Request Demo
Last update 09 Sep 2025
Wyckoff Heights Medical Center, Inc.
Last update 09 Sep 2025
Overview
Related
NCT01315808
Rate of Change of HbA1c (dx/dt) May Predict Progression to Type 2 DM: Comparing the Concept of dx/dt With QD Diabetes Prediction Model. D.E.R.M.S Initiative (Doctor Enabled Risk Management System)
100 Clinical Results associated with Wyckoff Heights Medical Center, Inc.
Login to view more data
Login to view more data
01 Nov 2025MICROVASCULAR RESEARCH
Comparative analysis of superficial collecting lymph vessels in normal tissue and lymphedema using video-capillaroscopy
Article
Author: Tsukuura, Reiko ; Nishimura, Takayoshi ; Matsui, Chihiro ; Mortada, Hatan ; Tanaka, Takakuni ; Arai, Go ; Escandón, Joseph M ; Miyazaki, Toko ; Ishibashi, Shigeki ; Yamamoto, Takumi
INTRODUCTION:
Lymphedema is a chronic, progressive disorder characterized by impaired lymphatic transport, tissue swelling, and fibrosis. This study used video-capillaroscopy, a high-resolution imaging technique, to assess superficial collecting lymphatic vessels and their vasa vasorum in patients with lymphedema. By comparing these microvascular structures to those in healthy tissue, we aimed to identify early vascular changes contributing to disease progression.
METHODS:
VC recordings were retrospectively analyzed from 28 limbs in 17 patients with lower extremity lymphedema and 53 lymphatic vessels in 12 cancer patients undergoing reconstructive surgery. In the latter group, observations were performed on normal subcutaneous tissue exposed at the donor site during flap harvest. These areas showed no tumor involvement, regional metastasis, or prior chemotherapy/radiotherapy. Thus, all normal tissue observations were made on untreated, unaffected sites. VCLs were classified into six stages (0-5) based on morphology and flow. Vessel diameter and red blood cell (RBC) velocity were measured. Statistical significance was set at p < 0.05.
RESULTS:
In normal donor tissue, mean VCL main vessel diameter and RBC velocity were 0.038 ± 0.031 mm and 185 ± 160.5 μm/s. In lymphedema, these values were reduced to 0.033 ± 0.024 mm and 28.3 ± 36.8 μm/s (p < 0.001). VCL Stage 0 showed preserved flow (p = 0.178), while Stages 1-5 exhibited progressive impairment.
CONCLUSION:
These findings suggest that early ischemic changes in the vasa vasorum may precede lymphatic dysfunction and fibrosis in lymphedema. Preserving microvascular integrity should be a therapeutic focus, alongside drainage support. Further studies are needed to clarify clinical relevance and optimize treatment strategies.
12 Aug 2025Journal of Personalized Medicine
Poly-4-Hydroxybutyrate as a Novel Biomaterial in Personalized Breast Surgery: A Systematic Review and Meta-Analysis.
Review
Author: Boyd, Carter J ; Escandón, Joseph M ; Karp, Nolan S ; Manrique, Oscar J ; Vyas, Krishna ; Kreutz-Rodrigues, Lucas ; Nugent, Ajani
Background/Objectives: In the search for optimal meshes and matrices in breast surgery, poly-4-hydroxybutyrate (P4HB) has emerged as a promising alternative. This review evaluates the clinical application of P4HB scaffolds, focusing on complication rates and surgical outcomes. Methods: A systematic search was conducted using PubMed and ScienceDirect. Clinical studies assessing perioperative outcomes and complications associated with P4HB scaffolds in breast surgery were included. Results were stratified into aesthetic and reconstructive surgery categories. Meta-analysis was implemented to assess the rate of complications and satisfaction. Results: This systematic review included 13 studies evaluating the use of P4HB scaffold in breast reconstruction (636 cases) and aesthetic breast surgery (462 patients). Breast reconstruction studies were all retrospective, mainly reporting two-stage, prepectoral, immediate reconstructions. Aesthetic studies included both prospective and retrospective designs, with varied implant planes and incision patterns. P4HB use was associated with high satisfaction (95.5%) and favorable outcomes, including lower odds of wound complications (log-OR = -1.135, p = 0.003). Complication rates were low across both surgical categories. P4HB scaffold showed promise in supporting implant-based procedures and maintaining breast shape over time, with minimal increase in surgical time and stable anthropometric measurements. Conclusions: The use of P4HB scaffold in breast reconstruction and aesthetic surgery shows promising results, notably in reducing wound-related complications. Breast reconstruction studies report low complication rates and favorable patient-reported outcomes. In aesthetic procedures, P4HB contributes to improved long-term breast shape and high satisfaction. Despite encouraging findings, further research is necessary to validate long-term efficacy and refine surgical approaches.
01 Aug 2025JAMA Pediatrics
US Neonatal Mortality From Perinatal Causes
Article
Author: Rath, Shree ; Eda, Sanjay ; Afaq, Munaza ; Aziz, Nouman ; Nabi, Waseem ; Bin Gulzar, Abu Huraira ; Khan, Muzamil
This cohort study identifies the top 10 perinatal complications–related causes of newborn deaths from 1999 to 2022.
