulin requirements for people with type 1 diabetes might not be necessary and that simplified qualitative meal-size estimation might offer an easier approach to deciding on appropriate meal insulin doses.14 A study of 30 persons with type 1 diabetes using a closed-loop insulin pump, however, compared two 3-week periods and showed that when the participants crossed over between the two approaches their "time in range" of 70–180 mg/dL was 74.1% with carbohydrate counting, significantly greater than 70.5% with the qualitative method.14 Fenofibrate may have benefit in diabetic retinopathy,15, 16 with a postulated mechanism involving blockade of hypoxia-inducible factor (HIF)-1.17 HIF-1 acts in part by stimulating vascular endothelial growth factor (VEGF) release. In a recent report, a novel small molecule HIF inhibitor was shown to potently inhibit HIF-regulated expression of VEGF and other vasoactive mediators thought to be involved in retinopathy pathogenesis, offering a new potential approach to retinopathy treatment.18 This may particularly be important in view of questions recently raised by a study suggesting that anti-VEGF treatment of >14 000 persons with diabetic retinopathy was associated with increase in likelihood of myocardial infarction or overall cardiovascular disease,19 although the association may be confounded by the relationship between CVD and more severe degrees of retinopathy.20 None. None.
01 Dec 2022Journal of diabetes investigation
Potential of a glucagon‐like peptide‐1 receptor /glucose‐dependent insulinotropic polypeptide receptor/glucagon receptor triagonist for the treatment of obesity and type 2 diabetes
Article
Author: Kazuki Fukuda ; Eiichi Araki ; Tatsuya Kondo ; Masaji Sakaguchi
Triagonists of GLP-1R/ GIPR /GCGR, including SAR441255, bind to each receptor and induce specific effects through each receptor signaling pathway, thus result in weight loss and glycemic control in obese T2D animal models.
100 Deals associated with SAR-441255
Login to view more data
R&D Status
10 top R&D records. to view more data
Login
| Indication | Highest Phase | Country/Location | Organization | Date |
|---|---|---|---|---|
| Overweight | Phase 1 | United States | 25 Apr 2019 |
Login to view more data
Clinical Result
Clinical Result
Indication
Phase
Evaluation
View All Results
Login to view more data
Translational Medicine
Boost your research with our translational medicine data.
login
or

Deal
Boost your decision using our deal data.
login
or

Core Patent
Boost your research with our Core Patent data.
login
or

Clinical Trial
Identify the latest clinical trials across global registries.
login
or

Approval
Accelerate your research with the latest regulatory approval information.
login
or

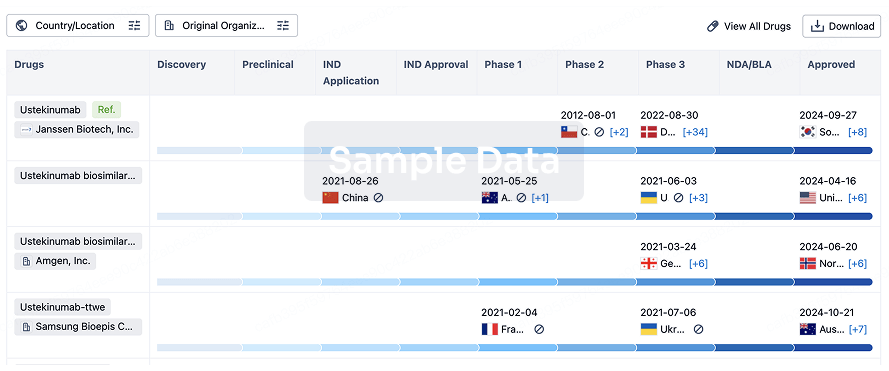
Biosimilar
Competitive landscape of biosimilars in different countries/locations. Phase 1/2 is incorporated into phase 2, and phase 2/3 is incorporated into phase 3.
login
or
Regulation
Understand key drug designations in just a few clicks with Synapse.
login
or

AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free