Request Demo
Last update 10 Dec 2025
Chosun University Hospital
Last update 10 Dec 2025
Overview
Basic Info
Introduction Chosun University, located in the Gwangju metropolitan area of South Korea, is a well-established private institution of higher education. With an enrollment of approximately 33,000 students, it is considered one of the most prominent universities in the country. |
Tags
Skin and Musculoskeletal Diseases
Immune System Diseases
Other Diseases
Small molecule drug
Synthetic peptide
Disease domain score
A glimpse into the focused therapeutic areas

Technology Platform
Most used technologies in drug development
Targets
Most frequently developed targets
Related
Target |
Mechanism |
Active Org. |
Originator Org. |
Active Indication |
Inactive Indication |
Drug Highest Phase |
First Approval Ctry. / Loc. |
First Approval Date |
Target |
Mechanism |
Active Org. |
Originator Org. |
Active Indication |
Inactive Indication |
Drug Highest Phase |
First Approval Ctry. / Loc. |
First Approval Date |
Target |
Mechanism |
Active Org. |
Originator Org. |
Active Indication |
Inactive Indication |
Drug Highest Phase |
First Approval Ctry. / Loc. |
First Approval Date |
KCT0011116
Efficacy and Safety of Oral Sulfate Tablets Versus 2L PEG for Bowel Preparation in Adults Aged 76 and Older: A Randomized Controlled Trial
KCT0010956
Comparative Evaluation of Ideal vs Actual Body Weight-Based Remimazolam Dosing in Obese Patients: A Randomized Controlled Trial
KCT0010953
Optimization of Initial Remimazolam Dosage for Achieving Adequate Anesthetic Depth in Young Adults – A Prospective Randomized Controlled Trial
100 Clinical Results associated with Chosun University Hospital
Login to view more data
Login to view more data
01 Jan 2026AMERICAN JOURNAL OF CARDIOLOGY
The Clinical Impact of Intravascular Imaging-Guided Percutaneous Coronary Intervention in Acute Myocardial Infarction Patients with High Thrombus Burden
Article
Author: Jeong, Jin-Ok ; Kim, Hyo-Soo ; Choi, Ki Hong ; Yun, Kyeong Ho ; Kim, Yisik ; Lee, Seung Hun ; Yoon, Chang-Hwan ; Lee, Joo Myung ; Park, Taek Kyu ; Hahn, Joo-Yong ; Choi, Seung-Hyuk ; Kwon, Woochan ; Yang, Jeong Hoon ; Hong, Young Joon ; Hur, Seung Ho ; Kim, Hyun Kuk ; Kim, Doo-Il ; Ahn, Young Keun ; Jo, Jinhwan ; Jeong, Myung Ho ; Park, Yong Hwan ; Kim, Ju Han ; Joh, Hyun Sung ; Gwon, Hyeon-Cheol ; Chang, Kiyuk ; Song, Young Bin ; Park, Hun Sik ; Bae, Jang-Whan ; Hwang, Jin-Yong ; Shin, Doosup
Despite the established clinical efficacy following intravascular imaging (IVI)-guided percutaneous coronary intervention (PCI) than angiography-guided PCI, evidence regarding prognostic benefits of IVI-guided PCI in acute myocardial infarction (AMI) patients with high thrombus burden remains limited. Using the nationwide registries of KAMIR-NIH and KAMIR-V, we evaluated the prognostic impact of IVI-guided PCI in AMI patients with high thrombus burden. A total of 4,074 patients with AMI and TIMI thrombus grades 4 or 5 who underwent aspiration thrombectomy were selected, of whom 892 patients (21.9%) received IVI-guided PCI and 3,182 patients (78.1%) received angiography-guided PCI. Primary outcome was major adverse cardiovascular event (MACE, a composite of all-cause death, MI, repeat revascularization, and stent thrombosis). Major secondary efficacy outcome was cardiac death and safety outcome was stroke at 3 years. During the median 3 years of follow-up, the risk of MACE was significantly lower in the IVI-guided PCI group than in the angiography-guided PCI group (12.9% vs 16.3%; adjusted HR, 0.80; 95% CI, 0.65 to 0.98; p = 0.035), mainly driven by a lower risk of all-cause death (5.7% vs 10.0%; adjusted HR, 0.65; 95% CI, 0.48 to 0.89; p = 0.007). IVI-guided PCI also showed lower risk of cardiac death compared with angiography-guided PCI (3.8% vs 7.0%; adjusted HR, 0.65; 95% CI, 0.44 to 0.95; p = 0.025). There was no significant difference in the risk of stroke between the groups. In this hypothesis generating study, IVI-guided PCI was associated with a lower risk of MACE and cardiac death than angiography-guided PCI in AMI patients with high thrombus burden.
01 Nov 2025INTERNATIONAL JOURNAL OF CARDIOLOGY
Duration of dual antiplatelet therapy in patients undergoing percutaneous coronary intervention for bifurcation lesions: Insights from the ULTRA-BIFURCAT registry
