Request Demo
Last update 31 Jul 2026
Lenalidomide
Last update 31 Jul 2026
Overview
Basic Info
Drug Type Degradable Molecular Glue |
Synonyms 1-oxo-2-(2,6-dioxopiperidin-3-yl)-4-aminoisoindoline, 3-(4-Amino-1-oxoisoindolin-2-yl)piperidine-2,6-dione, CMIO-LLD + [18] |
Action inhibitors, modulators, degraders |
Mechanism CK1α inhibitors(casein kinase 1 alpha 1 inhibitors), CRBN modulators(Cereblon modulators), IKZF1 degraders(DNA-binding protein Ikaros degraders) |
Therapeutic Areas |
Active Indication |
Inactive Indication |
Originator Organization |
Active Organization |
Inactive Organization |
License Organization |
Drug Highest PhaseApproved |
First Approval Date United States (27 Dec 2005), |
RegulationOrphan Drug (United States), Special Review Project (China), Orphan Drug (Japan), Priority Review (China) |







Login to view timeline
Structure/Sequence
Molecular FormulaC13H13N3O3 |
InChIKeyGOTYRUGSSMKFNF-UHFFFAOYSA-N |
CAS Registry191732-72-6 |
Related
1,333
Clinical Trials associated with LenalidomideNCT07600151
A Clinical Phase I/II, Multicenter, Open-label, National Study Evaluating Quintuplet Treat-ment With ISaTuximab, Bortezomib, Lenalidomide and Dexamethasone Plus Etentamig (Etenta-Isa-VRd) in Primary DiagnOsed High-Risk Multiple Myeloma Patients

NCT07735637
A Phase III, Open-label, Multicentre, Randomised Study Comparing Consolidation Treatment With AZD0120, an Autologous Dual Targeting Chimeric Antigen Receptor T-cell (CAR-T) Therapy Directed Against BCMA and CD19, Versus Autologous Stem Cell Transplant (ASCT) in Participants With Newly Diagnosed Multiple Myeloma Who Are Transplant Eligible (TE NDMM) (DURGA-6)

NCT07719543
A Phase III Multicenter Randomized Double-Blind Placebo-Controlled Study Evaluating the Efficacy and Safety of Lenalidomide in Patients With IgG4-Related Disease
100 Clinical Results associated with Lenalidomide
Login to view more data
100 Translational Medicine associated with Lenalidomide
Login to view more data
100 Patents (Medical) associated with Lenalidomide
Login to view more data
7,783
Literatures (Medical) associated with Lenalidomide31 Dec 2026Hematology
Secondary poor graft function after autologous stem cell transplantation in multiple myeloma: a case-based expert review and successful rescue with secondary autologous stem cell infusion
Review
Author: Song, Xiaoning ; Liu, Xiaojun ; Suo, Jing ; Lu, Jiapei ; Meng, Yuan ; Meng, Jianbo ; Zhang, Jinqiao ; You, Jiawen ; Zhang, Yuanyuan ; Dai, Yuxin ; Zang, Meirong
INTRODUCTION:
Secondary poor graft function (PGF) after autologous hematopoietic stem cell transplantation (Auto-HSCT) for multiple myeloma (MM) is rare, often delayed in recognition, and lacks standardized salvage algorithms.
AREAS COVERED:
Using a case-based expert-review format, we summarize diagnostic hallmarks, exclusion work-up, mechanistic drivers, and practical management, with emphasis on autologous stem-cell boost as a rescue option.
CASE SUMMARY:
A 59-year-old woman with IgG κ MM achieved timely neutrophil and platelet engraftment after Auto-HSCT, then developed recurrent transfusion-dependent pancytopenia approximately two months later. Relapse, occult infection/viral reactivation, immune cytopenia, nutritional deficiency, and drug-related myelosuppression were systematically excluded, supporting secondary PGF. Growth factors and thrombopoietin-receptor agonists produced only transient benefit. A second infusion of cryopreserved autologous peripheral blood stem cells (PBSCs) (3.621 × 106 CD34+/kg) without re-conditioning led to rapid platelet recovery within 7 days and durable trilineage hematopoiesis.
