Request Demo
Last update 08 May 2025

Texas Scottish Rite Hospital for Children
Last update 08 May 2025
Overview
Related
NCT06559215
Prospective Evaluation of Post-operative Pain Management Using Exparel in the Pediatric Population
NCT06559137
Prospective Evaluation of Post-operative Pain Management Using Peripheral Nerve Blocks in the Pediatric Population
NCT06048419
Acceptability and Efficacy of GO MOVE: A Mobile Health Technology for Youth With Unilateral Cerebral Palsy
100 Clinical Results associated with Texas Scottish Rite Hospital for Children
Login to view more data
Login to view more data
12 May 2025Brain Injury
Endophenotype presentation of athletes with concussion contingent on sex and time since injury
Article
Author: Cullum, C Munro ; Beitchman, Joshua A ; Chung, Jane S ; Stokes, Mathew ; Didehbani, Nyaz ; Miller, Shane M ; Hynan, Linda S ; Jones, Jacob C
01 Mar 2025Spine Deformity
Spine deformity surgery in patients with Beals syndrome can be effectively performed but does risk revision surgery
Article
Author: Datcu, Anne-Marie ; Thornberg, David ; Booth, Anna ; Sucato, Daniel J ; Sucato, Daniel J.
01 Mar 2025Clinical Orthopaedics & Related Research
Clinical Faceoff: The Role of Elective Bilateral Lower Limb Lengthening for Gaining Height
Article
Author: Birch, John ; Sabharwal, Sanjeev ; Paley, Dror
100 Deals associated with Texas Scottish Rite Hospital for Children
Login to view more data
100 Translational Medicine associated with Texas Scottish Rite Hospital for Children
Login to view more data
Corporation Tree
Boost your research with our corporation tree data.
login
or
Pipeline
Pipeline Snapshot as of 12 Jul 2025
No data posted
Login to keep update
Deal
Boost your decision using our deal data.
login
or
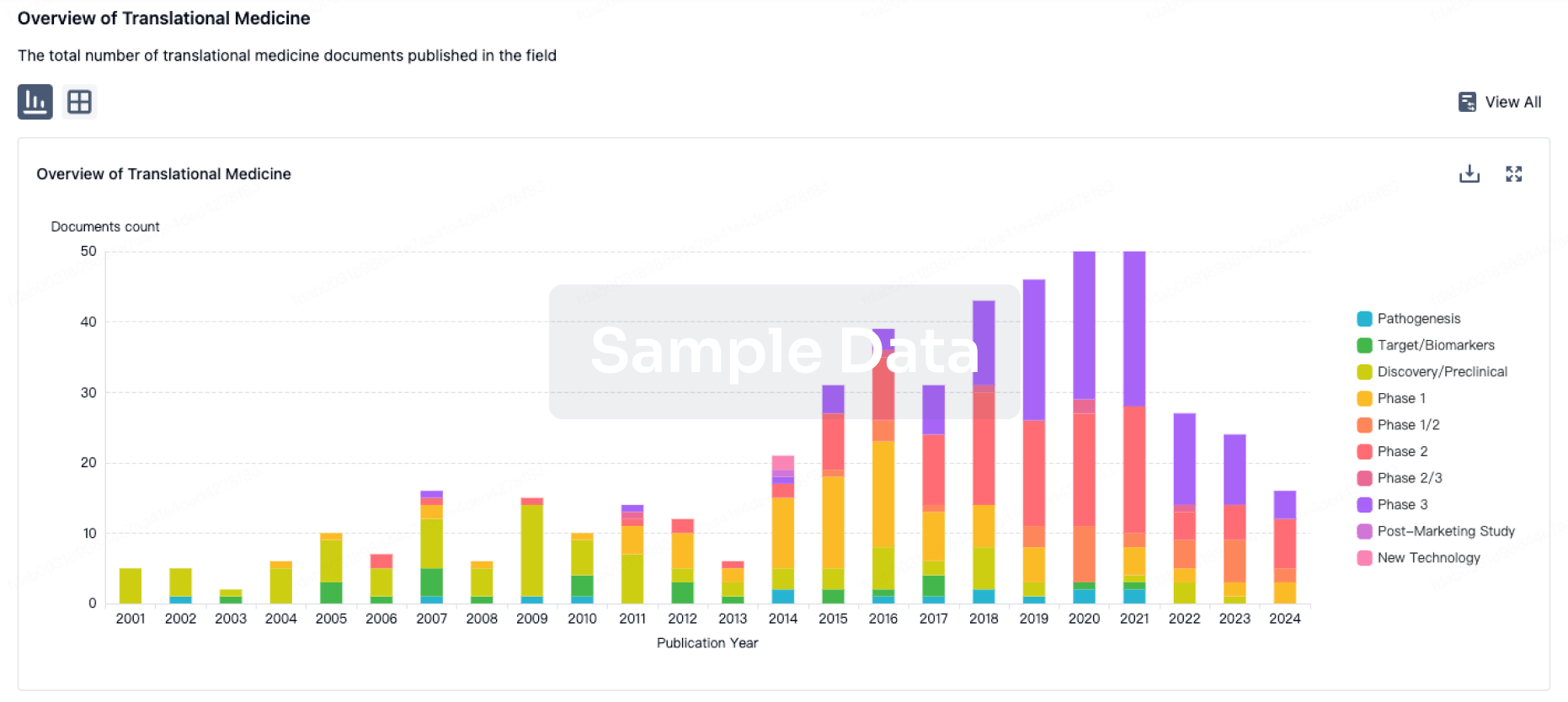
Translational Medicine
Boost your research with our translational medicine data.
login
or
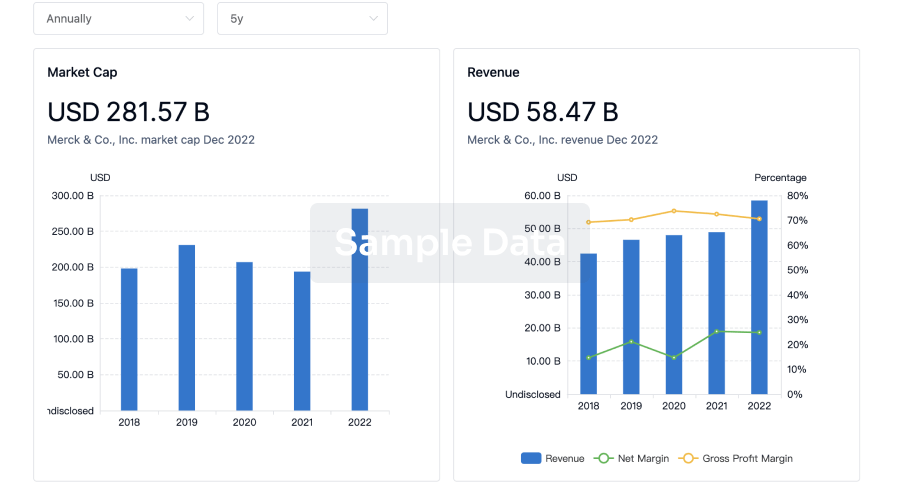
Profit
Explore the financial positions of over 360K organizations with Synapse.
