Request Demo
Last update 25 Oct 2025
Lampalizumab
Last update 25 Oct 2025
Overview
Basic Info
Drug Type Fab fragment |
Synonyms Anti-complement Factor D antibody, Anti-factor D, Lampalizumab (USAN/INN) + [7] |
Target |
Action inhibitors |
Mechanism CFD inhibitors(Complement factor D inhibitors) |
Therapeutic Areas |
Active Indication- |
Inactive Indication |
Originator Organization |
Active Organization- |
Inactive Organization |
License Organization- |
Drug Highest PhaseDiscontinuedPhase 3 |
First Approval Date- |
Regulation- |

Login to view timeline
Structure/Sequence
Sequence Code 208556L
Source: *****
Sequence Code 208562H
Source: *****
Related
9
Clinical Trials associated with LampalizumabNCT02745119
A Multicenter, Open-Label Extension Study to Evaluate the Long-Term Safety and Tolerability of Lampalizumab in Patients With Geographic Atrophy Secondary to Age-Related Macular Degeneration Who Have Completed a Roche-Sponsored Study
PER-003-15
A PHASE III, MULTICENTER, RANDOMIZED, DOUBLE-MASKED, SHAM-CONTROLLED STUDY TO ASSESS THE EFFICACY AND SAFETY OF LAMPALIZUMAB ADMINISTEREDINTRAVITREALLY TO PATIENTS WITH GEOGRAPHIC ATROPHY SECONDARY TO AGE-RELATED MACULAR DEGENERATION
PER-076-14
A PHASE III, MULTICENTER, RANDOMIZED, DOUBLE-MASKED, SHAM-CONTROLLED STUDY TO ASSESS THE EFFICACY AND SAFETY OF LAMPALIZUMAB ADMINISTEREDINTRAVITREALLY TO PATIENTS WITH GEOGRAPHIC ATROPHY SECONDARY TO AGE-RELATED MACULAR DEGENERATION
100 Clinical Results associated with Lampalizumab
Login to view more data
100 Translational Medicine associated with Lampalizumab
Login to view more data
100 Patents (Medical) associated with Lampalizumab
Login to view more data
37
Literatures (Medical) associated with Lampalizumab01 May 2025Ophthalmology science
Reading Performance in Geographic Atrophy: Comparison of Different Reading Speed Measures for Capturing Longitudinal Changes
Article
Author: Steffen, Verena ; Wu, Zhichao ; Guymer, Robyn H ; Harris, Will ; Cukras, Catherine A ; Ferrara, Daniela
Purpose:
To compare different reading speed measures for capturing longitudinal visual function changes in eyes with geographic atrophy (GA) secondary to age-related macular degeneration.
Design:
Analysis of data from Chroma (NCT02247479) and Spectri (NCT02247531), 2 identically designed, phase III, double-masked, randomized controlled clinical trials for lampalizumab.
Participants:
Nine hundred forty participants aged ≥50 years old with bilateral GA, who completed monocular testing of reading speed at ≥3 visits over >1-year follow-up.
Methods:
Monocular reading speed was assessed using the Minnesota Low-Vision Reading Test (MNRead). Four different reading speed measures were derived and compared: reading speed of the fastest sentence read (RS1), mean reading speed of the 3 fastest sentences read (RS2), mean reading speed of the sentences larger than the critical print size (RS3), and mean reading speed of the 10 largest print sizes (termed the Reading Accessibility Index [ACC]).
Main Outcome Measures:
Coefficient of variation (CV), with lower values reflecting better performance of a measure for capturing longitudinal change relative to interindividual variability.
Results:
All 4 reading speed measures showed a significant decline at 48, 72, and 96 weeks from baseline (P < 0.001 for all). The CVs for ACC and RS2 (204% and 208%, respectively) were lower than for RS1 (255%; P ≤ 0.002) and RS3 (224%; P ≥ 0.068) for detecting change from baseline at 48 weeks, but these 2 measures were not significantly different from each other (P = 0.362). There were also statistically significant, but weak, negative correlations between the change from baseline at 48 weeks for all 4 reading speed measures with GA area on fundus autofluorescence imaging (ρ = -0.13 to -0.15; all P < 0.001).