EXPERT OPINION:
Secondary PGF after Auto-HSCT appears multifactorial, involving quantitatively adequate but qualitatively fragile grafts, inflammatory/microenvironmental injury, and therapy-related megakaryocytic vulnerability (including heavy lenalidomide exposure). When backup cells are available and reversible causes are excluded, early unpreconditioned autologous PBSC boost is a safe, feasible, and likely under-utilized salvage strategy. Strategic PBSC banking and early recognition may prevent life-threatening PGF.
31 Dec 2026JOURNAL OF MEDICAL ECONOMICS
Indirect treatment comparison of DVRd plus DR maintenance (PERSEUS study) versus DVTd or VTd with or without lenalidomide maintenance in transplant-eligible patients with previously untreated multiple myeloma
Article
Author: Einsele, Hermann ; Facon, Thierry ; Nair, Sandhya ; Dimopoulos, Meletios A. ; He, Jianming ; Caillot, Denis ; Sonneveld, Pieter ; Zweegman, Sonja ; Ammann, Eric ; Spencer, Andrew ; Nobrega, Marjorie ; Broijl, Annemiek ; Perrot, Aurore ; Schjesvold, Fredrik ; Gay, Francesca ; Boccadoro, Mario ; Hajek, Roman ; Rodriguez-Otero, Paula ; Hulin, Cyrille ; Sitthi-Amorn, Anna ; Rowe, Melissa ; Leleu, Xavier ; Mina, Roberto
AIMS:
To compare the effectiveness of induction and consolidation with daratumumab, bortezomib, lenalidomide, and dexamethasone (DVRd) plus maintenance therapy with daratumumab and lenalidomide (DR) with 2 treatment regimens that are widely used for transplant-eligible newly diagnosed multiple myeloma (TE NDMM): bortezomib, thalidomide, and dexamethasone (VTd) or daratumumab-VTd (DVTd) followed by observation (Obs) or lenalidomide maintenance.
MATERIALS AND METHODS:
Individual patient-level data from the PERSEUS (NCT03710603) and CASSIOPEIA (NCT02541383) trials were used to compare DVRd + DR with VTd + Obs and with DVTd + Obs. Inverse probability of treatment weighting was used to adjust for differences in baseline patient characteristics between the two trials; inverse probability of censoring weighting was used to adjust for the second randomization of CASSIOPEIA. Data from the CASSIOPEIA and Myeloma XI (EudraCT 2009-010956-93) trials were combined to model outcomes associated with lenalidomide (R) maintenance following induction with DVTd or VTd.
RESULTS:
DVRd + DR showed superior progression-free survival compared with DVTd + Obs (hazard ratio, 0.39 [95% CI = 0.26-0.59]), VTd + Obs (0.17 [95% CI = 0.12-0.25]), DVTd + R (0.62 [95% CI = 0.41-0.92]), and VTd + R (0.29 [95% CI = 0.18-0.43]). Sensitivity analyses showed results were consistent with the base case.
LIMITATIONS:
The indirect treatment comparison was unanchored due to a lack of common comparators and relied on external data from the Myeloma XI trial to model outcomes associated with DVTd or VTd followed by R maintenance. Despite best efforts to identify and adjust for important treatment effect modifiers, there is a potential for residual confounding.
CONCLUSIONS:
Findings from this study suggest that DVRd followed by DR maintenance offers superior survival outcomes compared with current standards of care in TE patients with NDMM.
31 Dec 2026Hematology
Neutrophil extracellular trap-related genes in PTCL: identification, prognosis and drug interaction prediction via bioinformatics-machine learning
Article
Author: Chen, Jing ; Cheng, Fanjun ; Fang, Jun
OBJECTIVE:
This study aimed to identify neutrophil extracellular trap-related genes (NET-RGs), explore their prognostic significance, and predict drug interactions in peripheral T-cell lymphoma (PTCL).
