Last update 04 Nov 2024
Chongqing Emergency Medical Center
Last update 04 Nov 2024
Overview
Related
Magnetocardiography in the Identification and Risk Stratification of Patients With Acute Chest Pian
Identification of Myocardial Ischemia With Magnetocardiography Using Single Photon Emission Computed Tomography (SPECT) as a Reference Standard
A multicentre retrospective study: early evaluation of organ damage in heat stroke patients
100 Clinical Results associated with Chongqing Emergency Medical Center
Login to view more data
Login to view more data
31 Dec 2024AUTOIMMUNITY
Osteocyte-derived exosomes regulate the DLX2/wnt pathway to alleviate osteoarthritis by mediating cartilage repair
Article
Author: Pan, Liyan ; Li, Lijuan ; Li, Wei ; Lu, Li ; Xu, Wenjuan ; Zhi, Shenshen ; Zhang, Yuanyuan
BACKGROUND:
Chondrocyte viability, apoptosis, and migration are closely related to cartilage injury in osteoarthritis (OA) joints. Exosomes are identified as potential therapeutic agents for OA.
OBJECTIVE:
This study aimed to investigate the role of exosomes derived from osteocytes in OA, particularly focusing on their effects on cartilage repair and molecular mechanisms.
METHODS:
An injury cell model was established by treating chondrocytes with IL-1β. Cartilage repair was evaluated using cell counting kit-8, flow cytometry, scratch test, and Western Blot. Molecular mechanisms were analyzed using quantitative real-time PCR, bioinformatic analysis, and Western Blot. An OA mouse model was established to explore the role of exosomal DLX2 in vivo.
RESULTS:
Osteocyte-released exosomes promoted cell viability and migration, and inhibited apoptosis and extracellular matrix (ECM) deposition. Moreover, exosomes upregulated DLX2 expression, and knockdown of DLX2 activated the Wnt pathway. Additionally, exosomes attenuated OA in mice by transmitting DLX2.
CONCLUSION:
Osteocyte-derived exosomal DLX2 alleviated IL-1β-induced cartilage repair and inactivated the Wnt pathway, thereby alleviating OA progression. The findings suggested that osteocyte-derived exosomes may hold promise as a treatment for OA.
01 Nov 2024ULTRASOUND IN MEDICINE AND BIOLOGY
Deep Learning With Ultrasound Images Enhance the Diagnosis of Nonalcoholic Fatty Liver
Article
Author: Liu, Yao ; Li, Jin ; Yu, Wenrou ; Wang, Peizheng ; Huang, Yingzhou ; Li, Pan
01 Oct 2024International Journal of Surgery Case Reports
Fallopian tube cancer with inguinal lymph node metastasis as the first symptom: A case study and review of the literature
Article
Author: Yang, Qiyu ; Han, Shichao ; Su, Qing ; Pan, Zhuo ; Yin, Rong
INTRODUCTION AND IMPORTANCE:
Fallopian tube cancer that is characterized only by inguinal lymph node metastasis without intra-abdominal widespread is rare. Here we report a patient with primary Fallopian tube cancer with bilateral inguinal metastases as the first symptom.
CASE PRESENTATION:
A 68-year-old patient with primary Fallopian tube cancer, with painless bilateral inguinal enlargement (7 × 6 cm on the right side, 3 × 2 cm on the left side) as the only manifestation, was confirmed by preoperative biopsy as metastatic high-grade serous denocarcinoma, consider the adnexal or peritoneal source. Pelvic MRI, abdominal CT and PET-CT showed irregular signal foci can be seen in the right adnexal area, with a maximum cross-section of about 7.5 × 7.0 × 4.0 cm, considering malignancy, ovarian cancer may be possible; bilateral pelvic wall, bilateral inguinal, right iliac vessels with hypermetabolic lymph nodes. Serum CA125 level was markedly elevated at 922.40 U/ml and HE4 at 394.50 pmol/L. No abnormality was found in gastrointestinal endoscopy. At exploratory laparotomy, the tumor was confined to the right rear of the uterus, and a solid tumor with a size of about 10 × 6 × 6 cm was seen. The surface was smooth and closely related to the uterus. There was almost no tumor spread in the pelvic abdominal cavity, but there was 50 ml of pale blood-colored peritoneal fluid. The right ovarian capsule was intact. Cytoreductive surgery was performed, postoperative pathology confirmed adenocarcinoma of the right fallopian tube, and the patient received six cycles of paclitaxel plus cisplatin combination chemotherapy were administered, with three 3-weeks intervals between cycles. And subsequent the patient participated in a clinical trial. The work has been reported in line with the SCARE criteria.