Article
Author: Lee, Sang Yeub ; Stefanini, Giulio ; Leone, Attilio ; Campo, Gianluca ; Sandrone, Samuele ; Choo, Eun Ho ; Park, Kyungil ; Nebiolo, Marco ; Prof, Chang-Wook Nam ; Piccolo, Raffaele ; Tuttolomondo, Domenico ; Lee, Hyun-Jong ; Kim, Hyun Kuk ; Lim, Young-Hyo ; Kang, Jeehoon ; Prof, Gaetano Maria De Ferrari ; Bruno, Francesco ; Mattesini, Alessio ; Prof, Giuseppe Patti ; D'Ascenzo, Fabrizio ; Prof, Bon-Kwon Koo ; Cortese, Bernardo ; Greco, Antonio ; Perl, Leor ; Iannaccone, Mario ; Prof, Young Bin Song ; De Filippo, Ovidio ; Choi, Ki Hong ; Cho, Yun-Kyeong ; Youn, Young Jin
BACKGROUND:
The optimal duration of dual antiplatelet therapy (DAPT) after percutaneous coronary intervention (PCI) remains debated, particularly for bifurcation lesions, which are associated with increased thrombotic risk. Shorter DAPT regimens may reduce bleeding but could compromise ischemic protection.
METHODS:
This study analyzed data from the ULTRA and BIFURCAT registries, including patients treated with PCI for bifurcation lesions. Patients requiring oral anticoagulation were excluded. DAPT duration was categorized as ≤6 months, 6-12 months and > 12 months. The primary endpoint was major adverse cardiac events (MACE), a composite of all-cause death, myocardial infarction, target lesion revascularization, and stent thrombosis. Cox regression analysis was used to assess the association between DAPT duration and MACE.
RESULTS:
Among 6729 patients, 425 (6 %) received DAPT ≤6 months, 3446 (51 %) for 6-12 months and 2858 (42 %) for >12 months. At 800-day follow-up, MACE rates were higher with shorter DAPT (19.5 % vs. 10 % vs. 5.9 %, p < 0.001). Adjusted hazard ratios for MACE were significantly higher for DAPT ≤6 months (HR 4.8, 95 % CI 1.8-12.7) and 6-12 months (HR 2.7, 95 % CI:1.5-4.7) compared to >12 months. This trend was consistent in acute coronary syndrome (ACS) patients but not in stable patients.
CONCLUSION:
In PCI-treated bifurcation lesions, particularly in ACS patients, shorter DAPT duration (≤6 months) is associated with a higher risk of adverse events. These findings, albeit hypothesis generating, highlight the need to consider bifurcation lesions as a key factor in tailoring DAPT duration and may warrant confirmation in dedicated trials.
01 Oct 2025PEDIATRIC INFECTIOUS DISEASE JOURNAL
Optimal Vancomycin AUC Target in Pediatric MRSA Bacteremia: A Bayesian-guided Approach
Article
Author: Lee, Jina ; Lee, Yonghee ; Kim, Gahee
Background::
The optimal vancomycin area under the concentration-time curve (AUC) target for pediatric methicillin-resistant Staphylococcus aures (MRSA) bacteremia remains unclear. This study aimed to determine the optimal AUC target using Bayesian software.
Methods::
A retrospective analysis was conducted on patients 3 months to 18 years of age diagnosed with MRSA bacteremia at Asan Medical Center Children`s Hospital between September 2013 and December 2021. The vancomycin AUC was estimated using Bayesian software, and the relationship between AUC24–48 and outcomes, including persistent bacteremia ≥48 hours, acute kidney injury (AKI), 30-day all-cause mortality and recurrence, was analyzed.
Results::
Fifty-six cases were included, with a median age of 2.4 years. Most cases were healthcare-associated infections (96.4%) and occurred in patients with underlying conditions (92.9%). Persistent bacteremia, recurrent bacteremia, 30-day all-cause mortality and AKI were observed in 17.9%, 14.8%, 3.7% and 7.1%, respectively. Although an AUC24–48 ≥400 mg·h/L did not demonstrate clinical benefit, the receiver operating characteristic curve analysis identified 530 mg·h/L as the appropriate AUC24–48 threshold for predicting persistent bacteremia and AKI. Persistent bacteremia and AKI were more frequent in patients with AUC24–48 >530 mg·h/L (62.5% vs. 10.4%, P < 0.01; 37.5% vs. 2.1%, P < 0.01). No significant differences in 30-day mortality or recurrence were observed between the groups with AUC24–48 above and below this threshold.
Conclusions::
AUC24–48 ≤530 mg·h/L was associated with reduced persistent bacteremia and AKI in pediatric MRSA bacteremia, without significant disadvantages in mortality and recurrence. Future research should explore the lower limit of AUC targets to optimize vancomycin therapy in pediatric patients.
11 Dec 2024