METHODS:
Differentially expressed NET-RGs (DE-NRGs) between PTCL and normal tissues were screened. Functional enrichment analysis was conducted. Bioinformatics and machine learning were used to identify hub genes and assess their diagnostic value. Univariate and multivariate analyses were used to evaluate prognostic roles. Correlation and immune infiltration analyses were performed to explore relationships with the tumor microenvironment (TME). Clinical data were collected from PTCL patients who received potential agents (lenalidomide) as first-line treatment.
RESULTS:
A total of 31 DE-NRGs were identified (18 upregulated and 13 downregulated), enriched in inflammatory response, extracellular matrix organization, and infection involvement. Four hub genes (AKT2, MAPK14, IRF1, and TNF) were identified as effective PTCL diagnostic markers. Higher AKT2/MAPK14 expression correlated with poorer overall survival (OS), while elevated TNF expression associated with better OS; AKT2 and TNF independently predicted OS. These genes were implicated in modulating TME remodeling. Potential therapeutic agents (e.g. capivasertib, lenalidomide) were predicted, and lenalidomide may represent a feasible initial treatment option for PTCL, with an objective response rate (ORR) of 40.0% and a maximum survival duration exceeding 50 months.
CONCLUSION:
NET-RGs play crucial roles in diagnosis, prognosis, and TME regulation, and lenalidomide, a putative TNF-targeting agent, may represent a feasible initial treatment option in PTCL.
1,201
News (Medical) associated with Lenalidomide31 Jul 2026
Clinical ResultDrug ApprovalPhase 3AcquisitionFinancial Statement
30 Jul 2026
Phase 3Financial Statement
30 Jul 2026
Phase 1Phase 3Clinical ResultPhase 2License out/in
100 Deals associated with Lenalidomide
Login to view more data
External Link
| KEGG | Wiki | ATC | Drug Bank |
|---|---|---|---|
| D04687 | Lenalidomide |
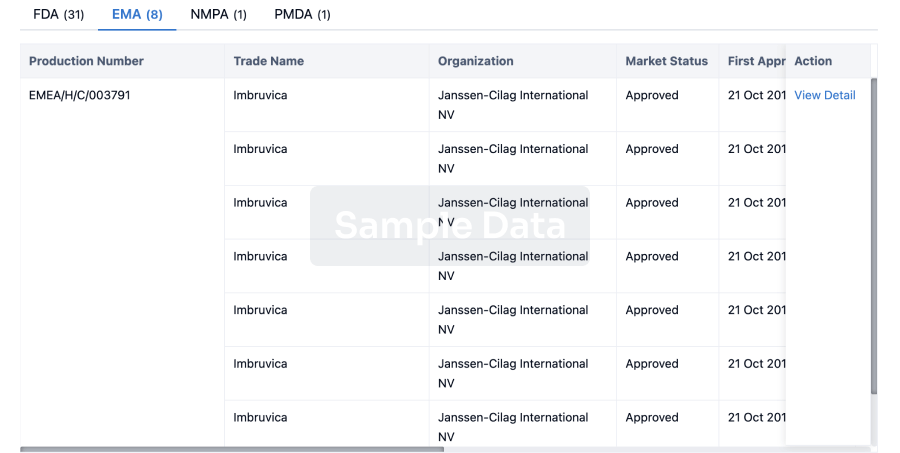
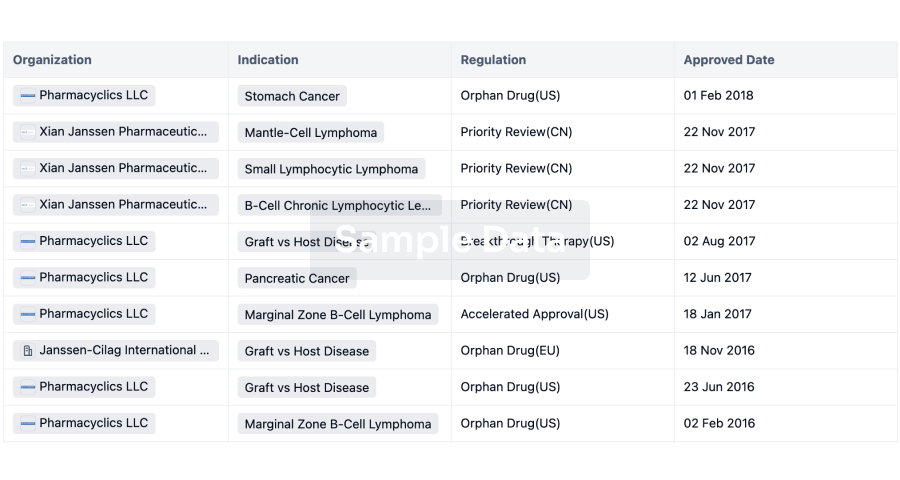
R&D Status
Approved
10 top approved records. to view more data
Login
| Indication | Country/Location | Organization | Date |
|---|---|---|---|
| Large B-cell lymphoma | United States | 11 Feb 2025 | |
| Marginal Zone B-Cell Lymphoma | United States | 28 May 2019 | |
| Adult T-Cell Leukemia-Lymphoma | Japan | 02 Mar 2017 | |
| Chromosome 5q Deletion Syndrome | European Union | 14 Jun 2007 | |
