Request Demo
Last update 16 Oct 2025
Crozer-Keystone Health System
Last update 16 Oct 2025
Overview
Related
NCT04467983
Abaloparatide Added to Ongoing Denosumab vs Continued Denosumab Alone

NCT04517682
SARS -CoV-2 Detection in Saliva Samples: A Test Validation Protocol

NCT03734471
Use of a Novel Chest Tube Insertion Device for Urgent Thoracostomy in an Emergency Department Setting
100 Clinical Results associated with Crozer-Keystone Health System
Login to view more data
Login to view more data
01 Sep 2025Journal of Trauma and Acute Care Surgery
Damage control thoracotomy trends, techniques, and outcomes: An EAST multicenter trial
Article
Author: Spalding, Chance ; Puzio, Teddy ; Panagiotopoulos, Ioannis ; Maxwell, Robert ; Wang, Gerald ; Smith, Harrison ; Robinson, Bryce ; Murphy, Partick ; Mulita, Francesk ; Senekijan, Lara ; Finch, Jordan ; Sperwer, Kimberly ; Hoefer, Leah ; Favors, Lauren ; Seng, Sirivan ; Ramos, Juan ; Villalobos, Liz ; Turay, David ; Cocanour, Christine ; Gebran, Anthony ; Cromer, Dominic ; Taylor, John ; Tatebe, Leah ; Bugaev, Nikolay ; Burke, Rachel ; Hoshal, Gillian ; Cheung, Dillon ; Capron, Gweniviere ; Chang, Grace ; Ratnasekera, Asanthi ; Nahmias, Jeffry ; Powers, Taylor ; LeClair, Madison J ; Kurian, Anna ; Frederick, Nicole ; Figueroa, Juan ; Douglas, Anthony D ; Snyder, Andrew ; Goldenberg-Sandau, Anna ; Meagher, Ashley ; Dalavayi, Satya ; Bankhead, Brittany ; Liveris, Anna ; Valgardsson, Atli ; Keskey, Robert ; Kaafarani, Haytham ; Carrick, Matthew
BACKGROUND:
Damage-control thoracotomy (DCT) lacks evidence regarding frequency of use, optimal technique, and outcomes. This Eastern Association for the Surgery of Trauma multicenter trial aimed to examine DCT usage over the last decade, evaluate types of temporary closure, and assess associated outcomes.
METHODS:
An international retrospective cohort study of thoracotomies from 2008 to 2020 at 25 centers was performed. Patients age 16 years or older undergoing thoracotomy within 24 hours of admission who survived to intensive care unit (ICU) admission were included. Mixed logistic regression was used to assess complications associated with closure type, trends in DCT utilization, and mortality. Competing risk regression model was used to determine trends in ICU-free days for DCT over time.
RESULTS:
Nine hundred twenty-two thoracotomy operations were performed, of those 402 (44%) were DCT. Most injuries were penetrating (n = 609, 66%) and the most common mechanism was gunshot wound. Damage-control thoracotomy patients were significantly more injured and ill on presentation. Fifty-four percent of DCT began in the emergency department. Most common temporary closure types included skin only (n = 103, 25%), commercial vacuum device (n = 123,30%), and adhesive dressing (n = 129, 32%). Frequent complications following DCT were pneumonia (n = 57, 14%), acute renal failure (n = 53,13%), and sepsis (n = 41, 10%). Mortality rate in the DCT group was 61%, versus 17% for definitive thoracotomy (n < 0.001). Utilization of DCT has increased in a linear fashion during the study period, as well as ICU-free days out of 30 (odds ratio, 1.66; 95% confidence interval, 1.18–2.33); however, mortality has not changed over time (odds ratio, 0.61; 95% confidence interval, 0.22–1.98). After mixed logistic regression, there was no difference in complications based on closure type.
CONCLUSION:
The use of DCT is increasing over time with improved ICU-free days, but without improved mortality. Mechanism of temporary closure should be determined based on operator's experience and institutional resources.
LEVEL OF EVIDENCE:
Therapeutic/Care Management; Level III.
