Request Demo
Last update 06 Dec 2025
AZD-2816
Last update 06 Dec 2025
Overview
Basic Info
Drug Type Recombinant vector vaccine, Prophylactic vaccine |
Synonyms SARS-CoV-2 spike glycoprotein variant vaccine (adenoviral vector vaccine, COVID-19), University of Oxford/AstraZeneca, AZD-2816 |
Target |
Action modulators |
Mechanism SARS-CoV-2 S protein modulators(SARS-CoV-2 S protein modulators) |
Therapeutic Areas |
Active Indication |
Inactive Indication- |
Originator Organization |
Active Organization |
Inactive Organization |
License Organization- |
Drug Highest PhasePhase 3 |
First Approval Date- |
Regulation- |

Login to view timeline
Related
1
Clinical Trials associated with AZD-2816NCT04973449
A Phase II/III Partially Double-Blinded, Randomised, Multinational, Active-Controlled Study in Both Previously Vaccinated and Unvaccinated Adults to Determine the Safety and Immunogenicity of AZD2816, a Vaccine for the Prevention of COVID-19 Caused by Variant Strains of SARS-CoV-2
100 Clinical Results associated with AZD-2816
Login to view more data
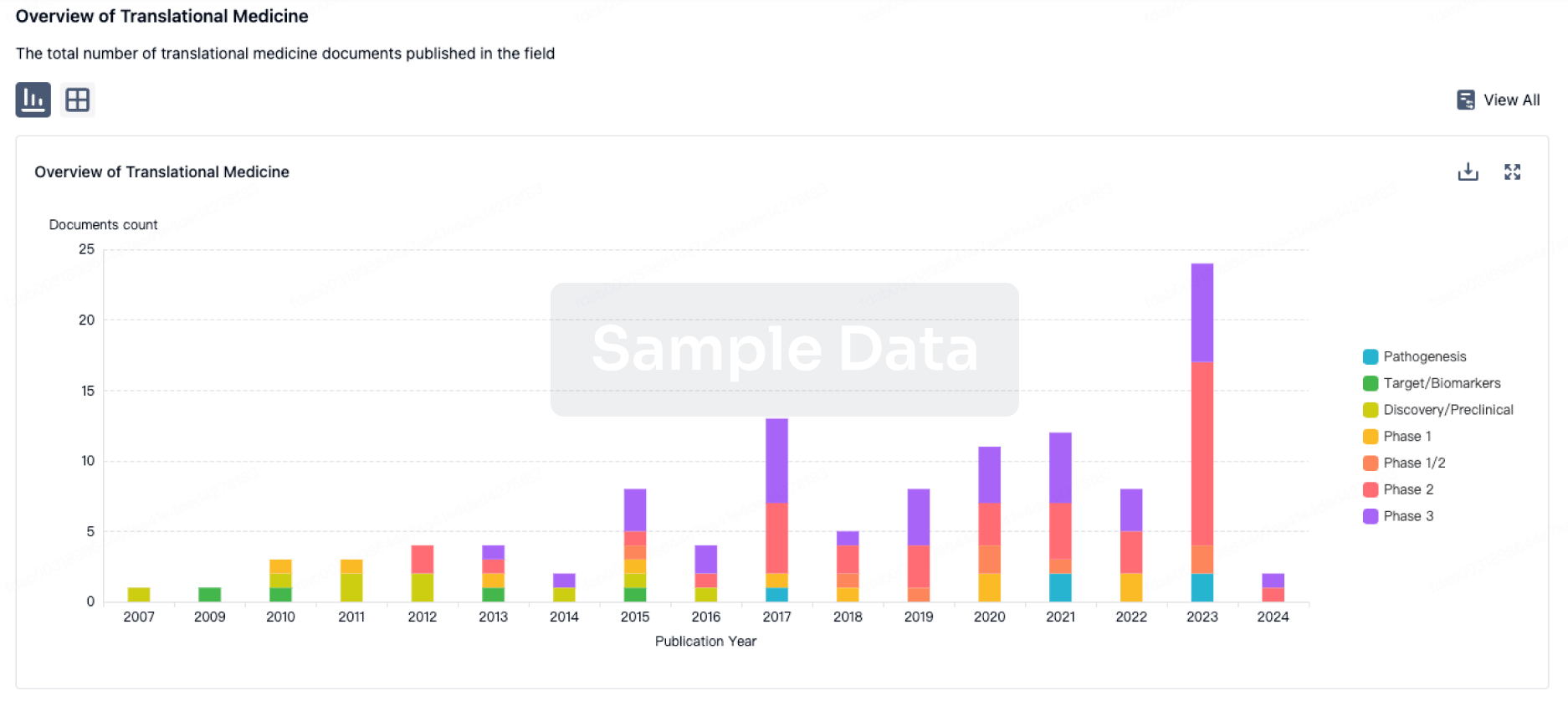
100 Translational Medicine associated with AZD-2816
Login to view more data
100 Patents (Medical) associated with AZD-2816
Login to view more data
21
Literatures (Medical) associated with AZD-281601 Aug 2024Lancet Microbe
Immunogenicity and safety of beta variant COVID-19 vaccine AZD2816 and AZD1222 (ChAdOx1 nCoV-19) as primary-series vaccination for previously unvaccinated adults in Brazil, South Africa, Poland, and the UK: a randomised, partly double-blinded, phase 2/3 non-inferiority immunobridging study
Article
Author: Shoemaker, Kathryn ; Badal-Faesen, Sharlaa ; Lambe, Teresa ; Bhorat, Qasim E ; Akhund, Tauseefullah ; Petropoulos, Christos J ; Mantyka, Jolanta ; Rugieri, Sidelcina ; Burgess, Lesley ; Aksyuk, Anastasia ; Vekemans, Johan ; Jones, Colin ; Moura de Oliveira Paiva, Maria Sanali ; Szylak, Ameena ; Bansal, Himanshu ; Engelbrecht, Johannes ; Pollard, Andrew J ; Ahmad, Abdullahi ; Costa Clemens, Sue Ann ; Seegobin, Seth ; Brites, Carlos ; Koen, Anthonet ; Jepson, Brett ; Greffrath, Johann ; Lombaard, Johan J ; Hirsch, Ian ; Vasconcellos, Eduardo ; Kobielusz-Gembala, Iwona ; Smith, Catherin C ; Bibi, Sagida ; Wrin, Terri ; Ramasamy, Maheshi N ; Matthews, Sam ; Stanely, Ann Marie ; Pipolo Milan, Eveline ; Bennet, Jaclyn A ; Wilkins, Deidre ; Khan, Mark ; Aley, Parvinder K ; Kelly, Elizabeth J ; Villafana, Tonya ; Olsson, Urban ; Sprinz, Eduardo ; Sorio, Guilherme L ; Green, Justin A ; de Oliveira Paiva, Hugo Diógenes
BACKGROUND:
AZD2816 is a variant-adapted COVID-19 vaccine that expresses the full-length SARS-CoV-2 beta variant spike protein but is otherwise similar to AZD1222 (ChAdOx1 nCoV-19). This study aimed to evaluate the safety and immunogenicity of AZD1222 or AZD2816 (or both) primary-series vaccination in a cohort of adult participants who were previously unvaccinated.
METHODS:
In this phase 2/3, randomised, multinational, active-controlled, non-inferiority, immunobridging study, adult participants previously unvaccinated for COVID-19 were enrolled at 16 study sites in Brazil, South Africa, Poland, and the UK. Participants were stratified by age, sex, and comorbidity and randomly assigned 5:5:5:2 to receive a primary series of AZD1222 (AZD1222 group), AZD2816 (AZD2816 [4-week] group), or AZD1222-AZD2816 (AZD1222-AZD2816 group) at 4-week dosing intervals, or AZD2816 at a 12-week interval (AZD2816 [12-week] group) and evaluated for safety and immunogenicity through 180 days after dose 2. Primary outcomes were safety (rates of solicited adverse events occurring during 7 days and unsolicited adverse events occurring during 28 days after each dose) and immunogenicity (non-inferiority of pseudovirus neutralising antibody geometric mean titre [GMT], GMT ratio margin of 0·67, and seroresponse rate, rate difference margin of -10%, recorded 28 days after dose 2 with AZD2816 [4-week interval] against beta vs AZD1222 against ancestral SARS-CoV-2) in participants who were seronegative at baseline. This trial is registered with ClinicalTrials.gov, NCT04973449, and is completed.