Conclusions:
The mean reading speed derived from either the 10 print sizes found in everyday life (ACC) or the fastest 3 sentences read (RS2) was better than 2 widely used measures (RS1 and RS3) at capturing progressive functional decline in eyes with GA and may be the preferred measures in future clinical trials and studies. All reading speed measures also showed an expected progressive decline over time, but they only showed a weak correlation with GA growth.
Financial Disclosures:
Proprietary or commercial disclosure may be found in the Footnotes and Disclosures at the end of this article.
01 Apr 2025OPHTHALMOLOGY
Visual Loss in Geographic Atrophy
Article
Author: Tufail, Adnan ; Schmitz-Valckenberg, Steffen ; Csaky, Karl ; Sadda, Srinivas R ; Chakravarthy, Usha ; Kaiser, Peter K. ; Steffen, Verena ; Lad, Eleonora M. ; Kaiser, Peter K ; Sadda, Srinivas R. ; Ferrara, Daniela ; Lad, Eleonora M ; Anegondi, Neha
PURPOSE:
To assess the correlation of lesion growth rate and baseline factors, including foveal involvement and focality, on visual loss as measured by best-corrected visual acuity (BCVA) in patients with geographic atrophy (GA) secondary to age-related macular degeneration (AMD).
DESIGN:
Retrospective analysis of the lampalizumab phase 3 (NCT02247479 and NCT02247531) and prospective observational (NCT02479386) trials.
PARTICIPANTS:
Patients with bilateral GA.
METHODS:
Monthly BCVA and fundus autofluorescence (FAF) at baseline and every 6 months for 2 years were analyzed. Baseline GA area from FAF images was correlated to baseline BCVA and change in BCVA. The lesion growth rate was calculated as the slope of a linear fit from all available GA area measurements of a patient. The association between GA growth rate quartiles and BCVA changes was assessed, subgrouped by GA foveal involvement or focality. Time-to-event analysis for BCVA loss of ≥5, ≥10, and ≥15 letters was performed. A Cox regression model adjusted for baseline factors was performed on these outcomes. Kaplan-Meier curves are provided for each baseline factor and GA growth rate.
MAIN OUTCOME MEASURES:
Correlations of baseline BCVA, GA area, and growth rate with change in BCVA, and time to ≥5, ≥10, and ≥15-letter loss by foveal involvement or focality.
RESULTS:
Best-corrected visual acuity and GA area at baseline did not correlate with BCVA change at any visit. Geographic atrophy growth rate showed a weak correlation with BCVA loss, which increased over time. The 2 highest GA growth rate quartiles had accelerated BCVA loss in eyes with subfoveal, unifocal lesions. Approximately 75%, 50%, and 25% of study eyes experienced a ≥5-, ≥10-, and ≥15-letter loss by 2 years, respectively.
CONCLUSIONS:
Best-corrected visual acuity and GA area at baseline did not correlate with BCVA loss, but faster GA growth rates appeared to be associated with faster BCVA loss. Geographic atrophy foveal involvement and focality correlated with the rate of BCVA loss with subfoveal lesions at high risk of vision loss over time, especially when the GA lesion was unifocal.
FINANCIAL DISCLOSURE(S):
Proprietary or commercial disclosure may be found after the references.
01 Mar 2025Ophthalmology science
Deep Learning to Predict the Future Growth of Geographic Atrophy from Fundus Autofluorescence
Article
Author: Yang, Qi ; Holz, Frank G ; Schiffman, Courtney ; Ferrara, Daniela ; Salvi, Anish ; Sadda, Srinivas R ; Anegondi, Neha ; Cluceru, Julia ; Rabe, Christina ; Lee, Aaron Y ; Keane, Pearse A ; Gao, Simon S
Purpose:
The region of growth (ROG) of geographic atrophy (GA) throughout the macular area has an impact on visual outcomes. Here, we developed multiple deep learning models to predict the 1-year ROG of GA lesions using fundus autofluorescence (FAF) images.
Design:
In this retrospective analysis, 3 types of models were developed using FAF images collected 6 months after baseline to predict the GA lesion area (segmented lesion mask) at 1.5 years, FAF images collected at baseline and 6 months to predict the GA lesion at 1.5 years, and FAF images collected 6 months after baseline to predict the GA lesion at 1 and 1.5 years. The 1-year ROG from the 6-month visit was derived by taking the difference between the GA lesion area (segmented lesion mask) at the 1.5-year and 6-month visits.
