Last update 01 Nov 2024
Children's Hospital of Nanjing Medical University
Last update 01 Nov 2024
Overview
Related
Mechanism and efficacy prediction indicators Following Repetitive Transcranial Magnetic Stimulation in Children With ASD:Functional magnetic resonance imaging study
Development of a growth hormone treatment prognostic model for short stature children: a multicenter cohort study of short stature children
Effect of stepwise nonpharmacological intervention for procedural pain on neuropsychological development and physical growth of preterm infants.
100 Clinical Results associated with Children's Hospital of Nanjing Medical University
Login to view more data
Login to view more data
31 Dec 2024Human Vaccines & Immunotherapeutics
The seroepidemiology of immunoglobulin G antibodies against pertussis toxin and filamentous hemagglutinin in the east of China during the COVID-19 pandemic
Article
Author: Sun, Xiang ; Zhou, Juan ; Wu, Yun ; Wang, Wen ; Zhang, Tingting ; Xu, Yan ; Sun, Jinning ; Chen, Qiang ; Jia, Chengmei ; Wang, Zhiguo
01 Dec 2024Colloids and Surfaces B: Biointerfaces
Biomimetic triggered release from hydroxyethyl cellulose @ Prussian blue microparticles for tri-modality biofilm removal
Article
Author: Muhire, Jules ; Xie, Min ; Qu, Qingli ; Zhang, Xiaoli ; Huang, Chaobo ; Pei, Dong ; Xiong, Ranhua ; Yang, Anquan ; Cheng, Weixia
01 Dec 2024Pediatric Cardiology
Perioperative Brain Injury in Children with Aortic Arch Anomalies: A Retrospective Study of Risk Factors and Outcomes
Article
Author: Qi, Jirong ; Ye, Mingtang ; Hu, Liang ; Mo, Xuming ; Peng, Wei ; Chen, Feng ; Wu, Kaihong ; Ding, Peicheng ; Ding, Jie ; Xu, Jiali
100 Deals associated with Children's Hospital of Nanjing Medical University
Login to view more data
100 Translational Medicine associated with Children's Hospital of Nanjing Medical University
Login to view more data
Corporation Tree
Boost your research with our corporation tree data.
login
or
Pipeline
Pipeline Snapshot as of 27 Dec 2024
No data posted
Login to keep update
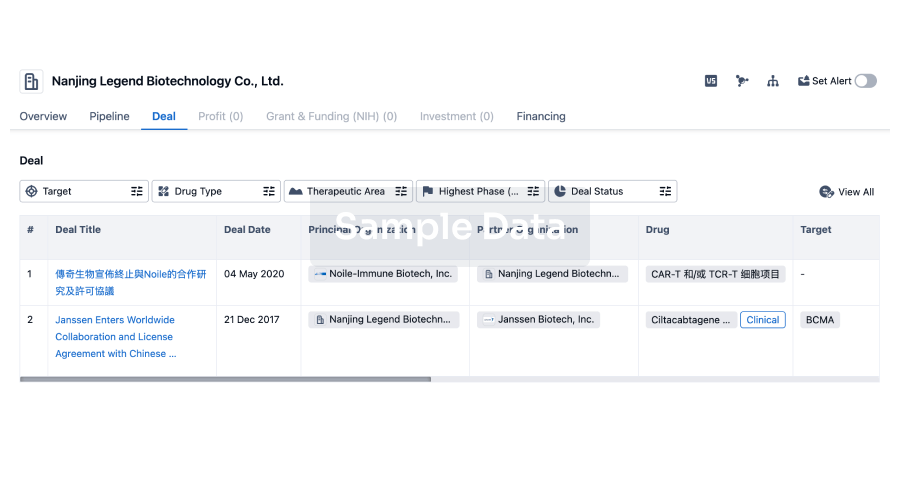
Deal
Boost your decision using our deal data.
