Request Demo
What is Axicabtagene Ciloleucel used for?
14 June 2024
Axicabtagene Ciloleucel, commercially known as Yescarta, is a groundbreaking therapy in the field of oncology, particularly for the treatment of certain types of aggressive B-cell lymphoma. This advanced therapeutic option falls under the category of chimeric antigen receptor (CAR) T-cell therapies. Developed by Kite Pharma, a subsidiary of Gilead Sciences, it has brought new hope to patients who have exhausted other treatment options. The primary target of Axicabtagene Ciloleucel is the CD19 antigen, which is commonly expressed on the surface of B-cell malignancies. It is specifically indicated for adult patients with relapsed or refractory large B-cell lymphoma after two or more lines of systemic therapy. As of its latest updates, Axicabtagene Ciloleucel has received approval from major regulatory bodies such as the FDA and EMA and continues to be the subject of ongoing research and clinical trials to explore its efficacy and safety in other hematological malignancies.
The mechanism of action for Axicabtagene Ciloleucel involves genetic reprogramming of a patient’s own T-cells to target and attack cancer cells. Here's how it works: T-cells are collected from the patient through a process called leukapheresis. These T-cells are then genetically modified in a laboratory setting to express a CAR that specifically binds to the CD19 antigen on the surface of B-cells. Once these engineered CAR T-cells are infused back into the patient’s bloodstream, they seek out and bind to CD19-expressing cells, which include malignant B-cells. Upon binding, the CAR T-cells become activated and induce the destruction of the cancer cells through cytotoxic mechanisms. This process not only targets and kills the cancer cells but also persists in the body to provide ongoing surveillance against the recurrence of the malignancy.
The administration of Axicabtagene Ciloleucel involves several carefully coordinated steps to ensure safety and efficacy. Initially, the patient undergoes leukapheresis to collect T-cells. These cells are then sent to a specialized facility for genetic modification and expansion. The entire manufacturing process can take a few weeks. Prior to the infusion of the modified CAR T-cells, the patient typically receives a short course of lymphodepleting chemotherapy to enhance the expansion and function of the infused CAR T-cells. The engineered T-cells are then administered as a one-time intravenous infusion. The onset of action can be quite rapid, with some patients experiencing a reduction in tumor burden within days to weeks. However, it is essential for patients to remain under close medical supervision for several weeks post-infusion to monitor for potential adverse reactions and to manage any complications that may arise.
While Axicabtagene Ciloleucel has shown remarkable efficacy, it is also associated with some significant side effects and contraindications. The most notable side effects include cytokine release syndrome (CRS) and neurological toxicities, both of which can be severe and life-threatening. CRS is a systemic inflammatory response that can cause fever, hypotension, and multi-organ dysfunction. Neurological toxicities can manifest as confusion, seizures, or encephalopathy. Other potential side effects include cytopenias, infections, and hypogammaglobulinemia. Due to these risks, Axicabtagene Ciloleucel is typically administered in a specialized healthcare setting where patients can be closely monitored and managed. Contraindications include active infections, uncontrolled autoimmune diseases, and certain cardiovascular conditions, as the therapy can exacerbate these conditions. It is also contraindicated in patients who are pregnant or breastfeeding due to the potential risks to the fetus or infant.
The interaction of Axicabtagene Ciloleucel with other drugs is an important consideration in the management of patients undergoing this therapy. Immunosuppressive agents can interfere with the expansion and activity of CAR T-cells, potentially reducing the efficacy of the treatment. Patients are usually advised to avoid corticosteroids and other immunosuppressive drugs before and after the infusion, unless absolutely necessary for the management of severe side effects like CRS. Additionally, the use of certain antiviral and antifungal medications may be necessary to prevent infections due to the immunosuppressed state induced by both the lymphodepleting chemotherapy and the CAR T-cell therapy itself. However, these agents should be selected and managed cautiously to avoid interactions that could compromise the patient's immune function or the efficacy of the CAR T-cells.