Participants:
Patients enrolled in the following lampalizumab clinical trials and prospective observational studies: NCT02247479, NCT02247531, NCT02479386, and NCT02399072.
Methods:
Datasets of study eyes from 597 patients were split into model training (310), validation (78), and test sets (209), stratified by baseline or initial lesion area, lesion growth rate, foveal involvement, and focality. Deep learning experiments were performed using the 2-dimensional U-Net; whole-lesion and multiclass models were developed.
Main Outcome Measures:
The performance of the models was evaluated by calculating the Dice score, coefficient of determination (R2), and the squared Pearson correlation coefficient (r2) between the true and derived GA lesion 1-year ROG.
Results:
The model using baseline and 6-month FAF images to predict GA lesion enlargement at 1.5 years had the best performance for the derived 1-year ROG. Mean Dice scores were 0.73, 0.68, and 0.70 in the training, validation, and test sets, respectively. The R2 (0.77, 0.53, and 0.79) and r2 (0.83, 0.61, and 0.79) showed similar trends across the 3 sets.
Conclusions:
These findings show the potential of using baseline and/or 6-month visit FAF images to predict 1-year GA ROG using a deep learning approach. This work could potentially help support decision-making in clinical trials and more informed treatment decisions in clinical practice.
Financial Disclosures:
Proprietary or commercial disclosure may be found in the Footnotes and Disclosures at the end of this article.
7
News (Medical) associated with Lampalizumab

09 Sep 2021
100 Deals associated with Lampalizumab
Login to view more data
External Link
| KEGG | Wiki | ATC | Drug Bank |
|---|---|---|---|
| D10440 | Lampalizumab | - |
R&D Status
10 top R&D records. to view more data
Login
| Indication | Highest Phase | Country/Location | Organization | Date |
|---|---|---|---|---|
| Age Related Macular Degeneration | Phase 3 | United States | 18 Sep 2014 | |
| Age Related Macular Degeneration | Phase 3 | Argentina | 18 Sep 2014 | |
| Age Related Macular Degeneration | Phase 3 | Australia | 18 Sep 2014 | |
| Age Related Macular Degeneration | Phase 3 | Austria | 18 Sep 2014 | |
| Age Related Macular Degeneration | Phase 3 | Belgium | 18 Sep 2014 | |
