Request Demo
Last update 08 May 2025

Vydehi Institute of Medical Sciences & Research Centre
Last update 08 May 2025
Overview
Related
CTRI/2024/09/074332
Clinical and radiographic evaluation of Poly Glycolic Acid / Poly Lactic Acid and hydroxyapatite paste in the treatment of periodontal intrabony defects:A randomized controlled clinical trial - NIL
CTRI/2024/07/070502
A comparative study between Clonidine and Buprenorphine as adjuvants to 0.5 percent Ropivacaine in Ultrasound guided Infraclavicular Brachial Plexus Block - nil
CTRI/2024/07/069758
To Evaluate The Efficacy Of Intra Operative Infusion Of Lignocaine On Post Operative Pain, Nausea, Vomiting And Recovery In Patients Undergoing Laparoscopic Gynecological Procedures - Nil
100 Clinical Results associated with Vydehi Institute of Medical Sciences & Research Centre
Login to view more data
Login to view more data
21 Apr 2025Cancer Research
Abstract 5807: Differential T cell response to anti-PD1 in breast cancer Sub-types is driven by activity of intra-tumoral immune cells
Author: Pavithira . ; M, Oliyarasi ; Krishnappa, Ravi ; Prabha, Amritha ; Kapur, Méhul ; Malhotra, Ritu ; MS, Ganesh ; BV, Prakash ; Basak, Nandini Pal ; C, Jayaprakash ; S, Saikrishna ; K, Govindaraj ; Nath, Moumita ; M, Rajashekar ; R, Pallavi ; Sankaran, Satish ; Bhowal, Chandan ; T, Venkatesh ; Das, Biswajit ; Malhotra, Mohit ; Haseeb, Abdul ; V, Syamkumar ; M, Dharanidharan ; Jaganathan, Kowshik ; MM, Mouniss ; Chandran, Kubera ; K, Upendra
08 Apr 2025Neurology
Plasma Exchange versus Intravenous Immunoglobulin for the Treatment of Guillain Barre Syndrome. (P4-8.006)
Author: Prasad, Ananya ; prashanth, disha ; Bellur, Vinay Chandramouli ; Rao, Advaith ; Raghunandan, Shruthi ; Gupta, Era ; Aluru, Deepika Reddy ; Prasad, Kushal ; Narayan, Shreya
08 Apr 2025Neurology
Artificial Intelligence (AI) powered P300 and SSVEP based Brain Computer Interfaces (BCI) used in Neurorehabilitation - a Systematic Review and Meta-Analysis (N5.001)
Author: Gupta, Aryan ; Prasad, Ananya ; Bellur, Vinay Chandramouli ; Raghunandan, Shruthi ; Prabhu, Allama ; Gupta, Era ; Rao, Advaith ; Prasad, Kushal ; Rao, Anmol ; Karaveetil, Shradha Chervittara
100 Deals associated with Vydehi Institute of Medical Sciences & Research Centre
Login to view more data
100 Translational Medicine associated with Vydehi Institute of Medical Sciences & Research Centre
Login to view more data
Corporation Tree
Boost your research with our corporation tree data.
login
or
Pipeline
Pipeline Snapshot as of 28 Jun 2025
No data posted
Login to keep update
Deal
Boost your decision using our deal data.