01 Sep 2025Cardiology in review
Sex-Specific Differences in Clinical Outcomes in Patients With Coronary Bifurcation Lesions
Review
Author: Aronow, Wilbert S. ; Sood, Akshit ; Patel, Nainesh C. ; Attar, Armin ; Gupta, Rahul ; Malik, Aaqib H. ; Frishman, William H. ; Agrawal, Ankit ; Hosseinpour, Alireza
Coronary bifurcation lesions are frequent challenging findings during percutaneous coronary intervention (PCI). Contemporary evidence has explored the potential sex-specific differences in patients undergoing PCI. In the present meta-analysis, we compared clinical outcomes of patients undergoing bifurcation PCI between women and men. Using the random-effects method, we compared the clinical outcomes of patients with a coronary bifurcation lesion following PCI between women and men. The results were reported using relative risk (RR) and 95% confidence interval (CI). Baseline comorbidities and mean age were compared between the 2 studied groups. Four observational studies comprising 30,684 patients (8898 women and 21,786 men) were included in the meta-analysis. Women were significantly older than men with a relatively higher prevalence of baseline comorbidities. After using adjusted data from 2 out of 4 available studies, performing PCI for bifurcation lesions in women was not associated with an increased risk of mortality (RR 1.33, 95% CI, 0.78–2.29), myocardial infarction (RR 1.22, 95% CI, 0.41–3.61), target lesion revascularization (RR 1.06, 95% CI, 0.40–2.81), stent thrombosis (RR 0.99, 95% CI, 0.09–10.52), and stroke (RR 1.19, 95% CI, 0.64–2.22). Women were at higher risk of major bleeding compared to male counterparts (RR 2.23, 95% CI, 1.73–2.89). The present study showed no difference in the risk of adverse clinical outcomes except the risk of bleeding between genders with coronary bifurcation lesions. Future studies with adjustment of age and baseline comorbidities are needed to confirm these findings.
01 Aug 2025Kidney360
Time Ticks Slowly for Kidney Transplant Reform
Article
Author: Hess, Gregory P.
19 Sep 2024
100 Deals associated with Crozer-Keystone Health System
Login to view more data
100 Translational Medicine associated with Crozer-Keystone Health System
Login to view more data
Corporation Tree
Boost your research with our corporation tree data.
login
or
Pipeline
Pipeline Snapshot as of 08 Nov 2025
No data posted
Login to keep update
Deal
Boost your decision using our deal data.
login
or
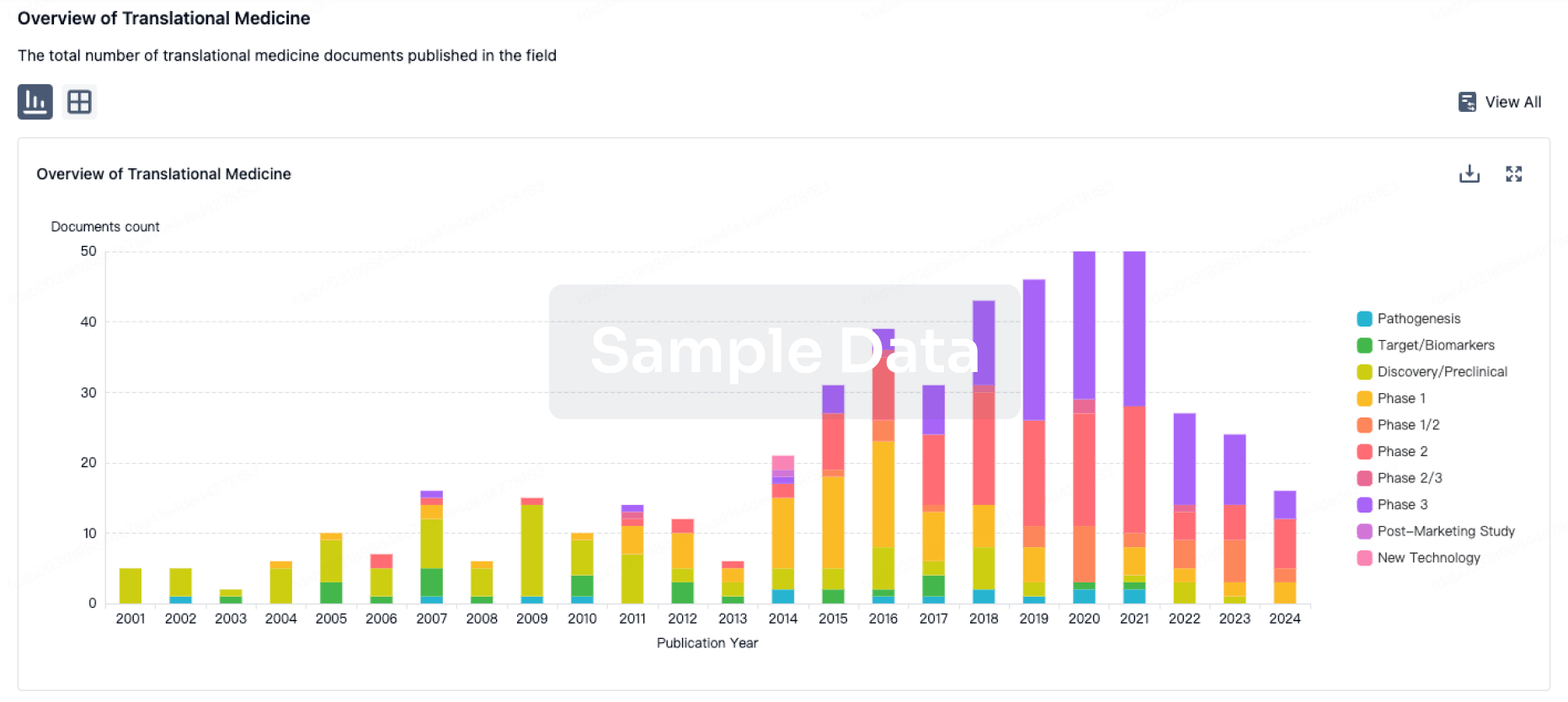
Translational Medicine
Boost your research with our translational medicine data.
login
or
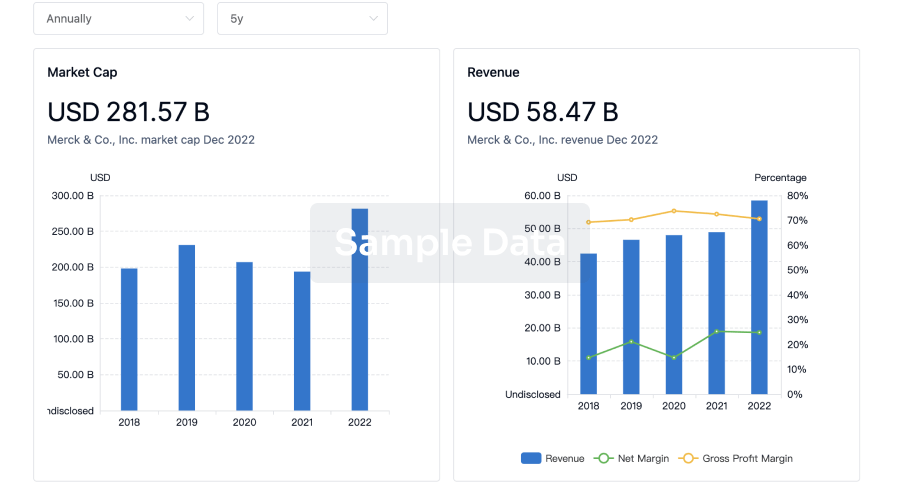
Profit
Explore the financial positions of over 360K organizations with Synapse.
login
or
Grant & Funding(NIH)
Access more than 2 million grant and funding information to elevate your research journey.
login
or

Investment
Gain insights on the latest company investments from start-ups to established corporations.
login
or
Financing
Unearth financing trends to validate and advance investment opportunities.
login
or
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free