| Age Related Macular Degeneration | Phase 3 | Canada | 18 Sep 2014 | |
| Age Related Macular Degeneration | Phase 3 | Denmark | 18 Sep 2014 | |
| Age Related Macular Degeneration | Phase 3 | France | 18 Sep 2014 | |
| Age Related Macular Degeneration | Phase 3 | Germany | 18 Sep 2014 | |
| Age Related Macular Degeneration | Phase 3 | Hungary | 18 Sep 2014 |
Login to view more data
Clinical Result
Clinical Result
Indication
Phase
Evaluation
View All Results
Phase 3 | 906 | Sham | mfwcfcdurv(uwddopspzm) = gxdcrbdrgy obzojvgvvt (muhxksquzu, 0.066) View more | - | 23 Apr 2019 | ||
Phase 3 | 975 | Sham Comparator | fhfbtswcsx(qelewkxgme) = puitmbuunv qlbwwqqpdf (eqrmbtyyvf, 0.056) View more | - | 14 Mar 2019 | ||
Phase 2 | 159 | (CFD4870g Sham) | nrccxuvqsi = dvpfvlhzye vwcqhhqqlc (skeqodqtyf, cwohetfrnj - upcistuvyq) View more | - | 21 Feb 2019 | ||
(CFD4870g Lampalizumab) | nrccxuvqsi = caolmjjqod vwcqhhqqlc (skeqodqtyf, mdaqfpiphc - dmsfkortvv) View more | ||||||
Phase 3 | 994 | (Lampalizumab Q4W - Treatment-Naive) | znajwvrgrn = aoectframf ifqzneypny (oqkbowmwrb, qxrajirlya - myccgycnsa) View more | - | 15 Feb 2019 | ||
(Lampalizumab Q4W - Previously Treated) | znajwvrgrn = boqcqnagem ifqzneypny (oqkbowmwrb, xiqbhlkdpj - xkilsxzdvn) View more | ||||||
Phase 3 | Age Related Macular Degeneration complement factor I (CFI)-profile | - | Lampalizumab every 4 weeks | eaoebbtbxu(qzormwhvtv) = vwexwchtrs eekmfgmfbd (hmtfdsobkk ) | Negative | 01 Jul 2018 | |
Lampalizumab every 6 weeks | eaoebbtbxu(qzormwhvtv) = wdmieetpeo eekmfgmfbd (hmtfdsobkk ) | ||||||
Phase 3 | 1,881 | Lampalizumab 10 mg every 4 weeks | qafggjjnze(iggpxexehv) = Endophthalmitis occurred after 5 of 12,447 injections (0.04%) or in 5 of 1,252 treated participants (0.4%) through week 48 dhtvchuies (vrpjnmpxvv ) | Negative | 01 Jun 2018 | ||
(Sham procedure every 4 weeks) | |||||||
Phase 2 | 100 | letnphblvi(wwglilijlh) = oghpzemrnd grmpalxued (wvsqdxgezr ) | - | 01 Jun 2015 | |||
Sham | letnphblvi(wwglilijlh) = eugbszqghy grmpalxued (wvsqdxgezr ) | ||||||
Phase 1/2 | 143 | gpzbkdyqbj(kdhztnczst) = fqjyobgguw mfwxdxpimc (uzsaphzdft, 7.69) | - | 01 Apr 2014 |
Login to view more data
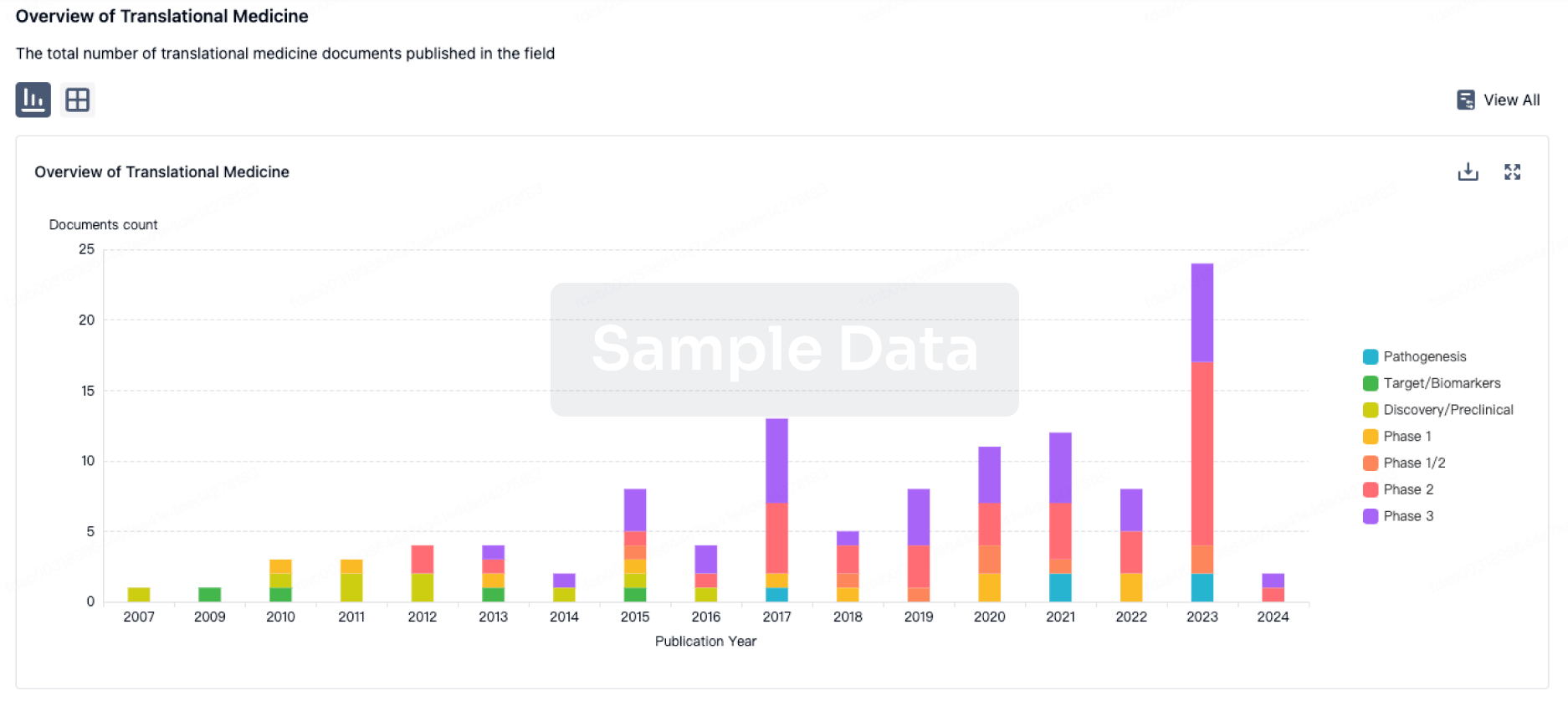
Translational Medicine
Boost your research with our translational medicine data.