login
or
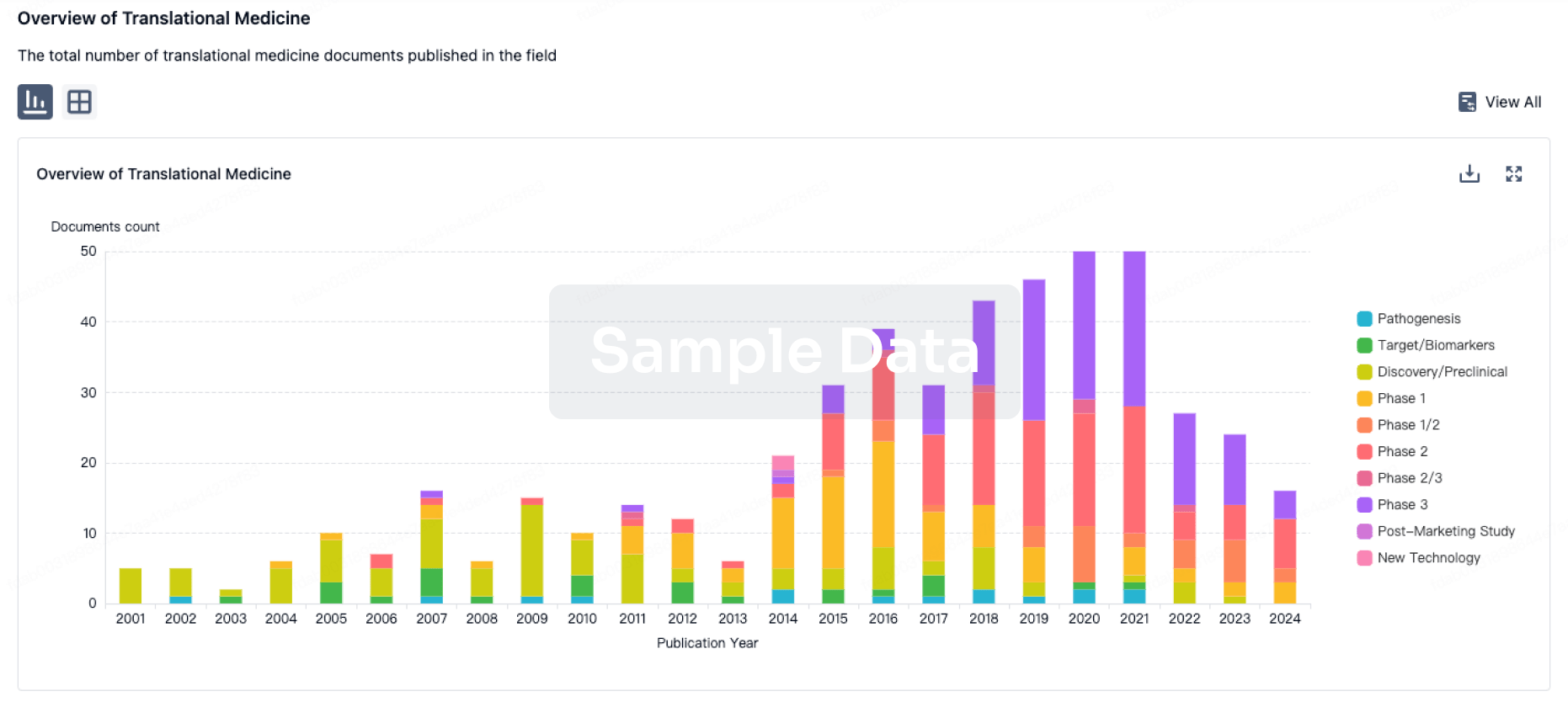
Translational Medicine
Boost your research with our translational medicine data.
login
or
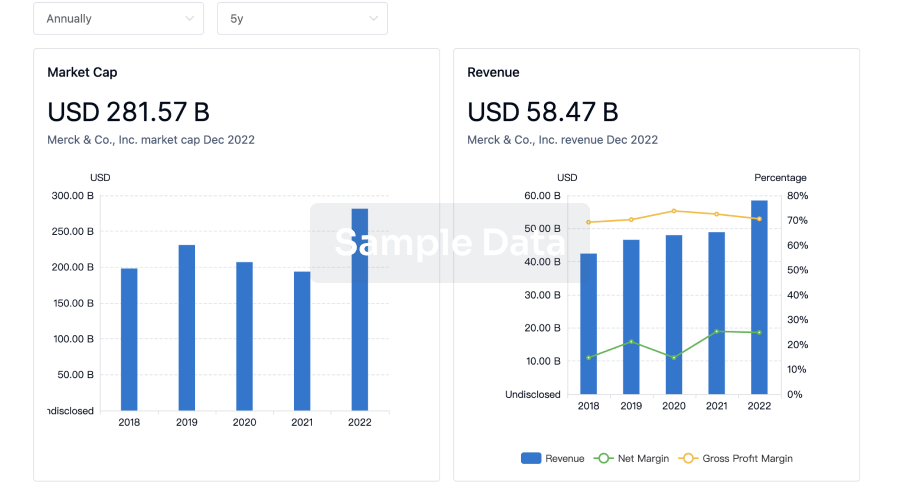
Profit
Explore the financial positions of over 360K organizations with Synapse.
login
or
Grant & Funding(NIH)
Access more than 2 million grant and funding information to elevate your research journey.
login
or
Investment
Gain insights on the latest company investments from start-ups to established corporations.
login
or

Financing
Unearth financing trends to validate and advance investment opportunities.
login
or
Chat with Hiro
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free