Last update 06 Oct 2024
Toshiba America Medical Systems, Inc.
Subsidiary Company|
1875|
California, United States
Last update 06 Oct 2024
Overview
Related
The Value of Fractional Flow Reserve Derived From Coronary CT Angiography as Compared to CCTA or CCTA and Stress MPI in the Triage of Low to Intermediate Emergent Chest Pain Patients With Toshiba CT-FFR
Implementing Myocardial Computed Tomographic Perfusion in a Community Hospital Setting
ROMAN (PCA-9000A) PET/CT System Verification
100 Clinical Results associated with Toshiba America Medical Systems, Inc.
Login to view more data
Login to view more data
13 Mar 2017Proceedings of SPIE--the International Society for Optical Engineering
Design optimization for accurate flow simulations in 3D printed vascular phantoms derived from computed tomography angiography
Article
Author: Ionita, Ciprian N ; Izzo, Richard L ; Rudin, Stephen ; Shepard, Lauren ; Siddiqui, Adnan H ; Springer, Michael ; Sommer, Kelsey ; Wilson, Michael F ; Said, Zaid ; Angel, Erin ; Podgorsak, Alexander R
3D printing has been used to create complex arterial phantoms to advance device testing and physiological condition evaluation. Stereolithographic (STL) files of patient-specific cardiovascular anatomy are acquired to build cardiac vasculature through advanced mesh-manipulation techniques. Management of distal branches in the arterial tree is important to make such phantoms practicable. We investigated methods to manage the distal arterial flow resistance and pressure thus creating physiologically and geometrically accurate phantoms that can be used for simulations of image-guided interventional procedures with new devices. Patient specific CT data were imported into a Vital Imaging workstation, segmented, and exported as STL files. Using a mesh-manipulation program (Meshmixer) we created flow models of the coronary tree. Distal arteries were connected to a compliance chamber. The phantom was then printed using a Stratasys Connex3 multimaterial printer: the vessel in TangoPlus and the fluid flow simulation chamber in Vero. The model was connected to a programmable pump and pressure sensors measured flow characteristics through the phantoms. Physiological flow simulations for patient-specific vasculature were done for six cardiac models (three different vasculatures comparing two new designs). For the coronary phantom we obtained physiologically relevant waves which oscillated between 80 and 120 mmHg and a flow rate of ~125 ml/min, within the literature reported values. The pressure wave was similar with those acquired in human patients. Thus we demonstrated that 3D printed phantoms can be used not only to reproduce the correct patient anatomy for device testing in image-guided interventions, but also for physiological simulations. This has great potential to advance treatment assessment and diagnosis.
01 Dec 2016Congenital heart diseaseQ3 · MEDICINE
Radiation Protocol for Three-Dimensional Rotational Angiography to Limit Procedural Radiation Exposure in the Pediatric Cardiac Catheterization Lab
Q3 · MEDICINE
Article
Author: Johnson, Jason ; McGhee, Vera ; Zurakowski, David ; Kuhls-Gilcrist, Andrew ; Sathanandam, Shyam ; Choudhri, Asim ; Waller, B. Rush ; Haddad, Lauren
BACKGROUND:
Three-dimensional rotational angiography (3DRA) offers more detailed anatomic information than 2D digital acquisition (2DDA). Concerns over potentially higher contrast and radiation doses have limited its routine use.
OBJECTIVE:
The primary objective of this study was to compare radiation doses required to obtain 3DRA using a customized low dose radiation protocol with 2DDA. The secondary objective was to compare total procedural radiation in pediatric cardiac catheterization procedures utilizing 3DRA to those that do not.
STUDY DESIGN:
Phantom studies were conducted to establish customized 3DRA protocols for radiation reduction. Comparison of 3DRA and non-3DRA procedures in age-, size- and diagnosis-matched controls was performed. Radiation doses were indexed to body surface area (BSA) to account for differing body habitus as validated from the phantom study.
RESULTS:
Study (n = 100) and control (n = 100) groups were matched for age (10.2 vs. 9.98 years; P = .239) and BSA (1.23 vs. 1.09 m2 ; P = .103). The dose area product (DAP) to acquire a 3DRA was similar to a 5 s, 15 frames/second 2DDA (278 vs. 241 cGy/cm2 ; P = .14). Despite the 3DRA group consisting of more complex interventions, no difference was found in the total procedural Air Kerma and DAP indexed to BSA (244 vs. 249 mGy/m2 ; P = .79 and 3348 vs. 3176 cGy/cm2 /m2 ; P = .48, respectively). The contrast volume to acquire a 3DRA compared to a 2DDA was greater (1.59 vs. 1.01 mL/kg; P < .001). However, no difference was found for the entire procedure (3.8 vs. 4 mL/kg, P = .494). This could have resulted from the need to obtain multiple 2DDAs to achieve the detail of a single 3DRA (11 vs. 7 per study; P < .001).