In conclusion, Axicabtagene Ciloleucel represents a significant advancement in the treatment of refractory B-cell lymphomas, offering new hope for patients with few remaining options. While it brings the promise of durable responses and potential cures, it also necessitates careful patient selection, meticulous management of side effects, and a thorough understanding of drug interactions. As research continues, it is hoped that the indications for Axicabtagene Ciloleucel will expand, and strategies to mitigate its risks will be further refined, making this innovative therapy accessible to a broader range of patients.
The mechanism of action for Axicabtagene Ciloleucel involves genetic reprogramming of a patient’s own T-cells to target and attack cancer cells. Here's how it works: T-cells are collected from the patient through a process called leukapheresis. These T-cells are then genetically modified in a laboratory setting to express a CAR that specifically binds to the CD19 antigen on the surface of B-cells. Once these engineered CAR T-cells are infused back into the patient’s bloodstream, they seek out and bind to CD19-expressing cells, which include malignant B-cells. Upon binding, the CAR T-cells become activated and induce the destruction of the cancer cells through cytotoxic mechanisms. This process not only targets and kills the cancer cells but also persists in the body to provide ongoing surveillance against the recurrence of the malignancy.
The administration of Axicabtagene Ciloleucel involves several carefully coordinated steps to ensure safety and efficacy. Initially, the patient undergoes leukapheresis to collect T-cells. These cells are then sent to a specialized facility for genetic modification and expansion. The entire manufacturing process can take a few weeks. Prior to the infusion of the modified CAR T-cells, the patient typically receives a short course of lymphodepleting chemotherapy to enhance the expansion and function of the infused CAR T-cells. The engineered T-cells are then administered as a one-time intravenous infusion. The onset of action can be quite rapid, with some patients experiencing a reduction in tumor burden within days to weeks. However, it is essential for patients to remain under close medical supervision for several weeks post-infusion to monitor for potential adverse reactions and to manage any complications that may arise.
While Axicabtagene Ciloleucel has shown remarkable efficacy, it is also associated with some significant side effects and contraindications. The most notable side effects include cytokine release syndrome (CRS) and neurological toxicities, both of which can be severe and life-threatening. CRS is a systemic inflammatory response that can cause fever, hypotension, and multi-organ dysfunction. Neurological toxicities can manifest as confusion, seizures, or encephalopathy. Other potential side effects include cytopenias, infections, and hypogammaglobulinemia. Due to these risks, Axicabtagene Ciloleucel is typically administered in a specialized healthcare setting where patients can be closely monitored and managed. Contraindications include active infections, uncontrolled autoimmune diseases, and certain cardiovascular conditions, as the therapy can exacerbate these conditions. It is also contraindicated in patients who are pregnant or breastfeeding due to the potential risks to the fetus or infant.
The interaction of Axicabtagene Ciloleucel with other drugs is an important consideration in the management of patients undergoing this therapy. Immunosuppressive agents can interfere with the expansion and activity of CAR T-cells, potentially reducing the efficacy of the treatment. Patients are usually advised to avoid corticosteroids and other immunosuppressive drugs before and after the infusion, unless absolutely necessary for the management of severe side effects like CRS. Additionally, the use of certain antiviral and antifungal medications may be necessary to prevent infections due to the immunosuppressed state induced by both the lymphodepleting chemotherapy and the CAR T-cell therapy itself. However, these agents should be selected and managed cautiously to avoid interactions that could compromise the patient's immune function or the efficacy of the CAR T-cells.
In conclusion, Axicabtagene Ciloleucel represents a significant advancement in the treatment of refractory B-cell lymphomas, offering new hope for patients with few remaining options. While it brings the promise of durable responses and potential cures, it also necessitates careful patient selection, meticulous management of side effects, and a thorough understanding of drug interactions. As research continues, it is hoped that the indications for Axicabtagene Ciloleucel will expand, and strategies to mitigate its risks will be further refined, making this innovative therapy accessible to a broader range of patients.
How to obtain the latest development progress of all drugs?