login
or
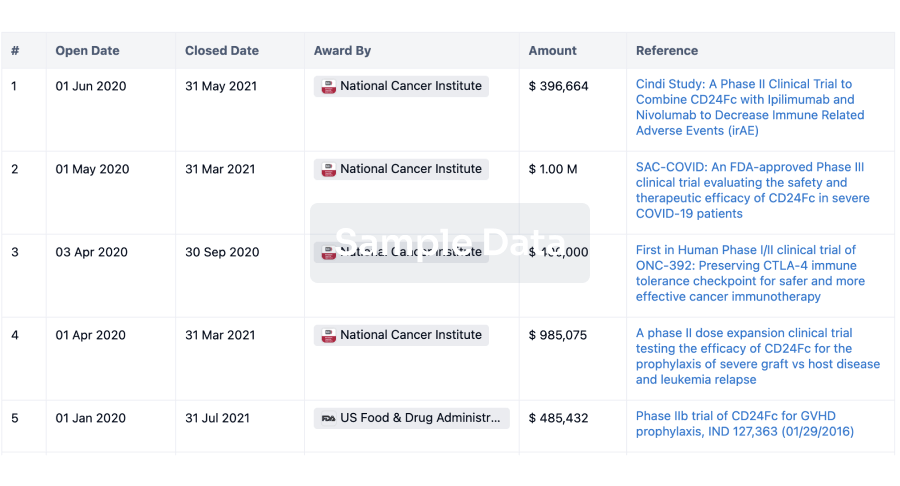
Grant & Funding(NIH)
Access more than 2 million grant and funding information to elevate your research journey.
login
or
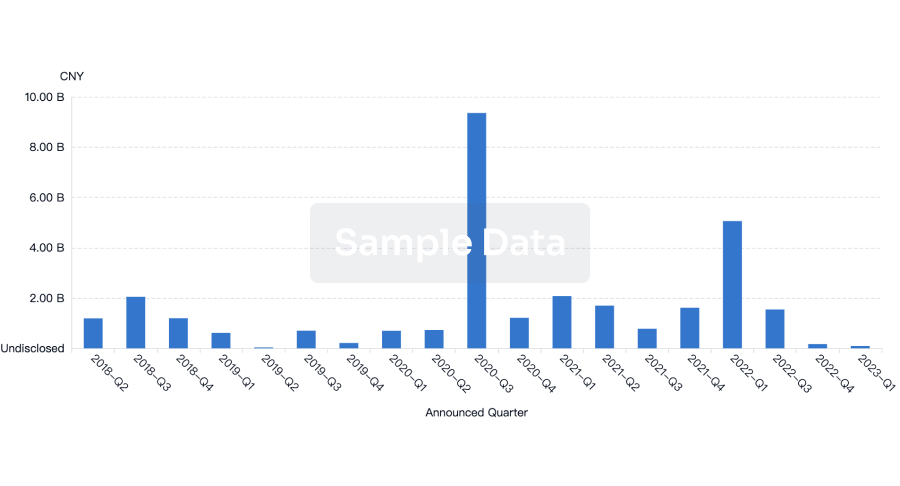
Investment
Gain insights on the latest company investments from start-ups to established corporations.
login
or
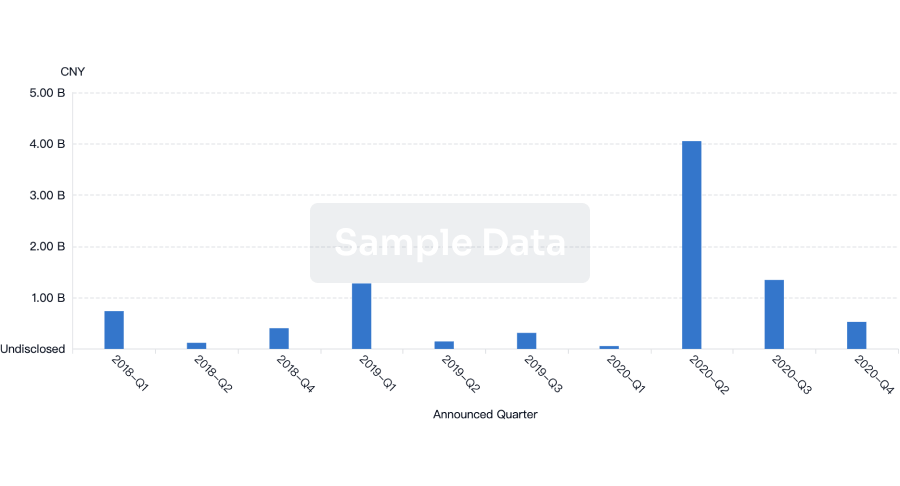
Financing
Unearth financing trends to validate and advance investment opportunities.
login
or
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free