Phase 3Clinical ResultPhase 2
100 Deals associated with Chosun University Hospital
Login to view more data
100 Translational Medicine associated with Chosun University Hospital
Login to view more data
Corporation Tree
Boost your research with our corporation tree data.
login
or
Pipeline
Pipeline Snapshot as of 11 Aug 2026
The statistics for drugs in the Pipeline is the current organization and its subsidiaries are counted as organizations,Early Phase 1 is incorporated into Phase 1, Phase 1/2 is incorporated into phase 2, and phase 2/3 is incorporated into phase 3
Preclinical
6
3
Other
Login to view more data
Current Projects
Login to view more data
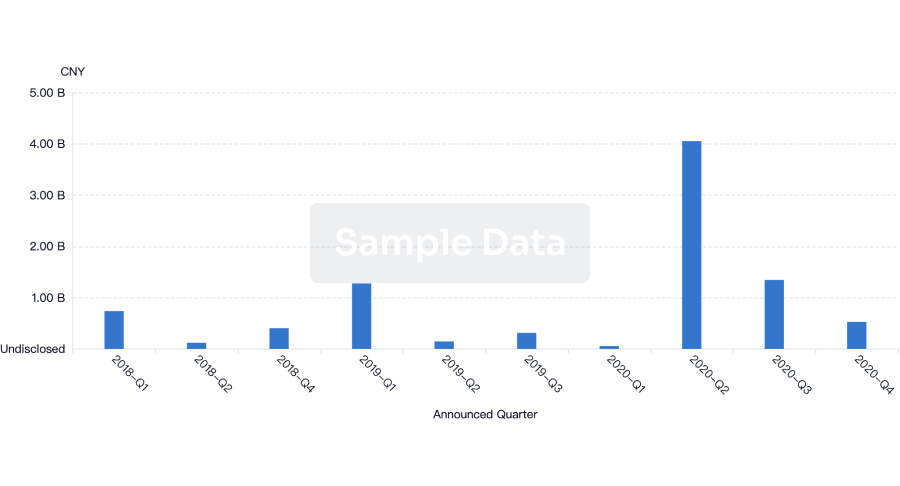
Deal
Boost your decision using our deal data.
login
or

Translational Medicine
Boost your research with our translational medicine data.
login
or

Profit
Explore the financial positions of over 360K organizations with Synapse.
login
or

Grant & Funding(NIH)
Access more than 2 million grant and funding information to elevate your research journey.
login
or

Investment
Gain insights on the latest company investments from start-ups to established corporations.
login
or

Financing
Unearth financing trends to validate and advance investment opportunities.
login
or
Hiro LS Researcher
The AI Search Engine Built to Accelerate Biopharma Decisions
Search across billion-scale life sciences data to uncover signals, validate evidence, and act with confidence.
Ask any biopharma research question→
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, Patsnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Discover Synapse Data Servers
Synapse data is now integrated into the PatSnap LS Model Context Protocol (MCP) service. Customize your LLM agent now using our MCP server!
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free