FINDINGS:
Between July 7 and Nov 12, 2021, 1449 participants were assigned to the AZD1222 group (n=413), the AZD2816 (4-week) group (n=415), the AZD1222-AZD2816 group (n=412), and the AZD2816 (12-week) group (n=209). Ten (2·6%) of 378 participants who were seronegative at baseline in the AZD1222 group, nine (2·4%) of 379 in the AZD2816 (4-week) group, eight (2·1%) of 380 in the AZD1222-AZD2816 group, and 11 (5·8%) of 191 in the AZD2816 (12-week) group had vaccine-related unsolicited adverse events. Serious adverse events were recorded in one (0·3%) participant in the AZD1222 group, one (0·3%) in the AZD2816 (4-week) group, two (0·5%) in the AZD1222-AZD2816 group, and none in the AZD2816 (12-week) group. Co-primary immunogenicity endpoints were met: neutralising antibody GMT (ratio 1·19 [95% CI 1·08-1·32]; lower bound greater than 0·67) and seroresponse rate (difference 1·7% [-3·1 to 6·5]; lower bound greater than -10%) at 28 days after dose 2 were non-inferior in the AZD2816 (4-week) group against beta versus in the AZD1222 group against ancestral SARS-CoV-2. Seroresponse rates were highest with AZD2816 against beta (12-week interval 94·3% [95% CI 89·4-97·3]; 4-week interval 85·7% [81·5-89·2]) and with AZD1222 (84·6% [80·3-88·2]) against ancestral SARS-CoV-2.
INTERPRETATION:
Primary series of AZD1222 and AZD2816 were well tolerated, with no emergent safety concerns. Both vaccines elicited robust immunogenicity against beta and ancestral SARS-CoV-2 with greater responses demonstrated when testing against SARS-CoV-2 strains that matched those targeted by the respective vaccine. These findings demonstrate the continued importance of ancestral COVID-19 vaccines in protecting against severe COVID-19 and highlight the feasibility of using the ChAdOx1 platform to develop COVID-19 vaccines against future SARS-CoV-2 variants.
FUNDING:
AstraZeneca.
01 Mar 2024Immunobiology
Evaluation of the serum levels of CCL2, CCL3, and IL-29 after first and second administrations of the COVID-19 vaccine (Oxford–AstraZeneca)
Article
Author: Rezvani, Mahdi ; Taghipour Khaje Sharifi, Gholamhossein ; Kaeidi, Ayat ; Abbasifard, Mitra ; Bagheri-Hosseinabadi, Zahra
BACKGROUND:
Previous studies show that chemokines and cytokines play a very important role in eliciting an appropriate response against viruses. Vaccination causes inflammation in the person receiving the vaccine, accompanied with production of inflammatory molecules by immune cells. The more and better the production and expression of chemokines and cytokines by immune cells, the better the response of the acquired immune system. Chemokines and cytokines are critical in promoting the innate immune response against the COVID-19. Here we intended to assess serum levels of CCL2, CCL3, and interleukin (IL)-29 in patients received COVID-19 vaccine.
METHODS:
In this study, 40 subjects vaccinated with the Oxford-AstraZeneca COVID-19 vaccine were selected. Blood samples were collected before injection of the vaccine, 3-5 days after the first dose injection, and 3-5 days subsequent to the second vaccination. To check the serum level of CCL2, CCL3, and IL-29, ELISA technique was used.
RESULTS:
Our results indicated that the serum levels of CCL2, CCL3, and IL-29 were significantly higher after first and second dose of vaccination compared to before vaccine administration. Furthermore, serum levels of all these mediators were higher after second dose of vaccine compared to the first vaccine administration.
CONCLUSIONS:
Oxford-AstraZeneca COVID-19 vaccine is able to induce inflammatory CCL2 and CCL3 chemokines as well as protective interferon lambda (IL-29).
01 Jan 2024Skinmed
Sweet Syndrome-Like Disorder Induced by the Oxford-AstraZeneca® SARS-CoV-2 Vaccine.
