Request Demo
Last update 08 May 2025

Yerevan State Medical University
Last update 08 May 2025
Overview
Related
ISRCTN16280803
A pilot study of Thulium RevoLix laser usage for tonsillectomy
NCT04306627
Evaluation of Carotid Intima Media Thickness by Treatment of Vascular and Metabolic Factors With Combined Antihypertensive and Hypolipidemic Therapy
100 Clinical Results associated with Yerevan State Medical University
Login to view more data
Login to view more data
01 May 2025Journal of Autoimmunity
Long-term efficacy and safety of colchicine and anti-IL-1 blockers in FMF: results from the Eurofever multicenter observational study
Article
Author: Porreca, Annamaria ; Rigante, Donato ; Bella, Saverio La ; Frenkel, Joost ; Horneff, Gerd ; Bakkaloglu, Sevcan ; Kasapcopur, Ozgur ; Simonini, Gabriele ; Sánchez-Manubens, Judith ; Legger, Elizabeth ; Bayindir, Yagmur ; Anton, Jordi ; Amarilyo, Gil ; Obici, Laura ; Jesenak, Milos ; Belder, Nuran ; Glerup, Mia ; Insalaco, Antonella ; Amaryan, Gayane ; Ozen, Seza ; Cantarini, Luca ; Brunner, Juergen ; Gattorno, Marco ; Fabio, Giovanna ; Alataki, Sofia ; Assalia, Naiera ; Alessio, Maria ; Bustaffa, Marta ; Spagnolo, Alessandra ; Ruperto, Nicolino ; Caorsi, Roberta ; Carrabba, Maria ; Gallizzi, Romina ; Breda, Luciana ; Kuemmerle-Deschner, Jasmin ; Papadopoulou-Alataki, Efimia
01 May 2025Bone
Decoding fracture healing: A scoping review of mechanistic pathways derived from transcriptional analysis in murine studies
Review
Author: Nafisi, Nazanin ; Mirzamohammadi, Hamid ; Nazarian, Ara ; Manoukian, David ; Klujian, Arthur ; Khak, Mohammad ; Mirzamohammadi, Fatemeh ; Shariyate, Mohammad Javad ; Rostami, Mahboubeh R ; Velasquez, Maria V ; Cummiskey, Tom ; Razavi, Ahmad Hedayatzadeh
23 Apr 2025European Heart Journal: Acute Cardiovascular Care
The impact of total ischemic time on in-hospital mortality and complications in patients with ST-elevation myocardial infarction
Author: Hayrapetyan, H G ; Arakelyan, I A ; Petrosyan, H H ; Muradyan, F I ; Hayrapetyan, L H ; Ter-Grigoryan, V R
100 Deals associated with Yerevan State Medical University
Login to view more data
100 Translational Medicine associated with Yerevan State Medical University
Login to view more data
Corporation Tree
Boost your research with our corporation tree data.
login
or
Pipeline
Pipeline Snapshot as of 19 Dec 2025
No data posted
Login to keep update
Deal
Boost your decision using our deal data.