CLINICAL DISCUSSION:
Literature review indicates that inguinal lymph node as the first manifestation of fallopian tube cancer is not usual, and with no widespread lymphadenopathies and abdominopelvic cavity are even rarer. This case shows that rare cases with only inguinal lymph node metastasis may occur through the underlying lymphatic and/or hematogenous routes.
CONCLUSION:
The diagnosis of tubal cancer is sometimes complicated and delayed. For elderly women without nonspecific symptoms, especially those with obvious masses, detailed examinations, and imaging studies should be carried out in time. The treatment of tubal cancer is multi-modal. Due to the high risk of recurrence of fallopian tube cancer, the possibility of metastasis after the initial diagnosis is large, so it is very important to receive close and regular follow-up for patients with fallopian tube cancer after treatment. We suggest that more tumor centers study the possible mechanisms, metastasis patterns, biological characteristics, etc. of such patients, and at the same time efforts should be made to early differential diagnosis, and ultimately prolong the survival time of such patients.
100 Deals associated with Chongqing Emergency Medical Center
Login to view more data
100 Translational Medicine associated with Chongqing Emergency Medical Center
Login to view more data
Corporation Tree
Boost your research with our corporation tree data.
login
or
Pipeline
Pipeline Snapshot as of 27 Dec 2024
No data posted
Login to keep update
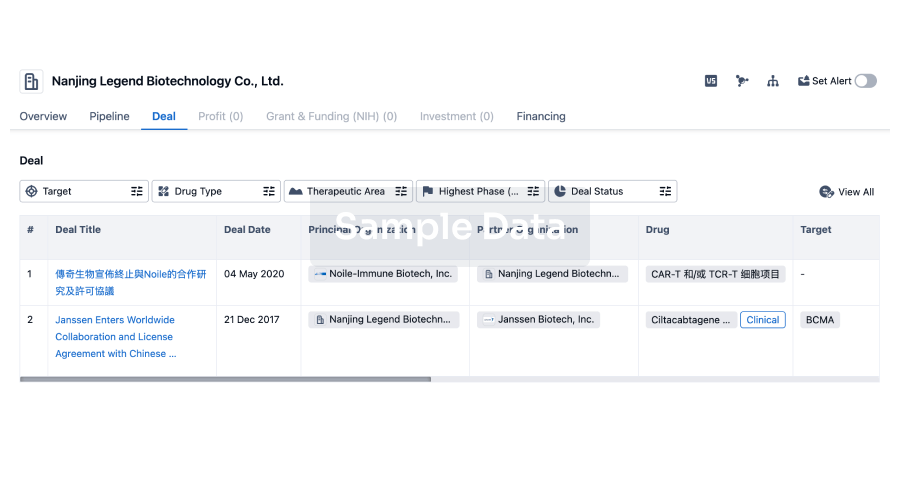
Deal
Boost your decision using our deal data.
