Request Demo
What is the mechanism of Levobunolol Hydrochloride?
17 July 2024
Levobunolol hydrochloride is a non-selective beta-adrenergic antagonist utilized primarily in the management of elevated intraocular pressure, commonly associated with conditions such as glaucoma. Understanding its mechanism of action is essential for comprehending how it effectively reduces intraocular pressure and minimizes the risk of optic nerve damage.
At the core of its mechanism, levobunolol hydrochloride works by inhibiting the action of catecholamines—primarily adrenaline and noradrenaline—on beta-adrenergic receptors. These receptors are present throughout various tissues in the body, including the heart, lungs, and eyes. Levobunolol hydrochloride is non-selective, meaning it blocks both beta-1 and beta-2 receptors.
In the context of ophthalmology, the primary action occurs within the eye. The ocular beta receptors, when stimulated by catecholamines, lead to increased production of aqueous humor, the fluid that maintains intraocular pressure. By blocking these receptors, levobunolol hydrochloride reduces aqueous humor production, thereby lowering the intraocular pressure. This reduction in pressure can help prevent or slow the progression of glaucomatous optic neuropathy, which can ultimately lead to vision loss if left untreated.
Another aspect of levobunolol hydrochloride’s mechanism involves a slight increase in the outflow of aqueous humor through the trabecular meshwork. Although this is a secondary action, it complements the primary mechanism of reducing aqueous humor production, thus contributing to an overall decrease in intraocular pressure.
The systemic absorption of levobunolol hydrochloride, though minimal when applied topically, can have additional effects due to its non-selective beta-blocking properties. For instance, it can influence cardiovascular and respiratory functions by reducing heart rate and contractility and potentially causing bronchoconstriction. Therefore, its use is contraindicated or requires caution in patients with conditions such as asthma, chronic obstructive pulmonary disease (COPD), and certain cardiac disorders.
Pharmacokinetically, levobunolol hydrochloride demonstrates a rapid onset of action, typically within an hour of administration, with the peak effect occurring within 2 to 6 hours. Its duration of action can last up to 24 hours, making it convenient for once or twice daily dosing. The drug is metabolized primarily in the liver, and its metabolites are excreted via the kidneys.
One must also consider potential side effects, which may arise from both systemic absorption and localized ocular effects. Common ocular side effects include transient stinging or discomfort upon instillation, dryness, and a potential for allergic reactions. Systemic side effects, although rare, can include bradycardia, hypotension, and bronchospasm due to its beta-blocking activity.
In conclusion, levobunolol hydrochloride operates by inhibiting beta-adrenergic receptors, leading to decreased aqueous humor production and, to a lesser extent, increased aqueous humor outflow. This dual mechanism effectively lowers intraocular pressure, making it a valuable option in the treatment of glaucoma. However, its non-selective nature necessitates careful consideration of potential systemic effects, especially in patients with preexisting cardiovascular or respiratory conditions. Understanding these mechanisms and precautions is vital for the safe and effective use of levobunolol hydrochloride in clinical practice.
At the core of its mechanism, levobunolol hydrochloride works by inhibiting the action of catecholamines—primarily adrenaline and noradrenaline—on beta-adrenergic receptors. These receptors are present throughout various tissues in the body, including the heart, lungs, and eyes. Levobunolol hydrochloride is non-selective, meaning it blocks both beta-1 and beta-2 receptors.
In the context of ophthalmology, the primary action occurs within the eye. The ocular beta receptors, when stimulated by catecholamines, lead to increased production of aqueous humor, the fluid that maintains intraocular pressure. By blocking these receptors, levobunolol hydrochloride reduces aqueous humor production, thereby lowering the intraocular pressure. This reduction in pressure can help prevent or slow the progression of glaucomatous optic neuropathy, which can ultimately lead to vision loss if left untreated.
Another aspect of levobunolol hydrochloride’s mechanism involves a slight increase in the outflow of aqueous humor through the trabecular meshwork. Although this is a secondary action, it complements the primary mechanism of reducing aqueous humor production, thus contributing to an overall decrease in intraocular pressure.
The systemic absorption of levobunolol hydrochloride, though minimal when applied topically, can have additional effects due to its non-selective beta-blocking properties. For instance, it can influence cardiovascular and respiratory functions by reducing heart rate and contractility and potentially causing bronchoconstriction. Therefore, its use is contraindicated or requires caution in patients with conditions such as asthma, chronic obstructive pulmonary disease (COPD), and certain cardiac disorders.