login
or
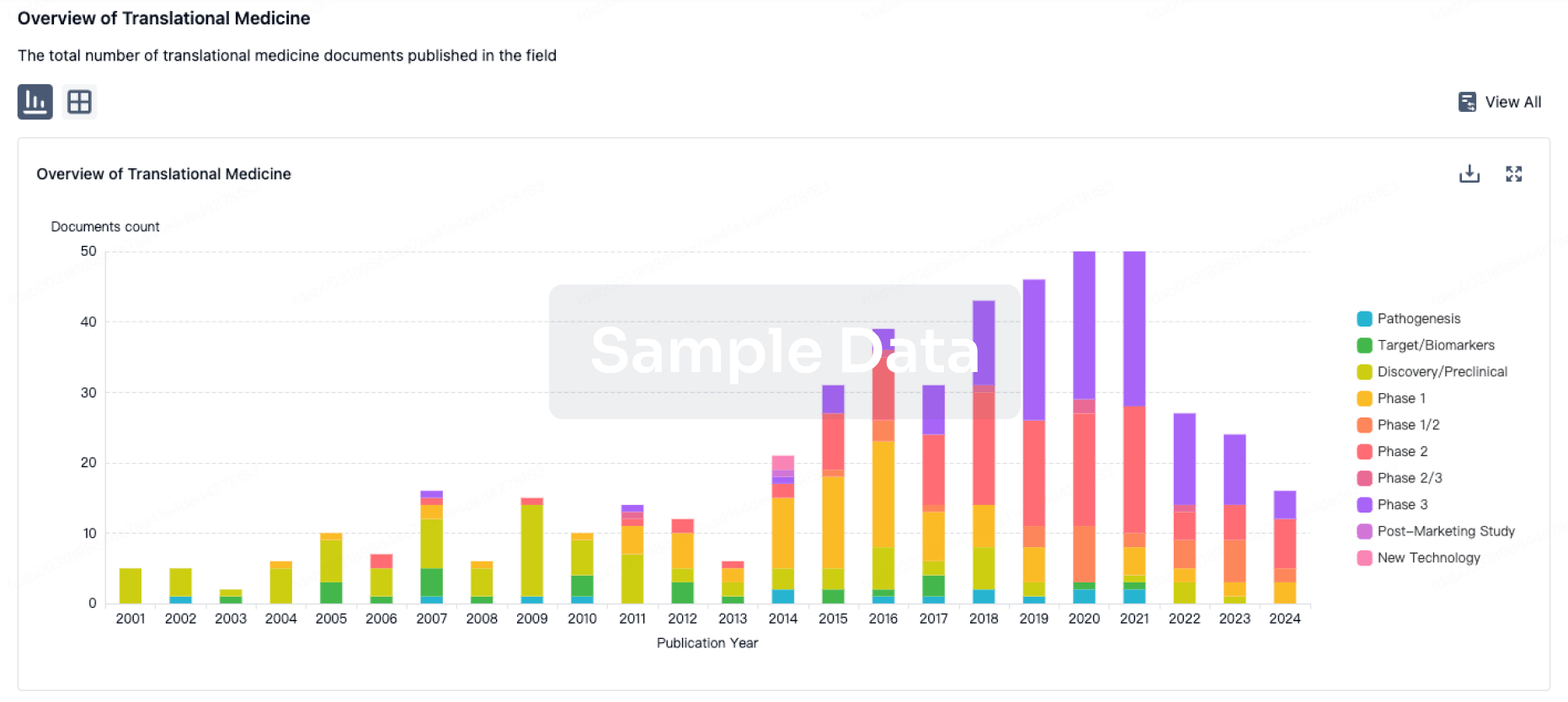
Translational Medicine
Boost your research with our translational medicine data.
login
or
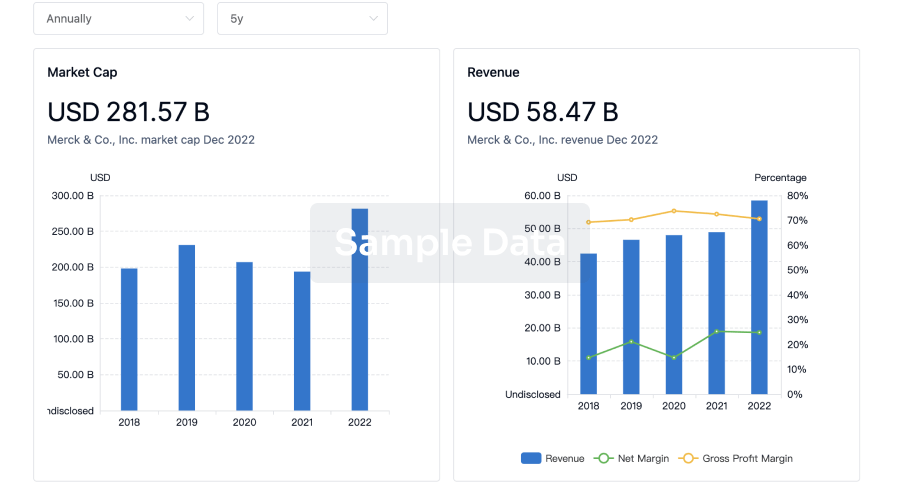
Profit
Explore the financial positions of over 360K organizations with Synapse.
login
or
Grant & Funding(NIH)
Access more than 2 million grant and funding information to elevate your research journey.
login
or

Investment
Gain insights on the latest company investments from start-ups to established corporations.
login
or
Financing
Unearth financing trends to validate and advance investment opportunities.
login
or
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free