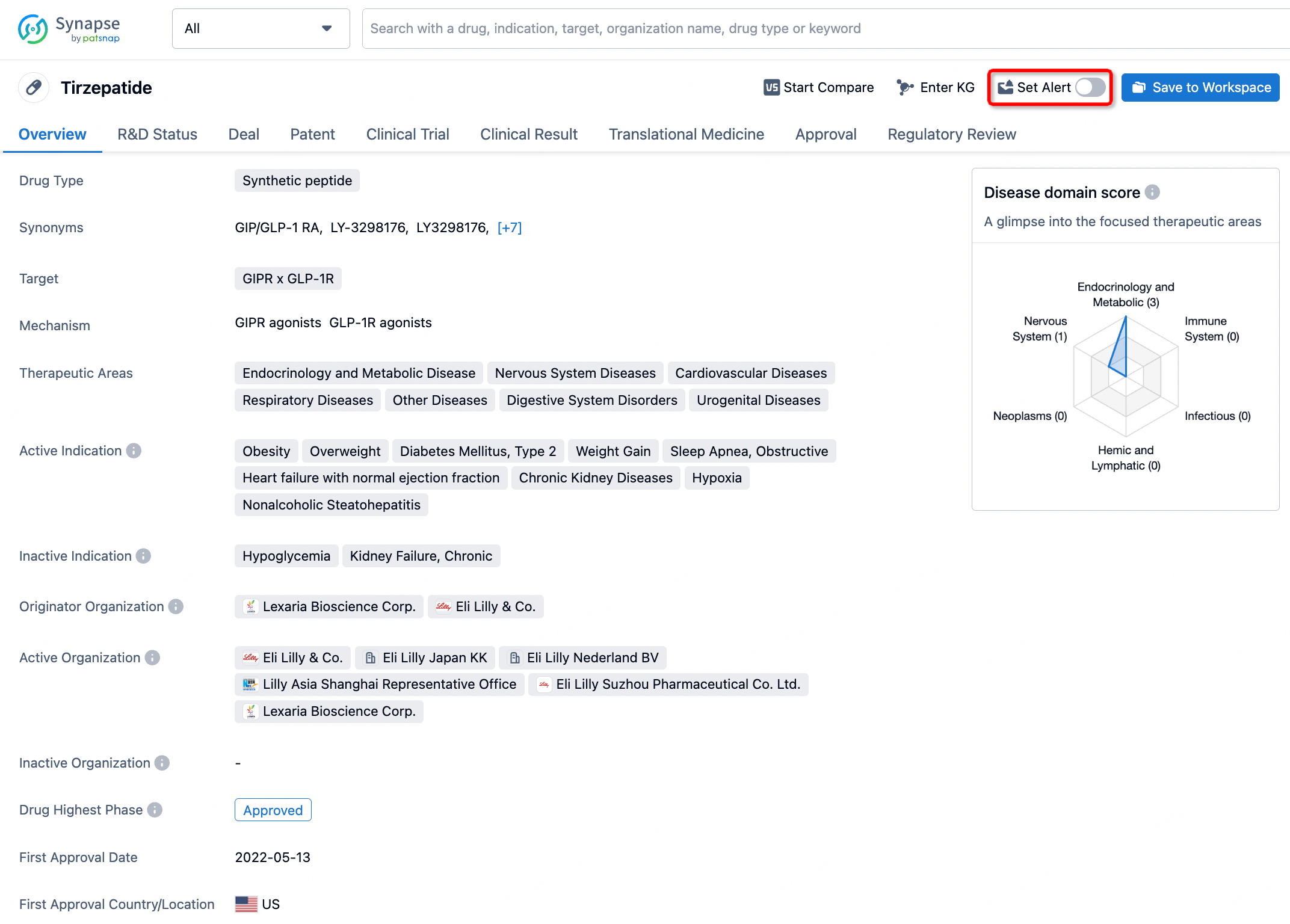
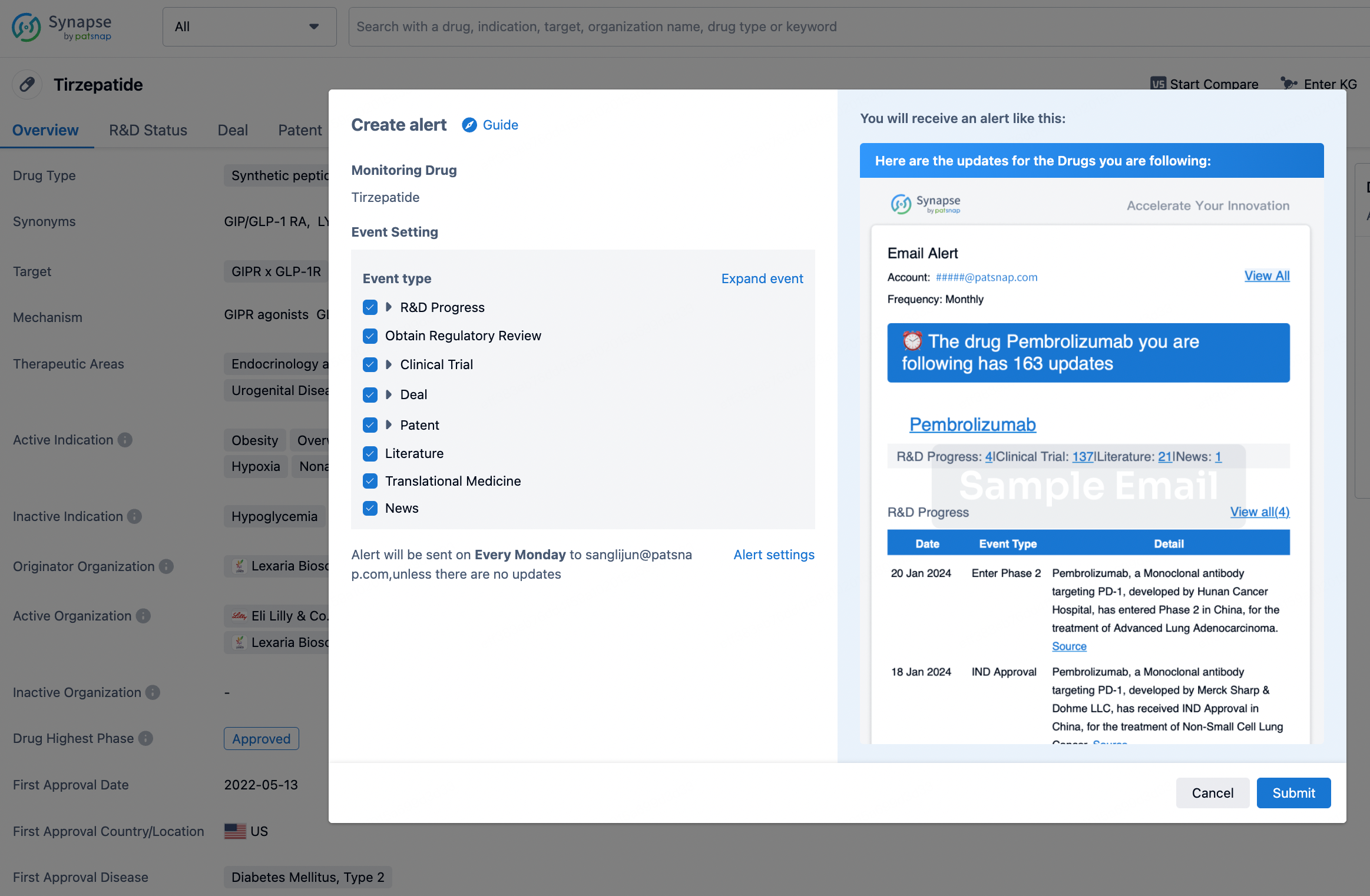
In the Synapse database, you can stay updated on the latest research and development advances of all drugs. This service is accessible anytime and anywhere, with updates available daily or weekly. Use the "Set Alert" function to stay informed. Click on the image below to embark on a brand new journey of drug discovery!
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.