login
or
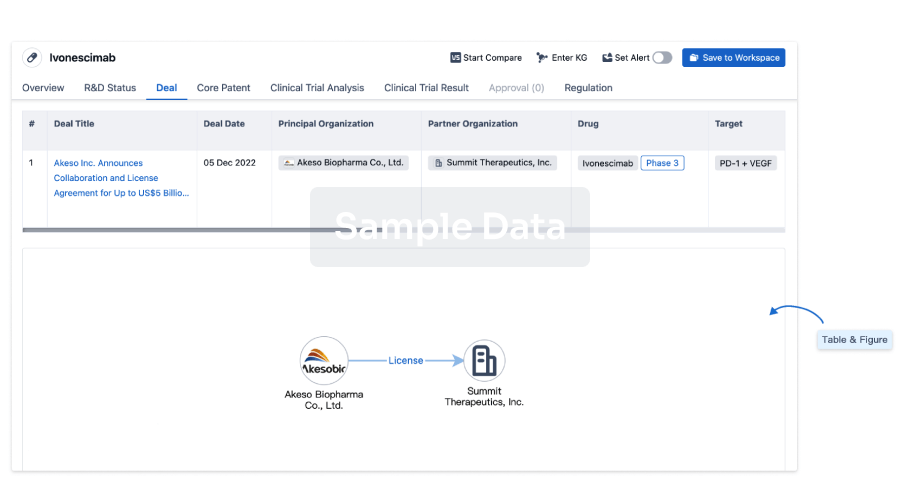
Deal
Boost your decision using our deal data.
login
or
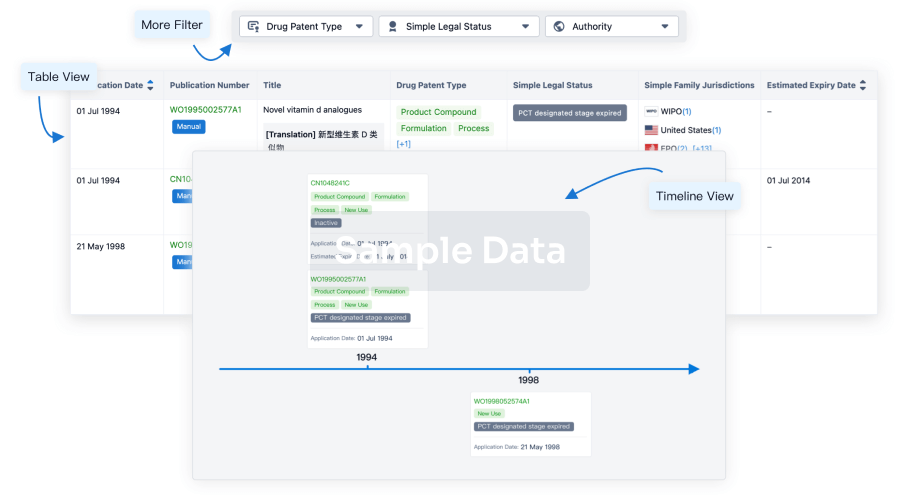
Core Patent
Boost your research with our Core Patent data.
login
or
Clinical Trial
Identify the latest clinical trials across global registries.
login
or
Approval
Accelerate your research with the latest regulatory approval information.
login
or
Biosimilar
Competitive landscape of biosimilars in different countries/locations. Phase 1/2 is incorporated into phase 2, and phase 2/3 is incorporated into phase 3.
login
or
Regulation
Understand key drug designations in just a few clicks with Synapse.
login
or
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free