CONCLUSIONS:
When 3DRA, using the proposed protocols is employed, total procedural contrast and radiation doses are comparable with the sole use of biplane cine-angiograms. These protocols may allow for routine use of 3DRA for congenital cardiac catheterizations.
01 Apr 2016Seminars in ultrasound, CT, and MRQ4 · MEDICINE
Cerebrospinal Fluid Dynamics and the Pathophysiology of Hydrocephalus: New Concepts
Q4 · MEDICINE
Review
Author: Kelly, Erin ; Yamada, Shinya
Many controversies remain regarding basic cerebrospinal fluid (CSF) physiology and the mechanism behind the development of hydrocephalus. Recent information obtained from CSF time spatial spin labeling inversion pulse method discovers different aspect of CSF dynamics. In this article, we would discuss how recent CSF imaging advances are leading to new concepts of CSF flow dynamics and the pathophysiology of hydrocephalus, with an emphasis on time spatial spin labeling inversion pulse imaging of CSF dynamics.
100 Deals associated with Toshiba America Medical Systems, Inc.
Login to view more data
100 Translational Medicine associated with Toshiba America Medical Systems, Inc.
Login to view more data
Corporation Tree
Boost your research with our corporation tree data.
login
or
Pipeline
Pipeline Snapshot as of 06 Oct 2024
No data posted
Login to keep update
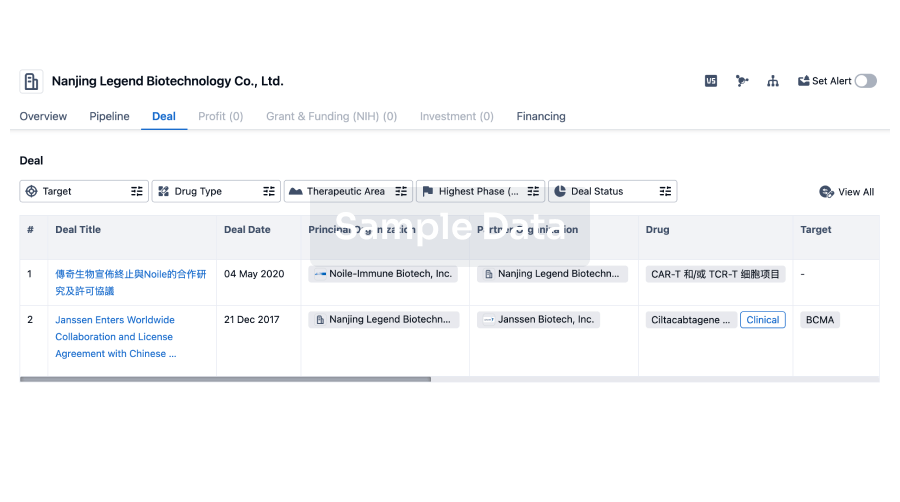
Deal
Boost your decision using our deal data.