Pharmacokinetically, levobunolol hydrochloride demonstrates a rapid onset of action, typically within an hour of administration, with the peak effect occurring within 2 to 6 hours. Its duration of action can last up to 24 hours, making it convenient for once or twice daily dosing. The drug is metabolized primarily in the liver, and its metabolites are excreted via the kidneys.
One must also consider potential side effects, which may arise from both systemic absorption and localized ocular effects. Common ocular side effects include transient stinging or discomfort upon instillation, dryness, and a potential for allergic reactions. Systemic side effects, although rare, can include bradycardia, hypotension, and bronchospasm due to its beta-blocking activity.
In conclusion, levobunolol hydrochloride operates by inhibiting beta-adrenergic receptors, leading to decreased aqueous humor production and, to a lesser extent, increased aqueous humor outflow. This dual mechanism effectively lowers intraocular pressure, making it a valuable option in the treatment of glaucoma. However, its non-selective nature necessitates careful consideration of potential systemic effects, especially in patients with preexisting cardiovascular or respiratory conditions. Understanding these mechanisms and precautions is vital for the safe and effective use of levobunolol hydrochloride in clinical practice.
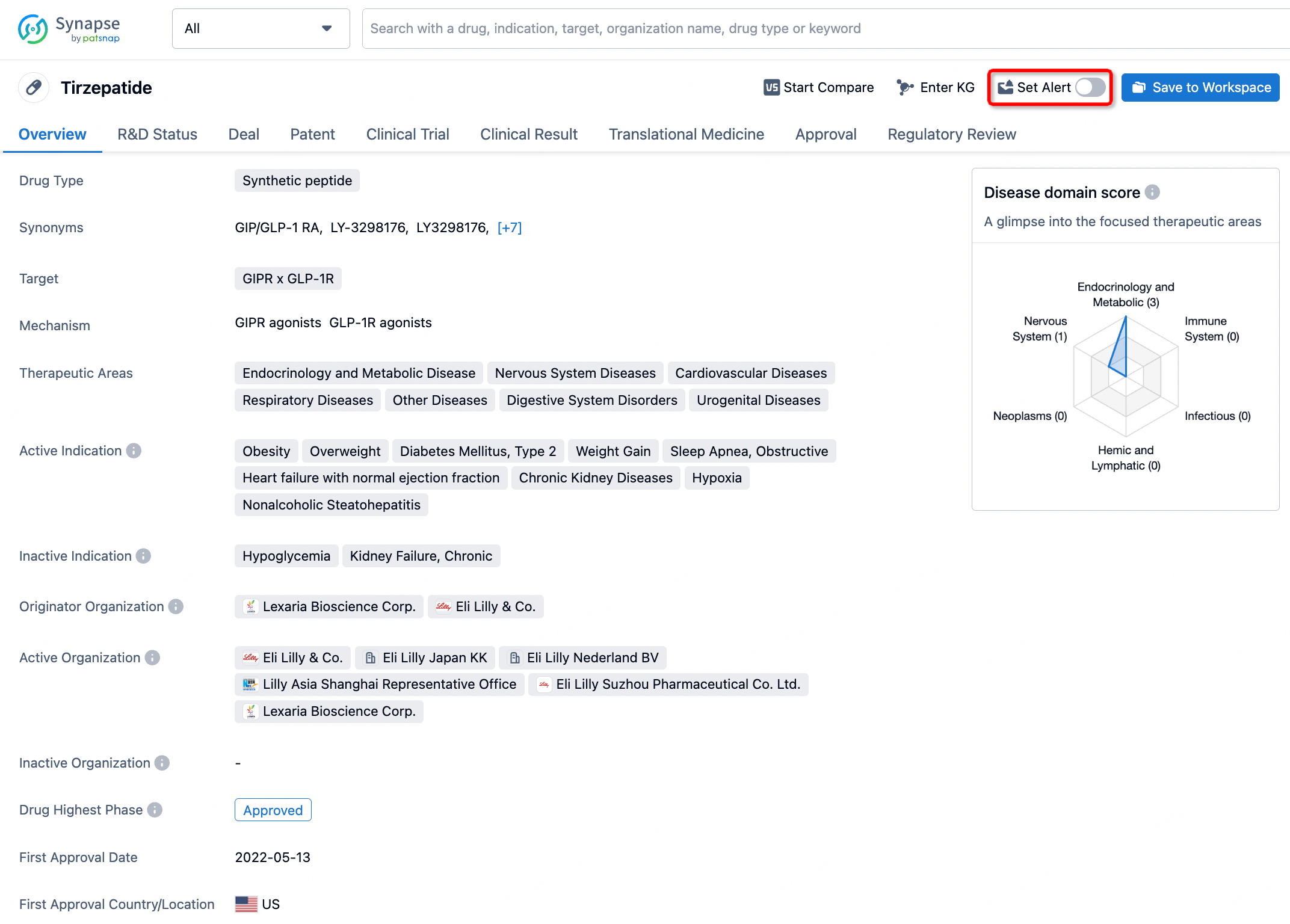
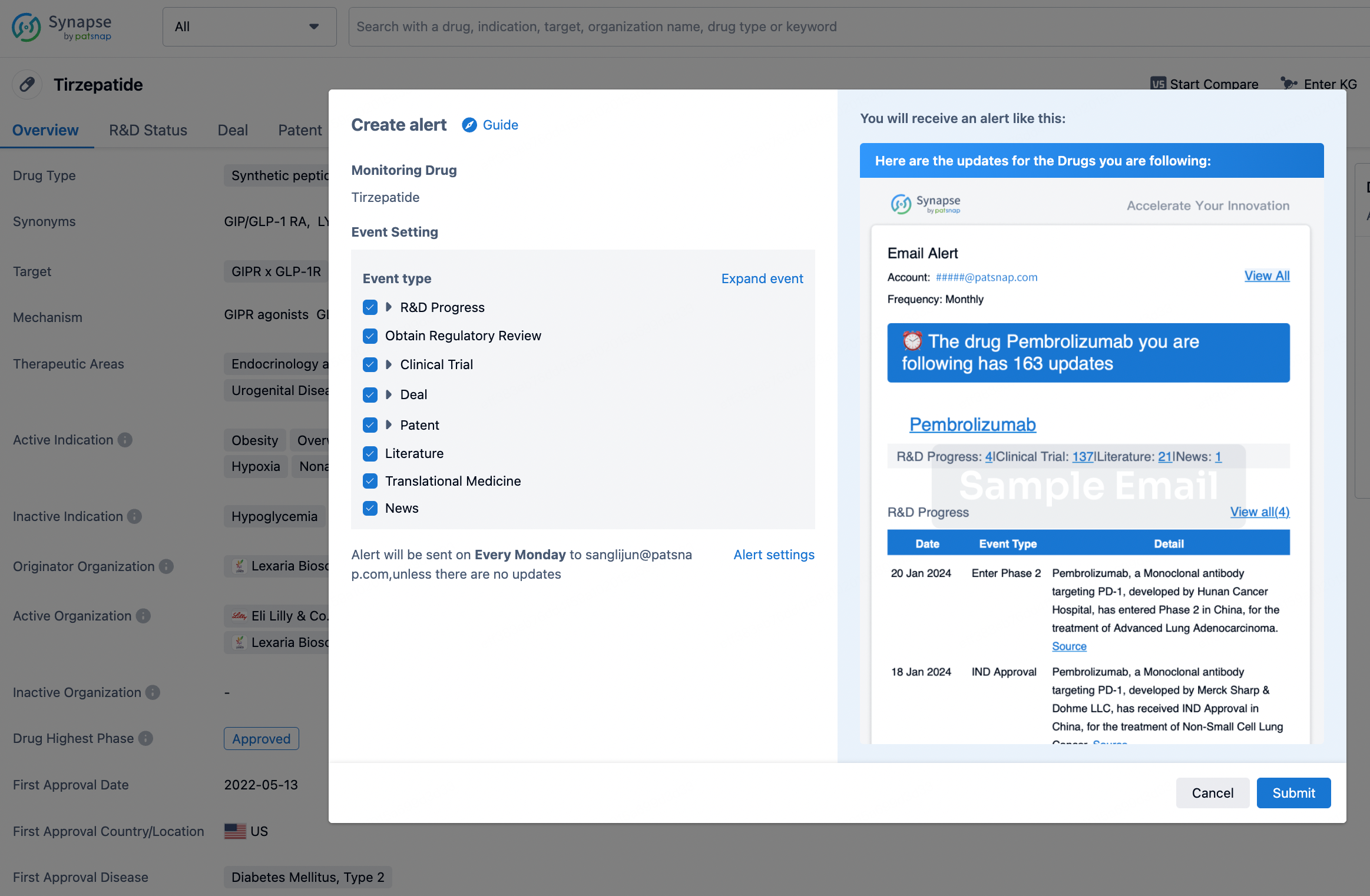
How to obtain the latest development progress of all drugs?
In the Synapse database, you can stay updated on the latest research and development advances of all drugs. This service is accessible anytime and anywhere, with updates available daily or weekly. Use the "Set Alert" function to stay informed. Click on the image below to embark on a brand new journey of drug discovery!
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.