login
or
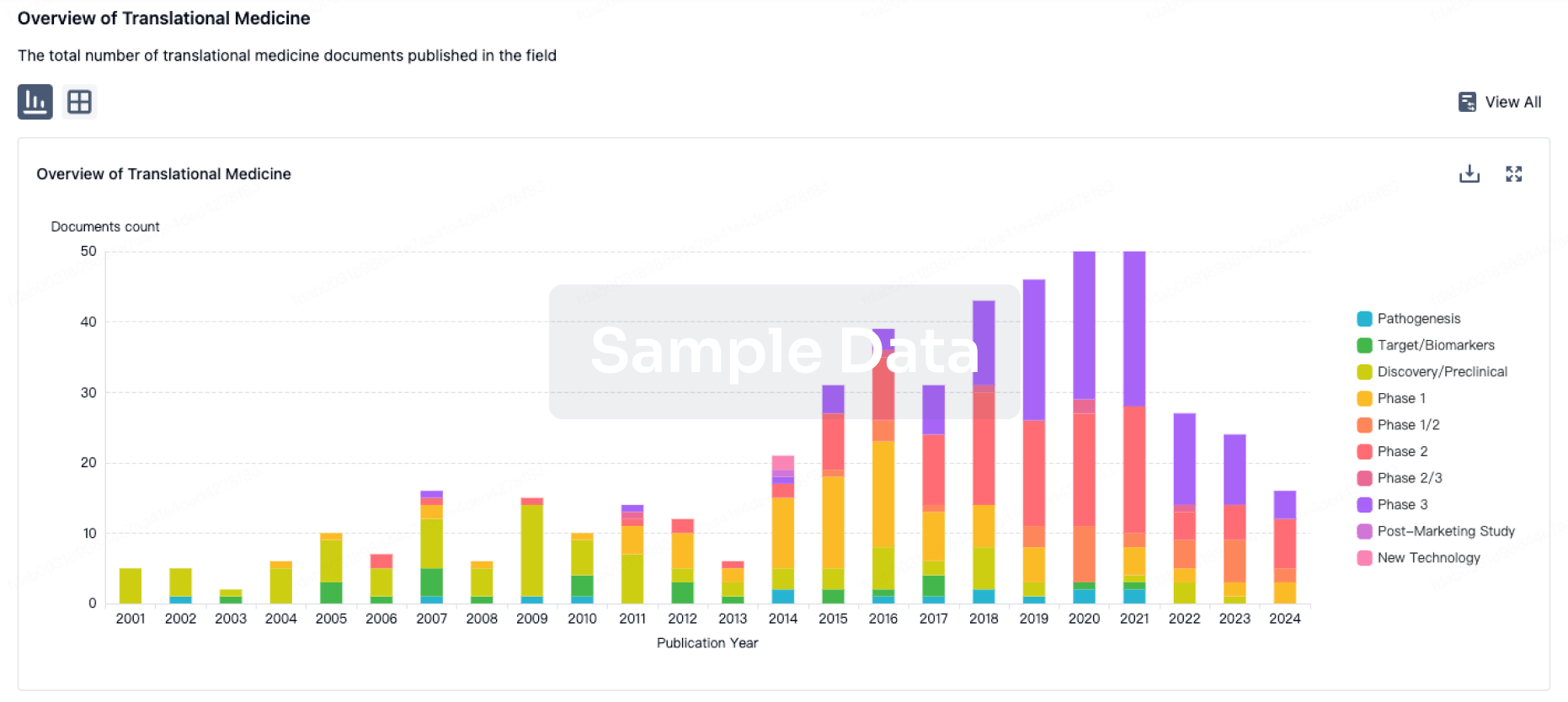
Translational Medicine
Boost your research with our translational medicine data.
login
or
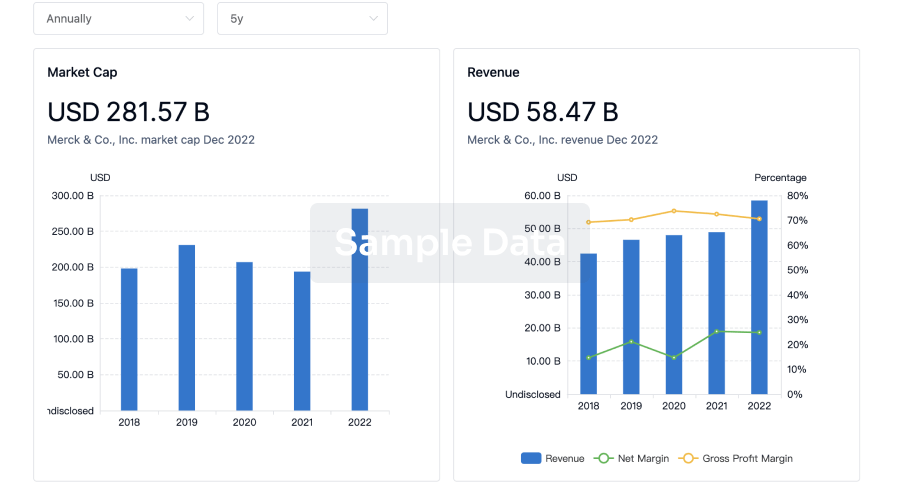
Profit
Explore the financial positions of over 360K organizations with Synapse.
