Request Demo
Last update 23 Jan 2025

Jeroen Bosch Hospital
Last update 23 Jan 2025
Overview
Related
NCT06746246
Prospective Evaluation of Multicenter Implementation of Remote Monitoring of Liver Cirrhosis Patients
NCT06636370
Contrast-enhanced Mammography and Abbreviated MRI as Supplemental Screening Modalities for Women Aged 50-75 With Extremely Dense Breast Tissue: the DENSE-2 Trial
NL-OMON57006
Perioperative Lipofilling in Operative Treatment of Proximal Phalanx Fractures and Related Tenolysis: Improving Range of Motion - Lipofilling in Surgery of Proximal Phalanx Fractures and Related Tenolysis
100 Clinical Results associated with Jeroen Bosch Hospital
Login to view more data
Login to view more data
01 Mar 2025Medical Mycology Case Reports
Pulmonary coccidioidomycosis presenting as a fungal ball mimicking aspergilloma
Article
Author: van der Sloot, C A ; van der Lee, Henrich ; Buil, Jochem B ; van den Biggelaar, Rik ; Couwenbergh, Tristan ; Leenders, Alexander C A P
01 Feb 2025Annals of Surgery
Nationwide Outcome after Pancreatoduodenectomy in Patients at Very High Risk (ISGPS-D) for Postoperative Pancreatic Fistula
Article
Author: Festen, Sebastiaan ; Bonsing, Bert A. ; Bosscha, Koop ; den Dulk, Marcel ; van Santvoort, Hjalmar C. ; van Eijck, Casper H.J. ; Wijsman, Jan H. ; Draaisma, Werner A. ; Suurmeijer, J. Annelie ; de Wilde, Roeland F. ; Stommel, Martijn W.J. ; Meerdink, Mark ; Patijn, Gijs A. ; Groot Koerkamp, Bas ; van Laarhoven, Kees ; van Dam, Ronald ; Busch, Olivier R. ; Stoop, Thomas F. ; Hendriks, Tessa E. ; Smits, F. Jasmijn ; Theijse, Rutger T. ; Lips, Daan J. ; Besselink, Marc G. ; van der Harst, Erwin ; Manusama, Eric ; Molenaar, I. Quintus
01 Feb 2025Surgery
Risk factors and outcomes of conversions in robotic and laparoscopic liver resections: A nationwide analysis
Article
Author: Lips, Daan J ; van Dam, Ronald M. ; de Boer, Marieke T ; Coolsen, Marielle M E ; Sijberden, Jasper P. ; Liem, Mike S L ; Rijken, Arjen M ; Marsman, Hendrik A. ; Verheijen, Paul M ; Sijberden, Jasper P ; Gerhards, Michael F. ; Leclercq, Wouter K G ; Kok, Niels F M ; Derksen, Wouter J.M. ; Nieuwenhuijs, Vincent ; van den Boezem, Peter B. ; Abu Hilal, Mohammad ; Lips, Daan J. ; van Dieren, Susan ; Belt, Eric J.T. ; de Graaff, Michelle R ; Marsman, Hendrik A ; Oosterling, Steven J ; Gerhards, Michael F ; Kok, Niels F.M. ; Tran, T.C. Khé ; Hagendoorn, Jeroen ; Gobardhan, Paul ; Besselink, Marc G. ; Vermaas, Maarten ; Rijken, Arjen M. ; Oosterling, Steven J. ; Patijn, Gijs A. ; de Graaff, Michelle R. ; Derksen, Wouter J M ; Bosscha, Koop ; Torrenga, Hans ; Liem, Mike S.L. ; Swijnenburg, Rutger-Jan ; de Boer, Marieke T. ; van Dam, Ronald M ; Mieog, J Sven D ; Besselink, Marc G ; Verheijen, Paul M. ; Coolsen, Marielle M.E. ; Tran, T C Khé ; van den Boezem, Peter B ; Terkivatan, Türkan ; Leclercq, Wouter K.G. ; Belt, Eric J T ; Pilz da Cunha, Gabriela ; Mieog, J. Sven D. ; Patijn, Gijs A
100 Deals associated with Jeroen Bosch Hospital
Login to view more data
100 Translational Medicine associated with Jeroen Bosch Hospital
Login to view more data
Corporation Tree
Boost your research with our corporation tree data.