login
or
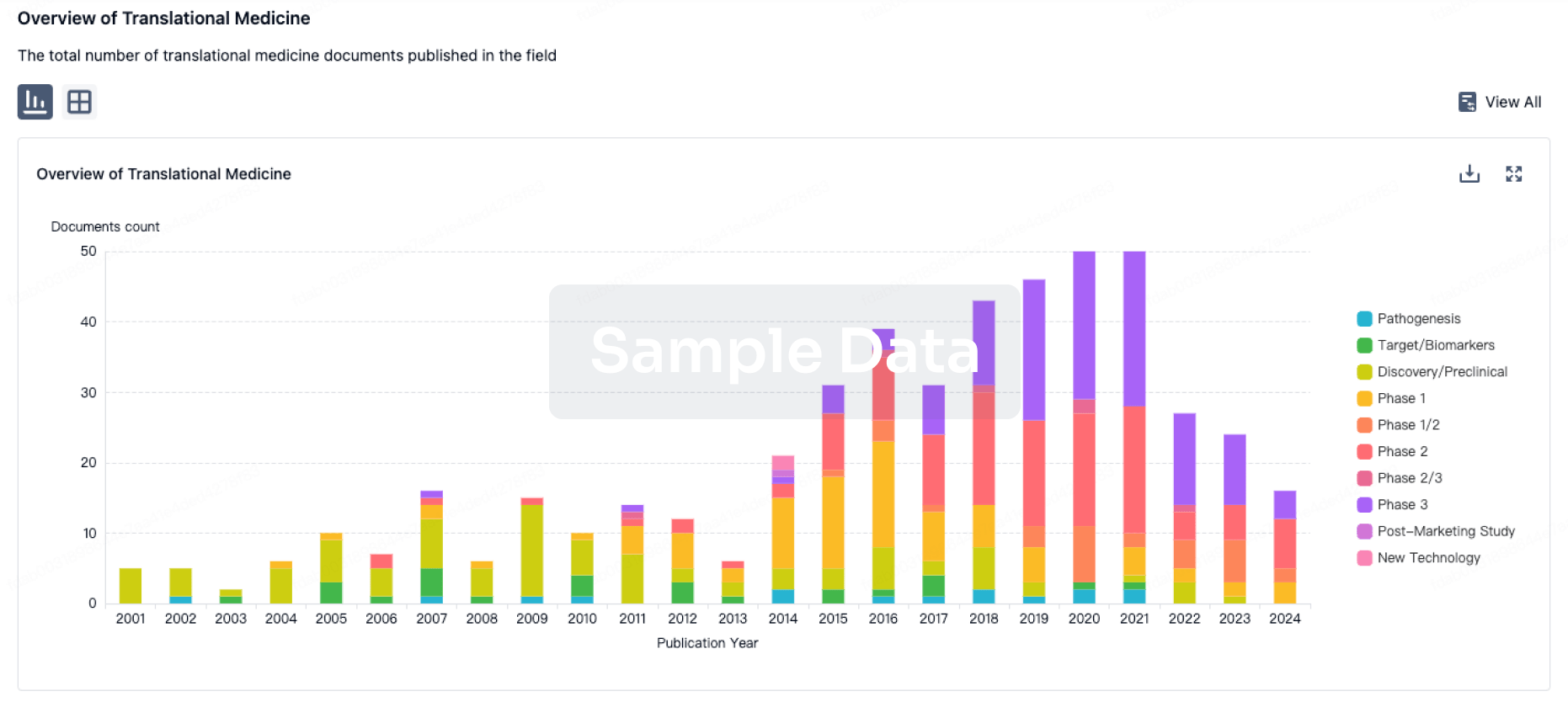
Translational Medicine
Boost your research with our translational medicine data.
login
or
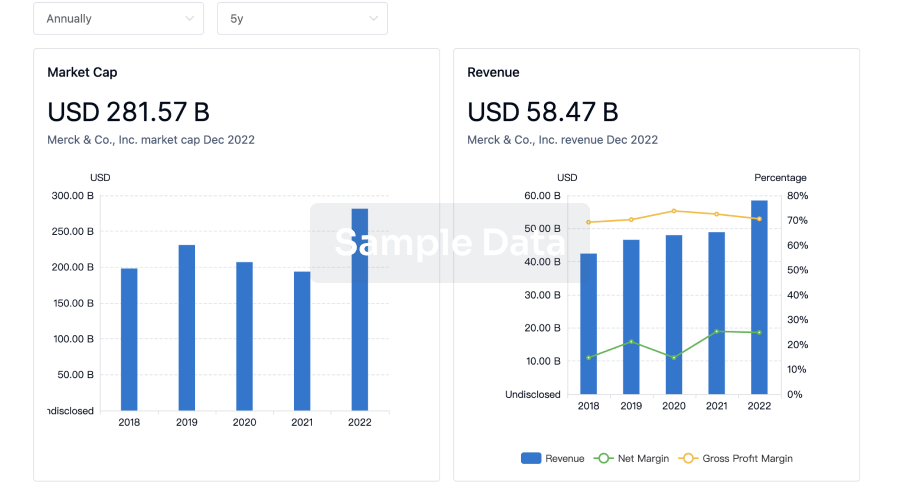
Profit
Explore the financial positions of over 360K organizations with Synapse.