login
or
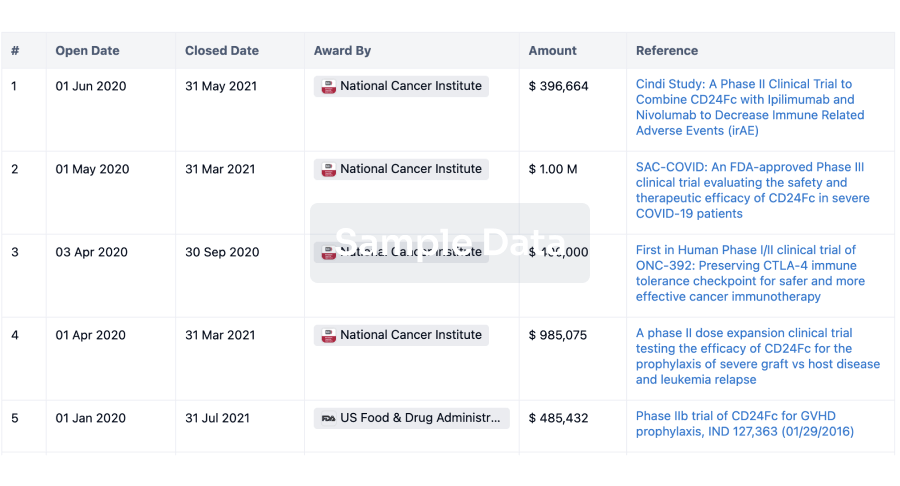
Grant & Funding(NIH)
Access more than 2 million grant and funding information to elevate your research journey.
login
or
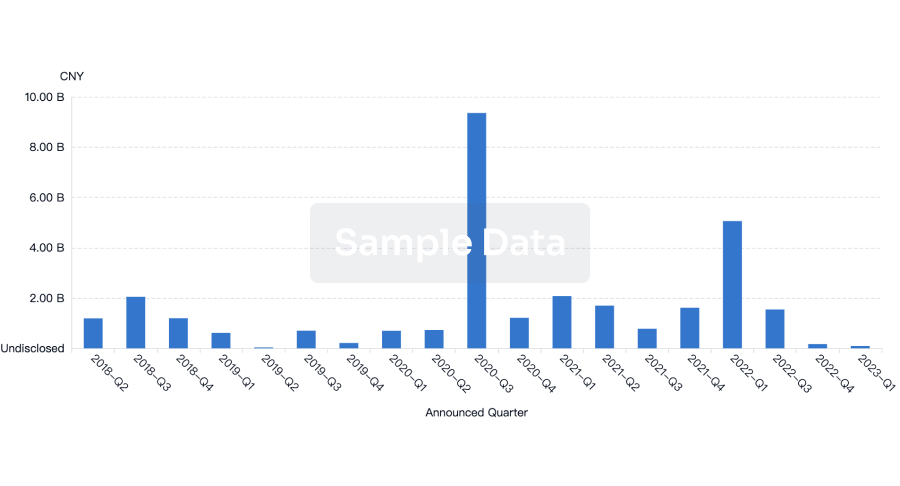
Investment
Gain insights on the latest company investments from start-ups to established corporations.
login
or
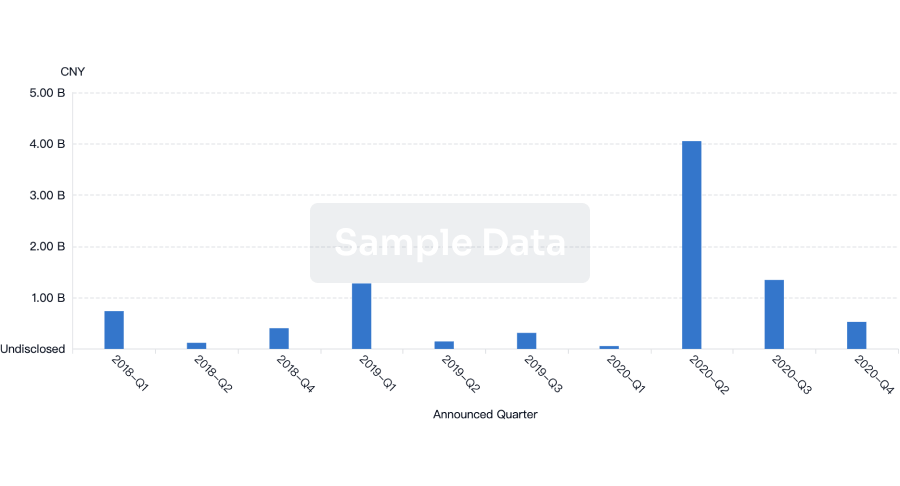
Financing
Unearth financing trends to validate and advance investment opportunities.
login
or
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free