| Chromosome 5q Deletion Syndrome | Iceland | 14 Jun 2007 | |
| Chromosome 5q Deletion Syndrome | Liechtenstein | 14 Jun 2007 | |
| Chromosome 5q Deletion Syndrome | Norway | 14 Jun 2007 | |
| Follicular Lymphoma | European Union | 14 Jun 2007 | |
| Follicular Lymphoma | Iceland | 14 Jun 2007 | |
| Follicular Lymphoma | Liechtenstein | 14 Jun 2007 | |
| Follicular Lymphoma | Norway | 14 Jun 2007 | |
| Mantle-Cell Lymphoma | European Union | 14 Jun 2007 | |
| Mantle-Cell Lymphoma | Iceland | 14 Jun 2007 | |
| Mantle-Cell Lymphoma | Liechtenstein | 14 Jun 2007 | |
| Mantle-Cell Lymphoma | Norway | 14 Jun 2007 | |
| Transfusion dependent anaemia | European Union | 14 Jun 2007 | |
| Transfusion dependent anaemia | Iceland | 14 Jun 2007 | |
| Transfusion dependent anaemia | Liechtenstein | 14 Jun 2007 | |
| Transfusion dependent anaemia | Norway | 14 Jun 2007 | |
| Multiple Myeloma | United States | 29 Jun 2006 |

Developing
10 top R&D records. to view more data
Login
| Indication | Highest Phase | Country/Location | Organization | Date |
|---|---|---|---|---|
| T-cell/histiocyte rich large B-cell lymphoma | Phase 3 | United States | 11 May 2021 | |
| T-cell/histiocyte rich large B-cell lymphoma | Phase 3 | Japan | 11 May 2021 | |
| T-cell/histiocyte rich large B-cell lymphoma | Phase 3 | Argentina | 11 May 2021 | |
| T-cell/histiocyte rich large B-cell lymphoma | Phase 3 | Australia | 11 May 2021 | |
| T-cell/histiocyte rich large B-cell lymphoma | Phase 3 | Austria | 11 May 2021 | |
| T-cell/histiocyte rich large B-cell lymphoma | Phase 3 | Canada | 11 May 2021 | |
| T-cell/histiocyte rich large B-cell lymphoma | Phase 3 | Colombia | 11 May 2021 | |
| T-cell/histiocyte rich large B-cell lymphoma | Phase 3 | Czechia | 11 May 2021 | |
| T-cell/histiocyte rich large B-cell lymphoma | Phase 3 | France | 11 May 2021 | |
| T-cell/histiocyte rich large B-cell lymphoma | Phase 3 | Germany | 11 May 2021 |
Login to view more data
Clinical Result
Clinical Result
Indication
Phase
Evaluation
View All Results
Phase 2 | 28 | vmvcpdgegk = dsruuypbvo mxwumqrmon (rohnibxrtc, tcfoqhidog - zhahrfamoi) View more | - | 02 Jul 2026 | |||
Phase 3 | 11 | (Ixazomib + Lenalidomide + Dexamethasone + Zoledronic Acid) | bjhxonpwzx = nmiypprduc ahmzhmctbh (iorxclsvzl, tonszmpdfi - peqnbncntn) View more | - | 30 Jun 2026 | ||
(Zoledronic Acid) | bjhxonpwzx = bjrqxajxay ahmzhmctbh (iorxclsvzl, kmrizstvqo - yfssrxxptk) View more | ||||||
