Request Demo
Last update 08 Mar 2026
East Kent Hospitals University NHS Foundation Trust
Last update 08 Mar 2026
Overview
Related
NCT07198737
Effect of Virtual Reality and Trans Auricular X-Vagus Nerve Stimulation for Anxiety and Depression in Chronic Shoulder Pain Patients
NCT07274098
A Randomised Controlled Pilot Study of the Effectiveness of a VR Headset on Post Operative Relaxation, Anxiety and Pain in Patients Undergoing Elective Laparoscopic Colorectal Surgery
ISRCTN15234554
Post-market clinical follow-up study to provide safety, performance and clinical benefits data of the Zimmer® Natural Nail® antegrade and retrograde femoral nail (implants and instrumentation) – a retrospective consecutive series study
100 Clinical Results associated with East Kent Hospitals University NHS Foundation Trust
Login to view more data
Login to view more data
01 Feb 2026BRITISH JOURNAL OF CLINICAL PHARMACOLOGY
CYP2C19
genotype testing for clopidogrel: A guideline developed by the UK Centre of Excellence in Regulatory Science and Innovation in Pharmacogenomics (CERSI‐PGx)
Review
Author: Tom A. T. Hughes ; Stefanie Lip ; Aaron Peace ; Iain Frater ; Judith Hayward ; Sree Kondapally ; Luigi Venetucci ; Sophie Harding ; Nicholas Greaves ; Hannah O'Neill ; Salim Elyas ; Kerry Burke ; Patrick Mok ; Munir Pirmohamed ; Cinzia Dello Russo ; David Hargroves ; Imran Rafi ; Vicky Stinton ; Rebecca Kuruvilla ; Vicky Chaplin ; Simon Ray ; Dyfrig A. Hughes ; Alexander S. F. Doney
Clopidogrel, an antiplatelet agent, is currently licensed in the United Kingdom for the prevention and treatment of atherothrombotic events in cerebrovascular disease, coronary artery disease and peripheral arterial disease. Clopidogrel requires metabolic activation by the cytochrome P450 enzyme CYP2C19 to be effective. CYP2C19 is encoded by a polymorphic gene; variants in the
CYP2C19
gene, which vary in frequency in different ethnic groups can abolish, reduce or increase enzyme activity, thereby affecting the conversion of clopidogrel to its active metabolite. Individuals who have either one or two loss‐of‐function alleles are referred to as intermediate and poor metabolisers, respectively, and in these patients, the clinical effectiveness of clopidogrel is reduced or absent. Any patient about to be prescribed clopidogrel, regardless of the underlying indication, should have pharmacogenetic testing to identify clinically relevant
CYP2C19
variants, where testing is available, to optimize their antiplatelet therapy. Clopidogrel use should be avoided in patients with an intermediate or poor CYP2C19 metaboliser phenotype in all approved indications and alternative treatment regimens used as detailed in this guideline. Our guideline is compatible with other international pharmacogenetic prescribing guidelines, but we also provide recommendations in other areas. Summary guidance on a page is provided for each of the indications in Boxes 1–3. This guideline is grounded in the latest evidence in this field but cannot account for all individual factors relevant to patient care. Therefore, prescribers must conduct a thorough assessment of each patient's risk–benefit profile, ensuring that therapy is optimized to maximize benefits while minimizing potential harms.
01 Jan 2026ANNALS OF THE ROYAL COLLEGE OF SURGEONS OF ENGLAND
A national survey of the diagnosis and management of Ménière’s disease among ENT consultants, UK
Article
Author: Neumann, C ; Kanegaonkar, RG ; Parihar, S ; Koumpa, FS
Introduction:
Ménière's disease (MD) is a rare condition whose diagnosis can be challenging. The American Academy of Otorhinolaryngology-Head and Neck Surgeons (AAO-HNS) has published new guidance to facilitate the diagnosis of MD. We surveyed ear, nose and throat (ENT) consultants in the United Kingdom (UK) to assess their confidence in diagnosing MD, their use of the AAO-HNS guidance and current diagnostic and treatment approaches.
Methods:
An online questionnaire was distributed. It asked respondents to anonymously rank their confidence in diagnosing MD, identify the minimum investigations required to make a diagnosis, describe their use of the AAO-HNS criteria, share their preferred treatment for acute attacks and state first- and second-line preventative treatment options.
Results:
A total of 86 responses were collected. In total, 88% of respondents reported high levels of confidence in diagnosing MD. Most respondents (29.1%) stated the minimum tests required were ‘history’, ‘otoscopy’, ‘pure tone audiometry’ and ‘MRI’ (magnetic resonance imaging), although some chose as few as one test (3.49%) and others up to seven (1.2%). Regarding use of the AAO-HNS criteria, responses ranged from ‘always’ (34.9%) to ‘never’ (20.9%). Prochlorperazine was the first-line treatment for acute attacks for 81.4% of respondents. Betahistine (38.4%) and dietary restrictions (37.2%) were recommended almost equally as first-line preventative measures. The most popular second-line measure was intratympanic steroids (34.9%), followed by betahistine (24.4%).
Conclusion:
Our survey revealed wide disparities in the diagnosis and management of MD by ENT consultants in the UK, and AAO-HNS guidelines were not universally used. We propose developing greater consensus and intend to conduct a similar international survey to gather a broader perspective.
01 Jan 2026European Journal of Nuclear Medicine and Molecular Imaging
A century in the making: Medical imaging, nuclear medicine, and the transformation of global healthcare
Review
Author: Bashir, Hassan ; Fanti, Stefano ; Bashir, Humayun
This paper explores how the global mobility of healthcare professionals shapes the evolution of nuclear medicine through shifts in labour, logistics, and knowledge systems. It examines how credentialing asymmetries, fragile supply infrastructures, and uneven digital integration affect equitable access to innovation and practice. The analysis highlights how professional circulation generates both collaboration and structural exclusion, particularly when expertise crosses regulatory and institutional boundaries. It argues that mobility not only redistributes clinical skills but also redefines authority, standards, and epistemologies in medical imaging. By tracing these dynamics, the paper opens space for rethinking inclusion, accountability, and fairness in the global development of medical imaging and nuclear medicine.
100 Deals associated with East Kent Hospitals University NHS Foundation Trust
Login to view more data
100 Translational Medicine associated with East Kent Hospitals University NHS Foundation Trust
Login to view more data
Corporation Tree
Boost your research with our corporation tree data.
login
or
Pipeline
Pipeline Snapshot as of 14 Mar 2026
No data posted
Login to keep update
Deal
Boost your decision using our deal data.
login
or