login
or
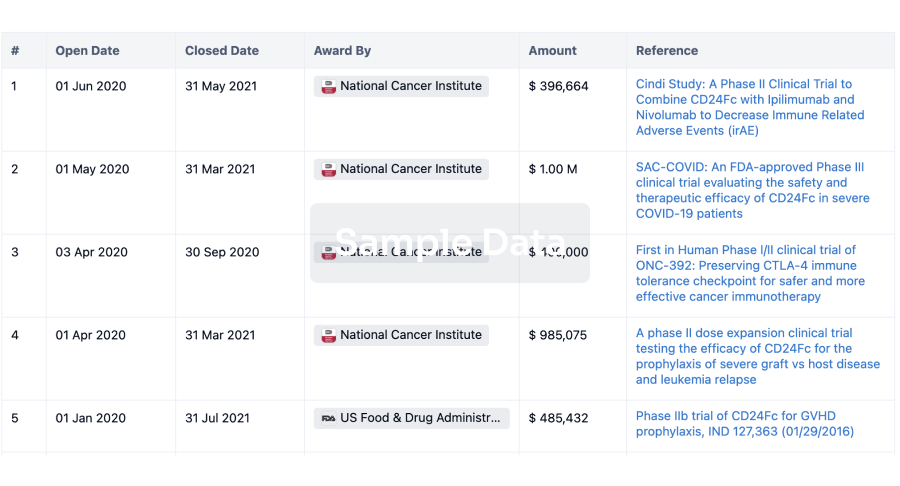
Grant & Funding(NIH)
Access more than 2 million grant and funding information to elevate your research journey.
login
or
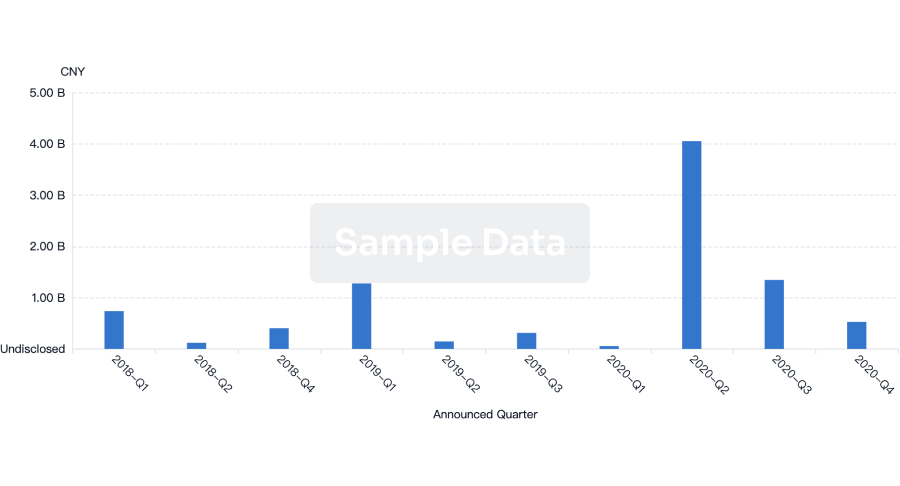
Investment
Gain insights on the latest company investments from start-ups to established corporations.
login
or

Financing
Unearth financing trends to validate and advance investment opportunities.
login
or
Chat with Hiro
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free