login
or
Pipeline
Pipeline Snapshot as of 06 Apr 2025
No data posted
Login to keep update
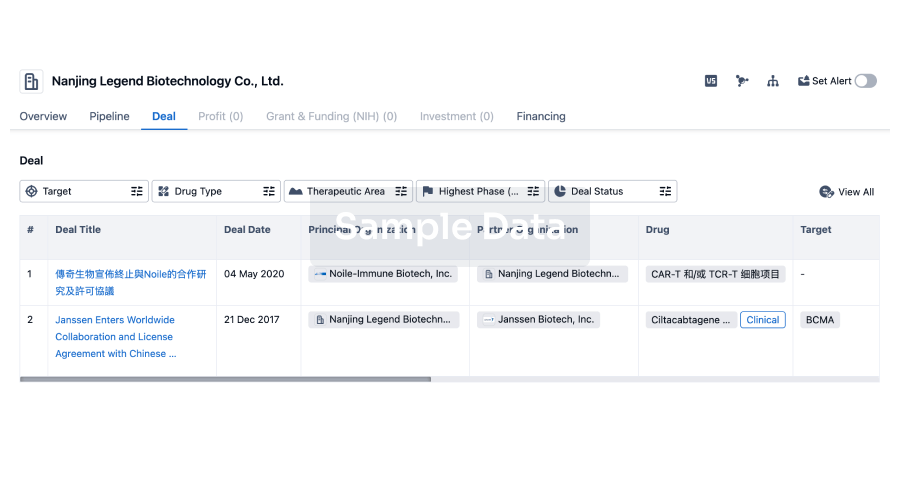
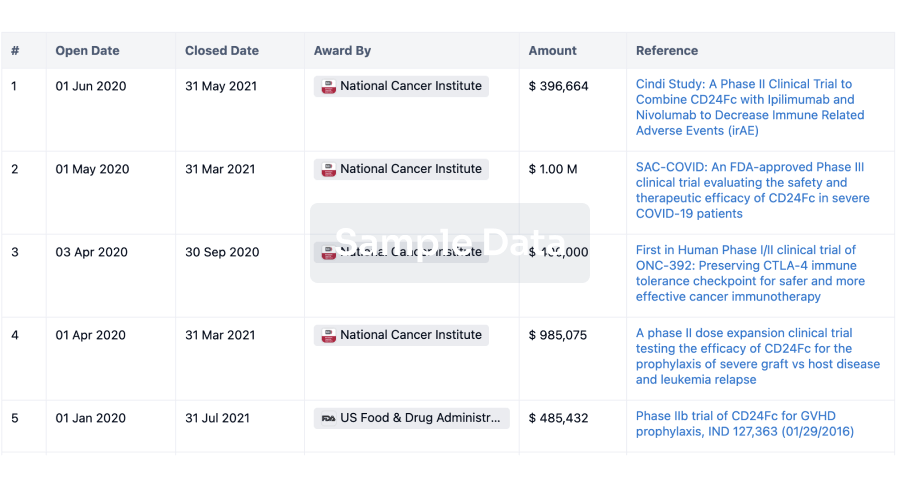
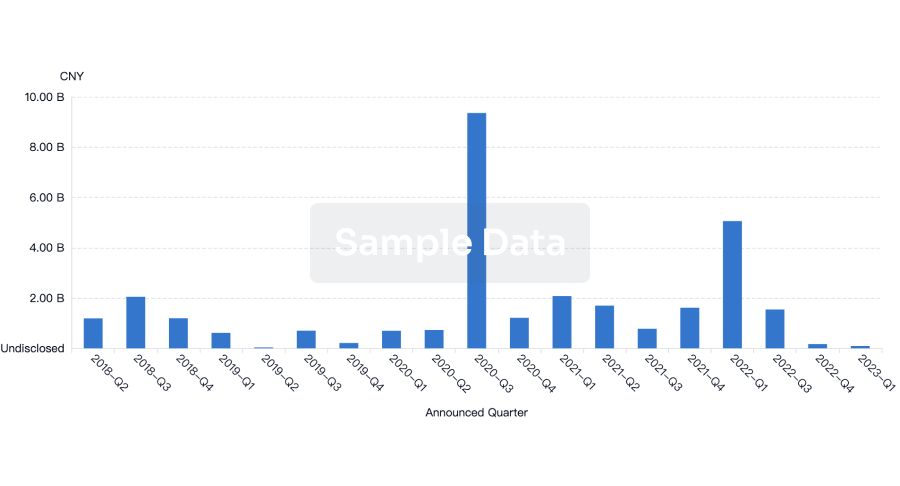
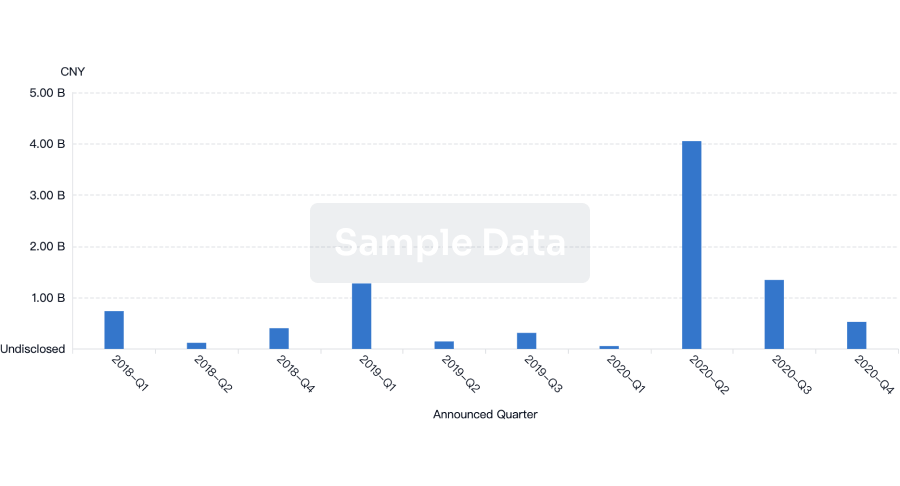
Deal
Boost your decision using our deal data.
login
or