Translational Medicine
Boost your research with our translational medicine data.
login
or

Profit
Explore the financial positions of over 360K organizations with Synapse.
login
or

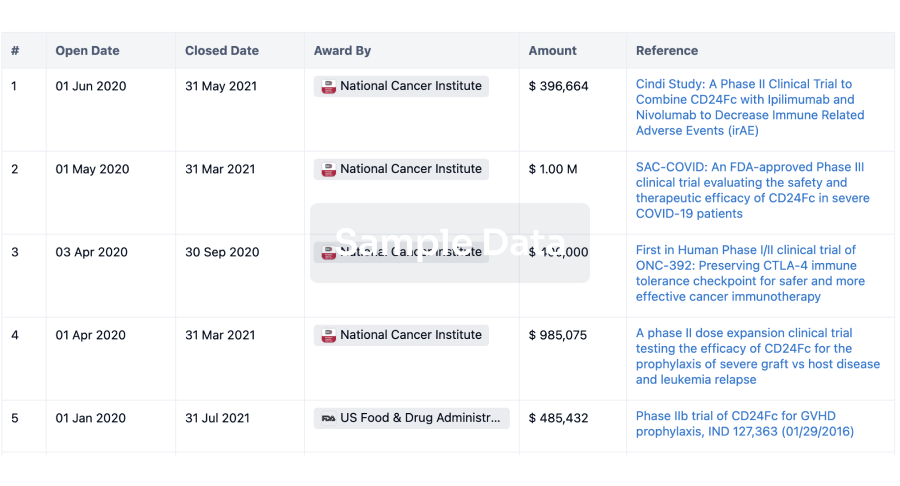
Grant & Funding(NIH)
Access more than 2 million grant and funding information to elevate your research journey.
login
or
Investment
Gain insights on the latest company investments from start-ups to established corporations.
login
or

Financing
Unearth financing trends to validate and advance investment opportunities.
login
or

AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free