login
or
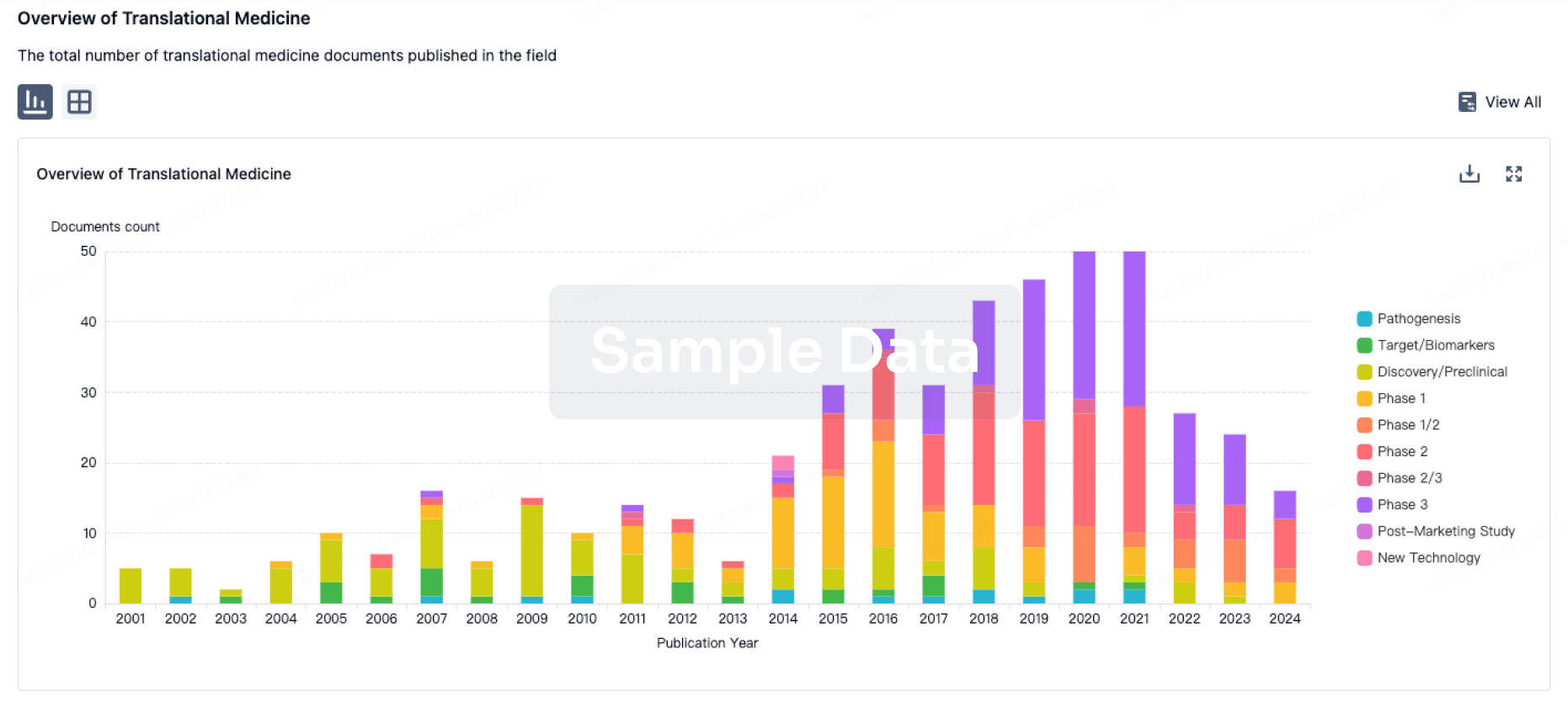
Translational Medicine
Boost your research with our translational medicine data.
login
or
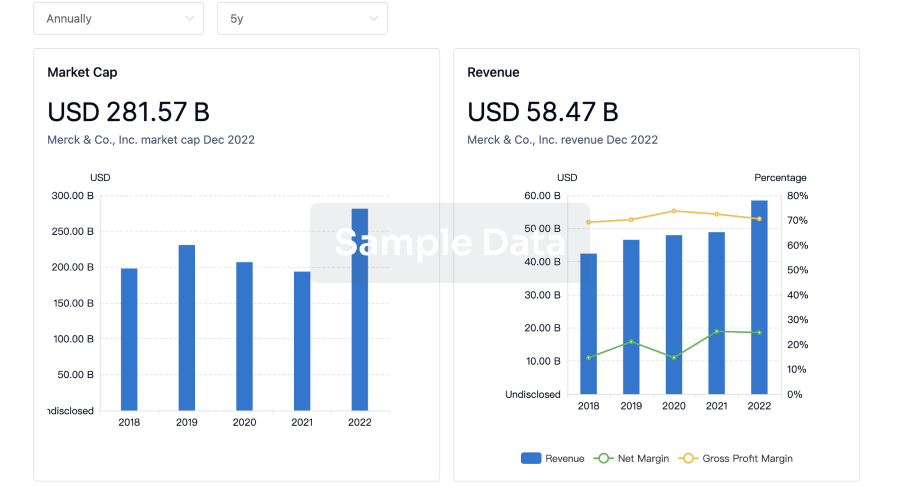
Profit
Explore the financial positions of over 360K organizations with Synapse.