15 May 2025
Diagnostic ReagentsClinical Result
15 Nov 2022
Executive Change
100 Deals associated with Wyckoff Heights Medical Center, Inc.
Login to view more data
100 Translational Medicine associated with Wyckoff Heights Medical Center, Inc.
Login to view more data
Corporation Tree
Boost your research with our corporation tree data.
login
or
Pipeline
Pipeline Snapshot as of 08 Dec 2025
No data posted
Login to keep update
Deal
Boost your decision using our deal data.
login
or
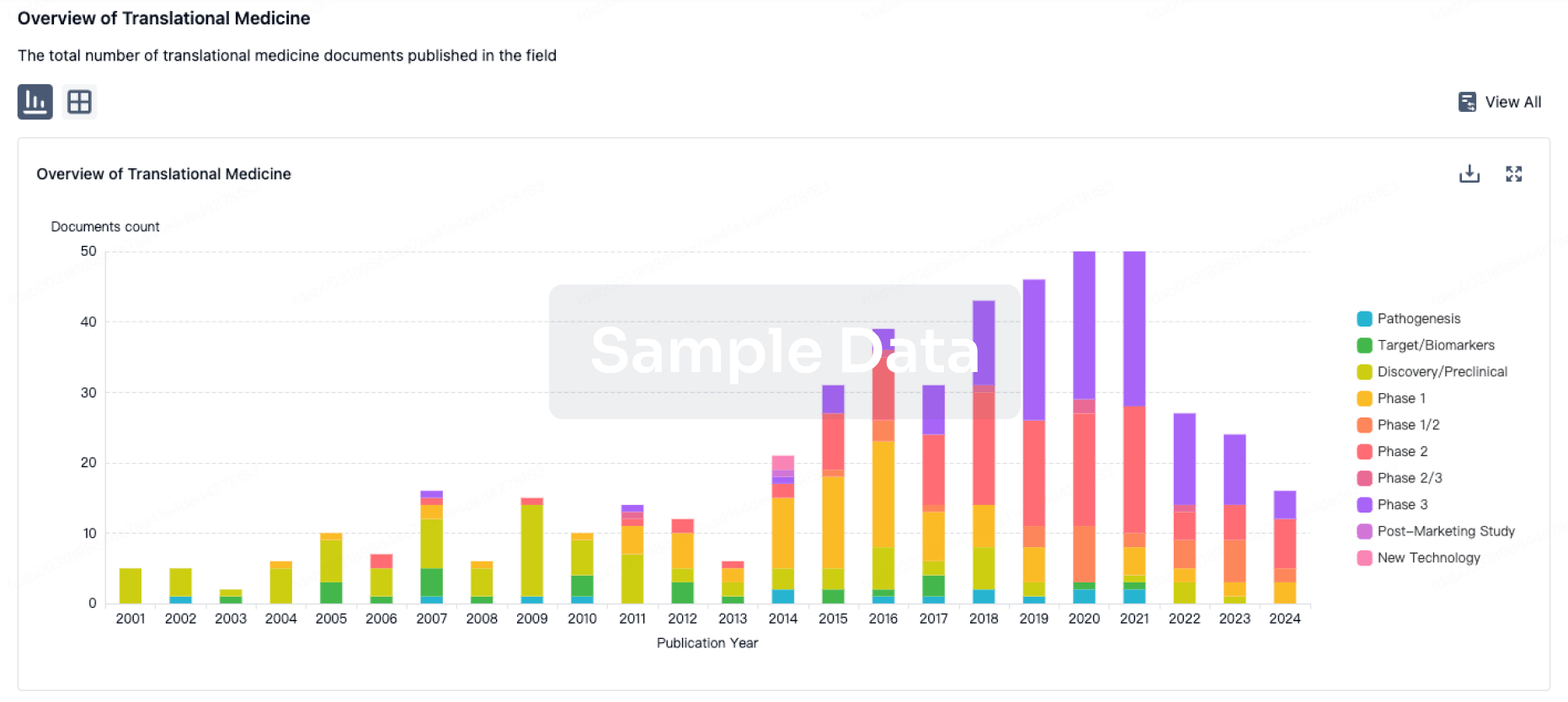
Translational Medicine
Boost your research with our translational medicine data.
login
or
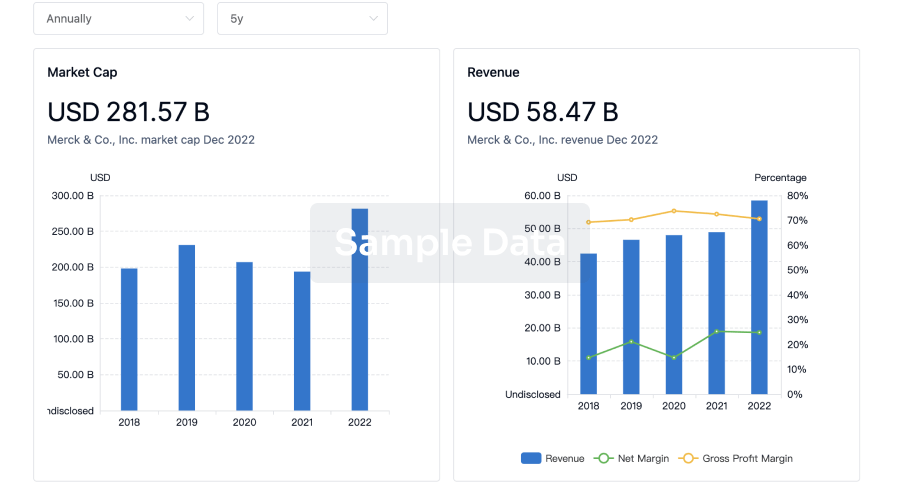
Profit
Explore the financial positions of over 360K organizations with Synapse.
login
or
Grant & Funding(NIH)
Access more than 2 million grant and funding information to elevate your research journey.
login
or

Investment
Gain insights on the latest company investments from start-ups to established corporations.
login
or
Financing
Unearth financing trends to validate and advance investment opportunities.
login
or
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free