Not Applicable | - | 27 | atkdeandcw(wzqaqueaoz) = pznvdmgasg zrchyzqgym (gtjiktyyxc ) View more | Positive | 11 Jun 2026 | ||
Phase 1 | 66 | roisrudkkv(ssyyqofogw) = xmlrhxuadv gzpqzdjtty (jwgtzqzxum ) View more | Positive | 09 Jun 2026 | |||
Not Applicable | - | 3,328 | dxdbhxfjzt(lnlmbfidiz) = vthfmaakui zsrkeqehxe (zeyfjlbiec ) View more | Positive | 29 May 2026 | ||
Phase 1/2 | Multiple Myeloma First line | 36 | sldegjsipf(tqriwjtntx) = zyxnpwrbpd ofiqlawjpp (ccysuwsshj ) View more | Positive | 29 May 2026 | ||
Not Applicable | 127 | (Lenalidomide-induced eosinophilia) | jjvncljzvs(kkfhynhqlb) = edezorprgy gyeryoxwhz (sejccmoirj ) View more | Positive | 29 May 2026 | ||
(No Lenalidomide-induced eosinophilia) | jjvncljzvs(kkfhynhqlb) = yseohhoith gyeryoxwhz (sejccmoirj ) View more | ||||||
Phase 2 | 69 | (Cohort 1) | rjrdiqycjp = lkijfdspty lvteudnhqj (xqxudqhnnu, bsrxzkurxm - mknfaxhxmc) View more | - | 29 May 2026 | ||
(Cohort 2) | rjrdiqycjp = ozamtvithc lvteudnhqj (xqxudqhnnu, slbwukixoj - dmqepxjasm) View more | ||||||
Not Applicable | Diffuse large B-cell lymphoma recurrent Second line | 54 | fofbzcbrxt(osmenwqvbu) = oxlelgbmed douzjtfuny (wkqojaaivu ) View more | Positive | 12 May 2026 | ||
Phase 2 | 38 | dqhjnmdkzl(wyvqfmrqna) = plsnpvvfiu zxpdefnxef (jxoffzqpei ) View more | Positive | 12 May 2026 |
Login to view more data
Translational Medicine
Boost your research with our translational medicine data.
login
or

Deal
Boost your decision using our deal data.
login
or

Core Patent
Boost your research with our Core Patent data.
login
or

Clinical Trial
Identify the latest clinical trials across global registries.
login
or

Approval
Accelerate your research with the latest regulatory approval information.
login
or
Regulation
Understand key drug designations in just a few clicks with Synapse.
login
or
Hiro LS Researcher
The AI Search Engine Built to Accelerate Biopharma Decisions
Search across billion-scale life sciences data to uncover signals, validate evidence, and act with confidence.
Ask any biopharma research question→
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, Patsnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Discover Synapse Data Servers
Synapse data is now integrated into the PatSnap LS Model Context Protocol (MCP) service. Customize your LLM agent now using our MCP server!
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free