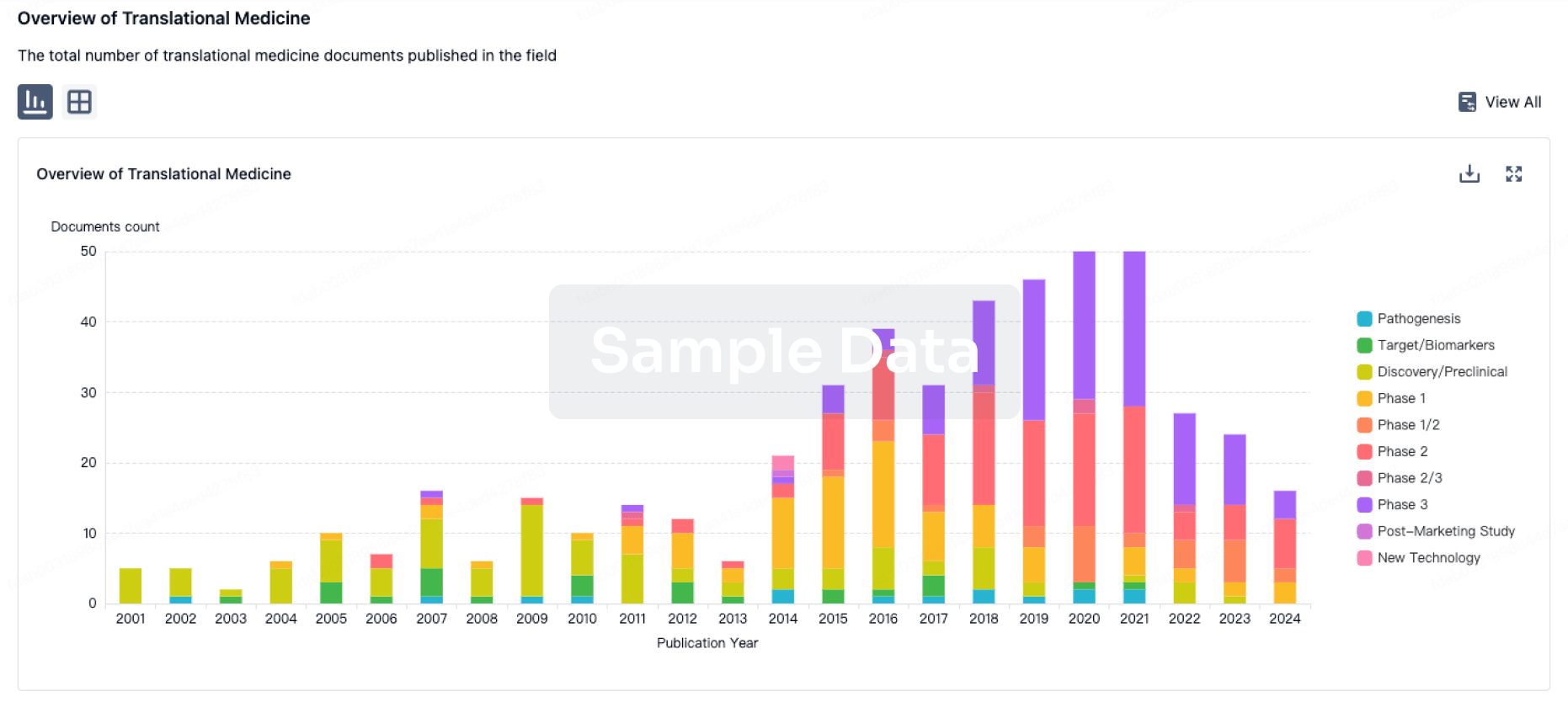
Translational Medicine
Boost your research with our translational medicine data.
login
or
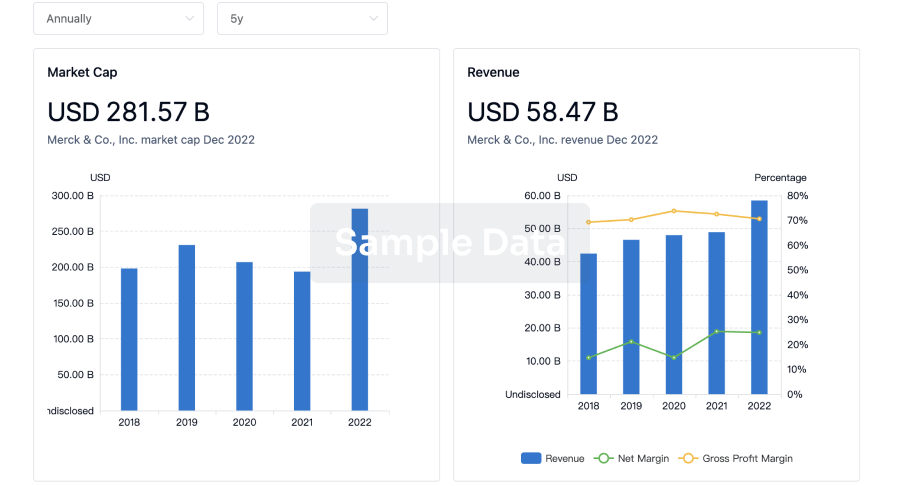
Profit
Explore the financial positions of over 360K organizations with Synapse.
login
or
Grant & Funding(NIH)
Access more than 2 million grant and funding information to elevate your research journey.
login
or
Investment
Gain insights on the latest company investments from start-ups to established corporations.
login
or
Financing
Unearth financing trends to validate and advance investment opportunities.
login
or
Chat with Hiro
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free