login
or
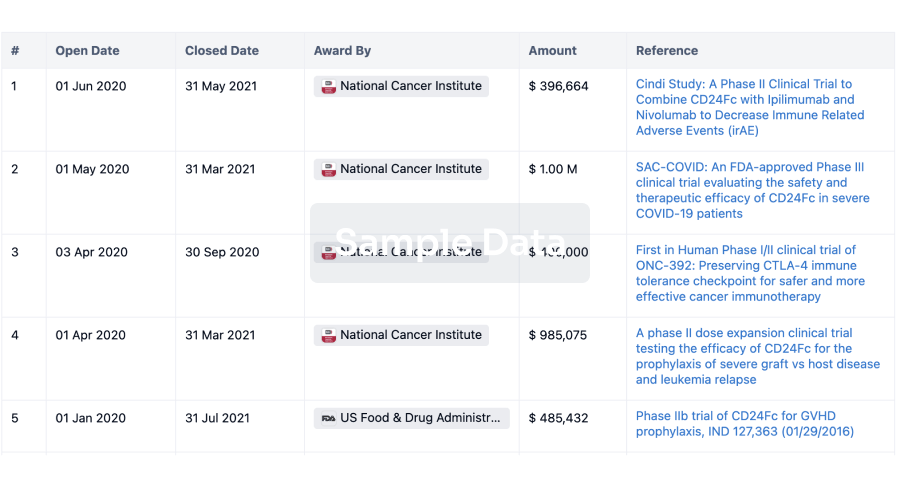
Grant & Funding(NIH)
Access more than 2 million grant and funding information to elevate your research journey.
login
or
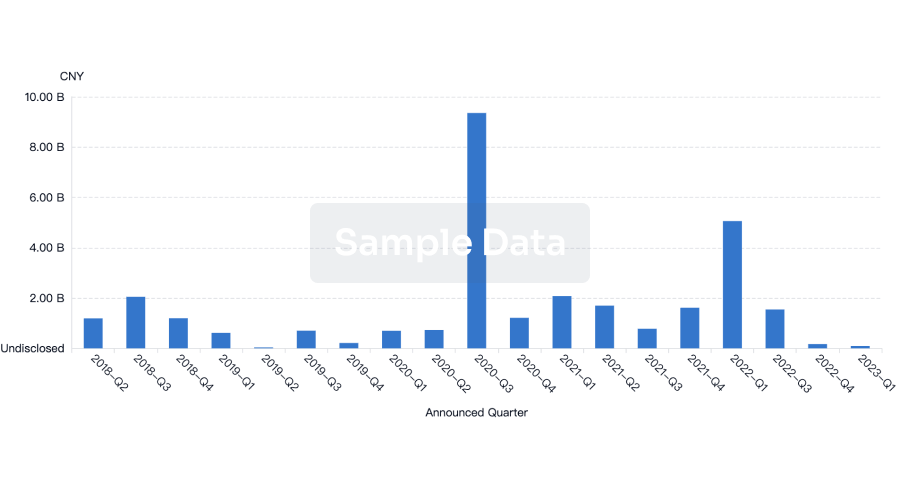
Investment
Gain insights on the latest company investments from start-ups to established corporations.
login
or
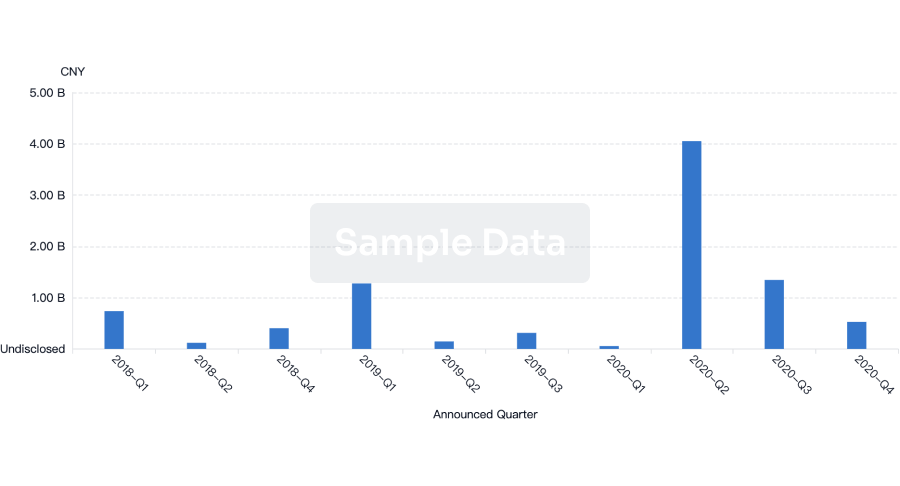
Financing
Unearth financing trends to validate and advance investment opportunities.
login
or
Chat with Hiro
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free