Article
Author: Dantas, Lia D P ; Schoenardie, Bruna O ; Bonamigo, Renan R ; Damke, Jéssica P
1
News (Medical) associated with AZD-281626 May 2022
VaccineCollaborateAntibodymRNA
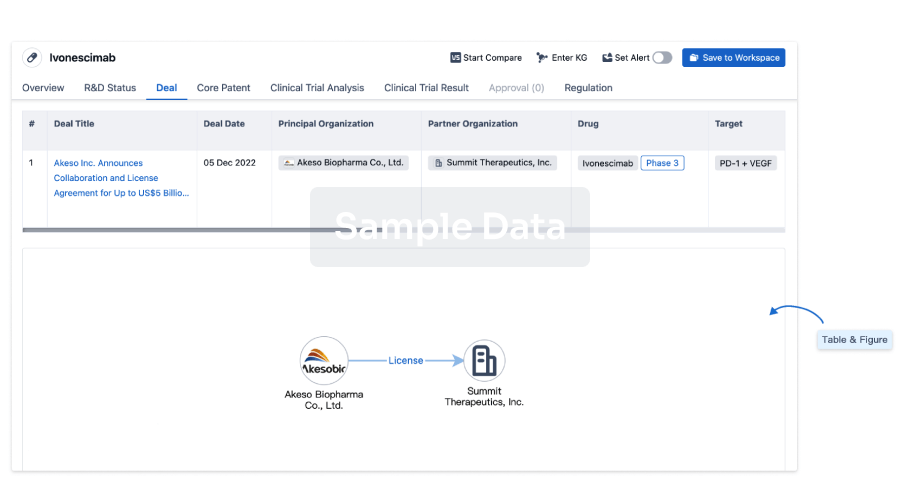
100 Deals associated with AZD-2816
Login to view more data
R&D Status
10 top R&D records. to view more data
Login
| Indication | Highest Phase | Country/Location | Organization | Date |
|---|---|---|---|---|
| COVID-19 | Phase 3 | Brazil | 27 Jun 2021 | |
| COVID-19 | Phase 3 | Poland | 27 Jun 2021 | |
| COVID-19 | Phase 3 | South Africa | 27 Jun 2021 | |
| COVID-19 | Phase 3 | United Kingdom | 27 Jun 2021 |
Login to view more data
Clinical Result
Clinical Result
Indication
Phase
Evaluation
View All Results
Phase 2/3 | - | cxulnwcial(eyuleaugmy) = btroungtub ttskwjuhcc (zsktjtvbzg ) View more | - | 01 Nov 2023 | |||
cxulnwcial(eyuleaugmy) = qikucwzbqh ttskwjuhcc (zsktjtvbzg ) View more |
Login to view more data
Translational Medicine
Boost your research with our translational medicine data.
login
or
Deal
Boost your decision using our deal data.
login
or
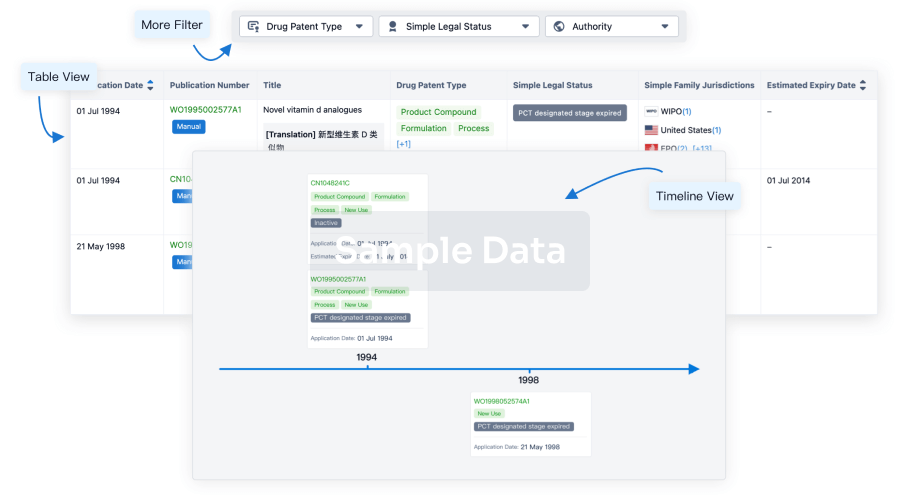
Core Patent
Boost your research with our Core Patent data.
login
or
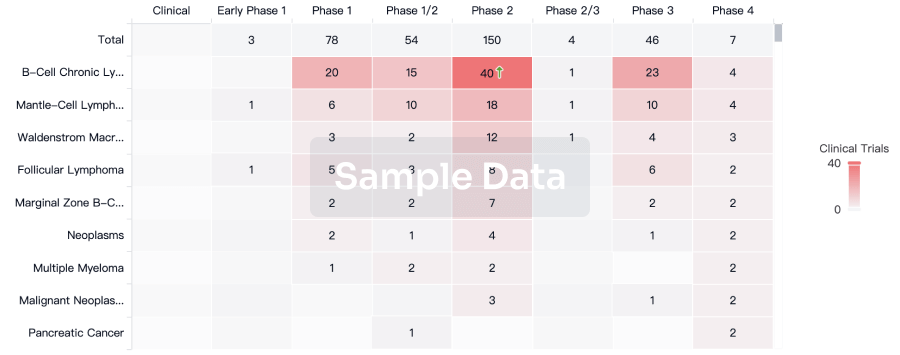
Clinical Trial
Identify the latest clinical trials across global registries.
login
or
Approval
Accelerate your research with the latest regulatory approval information.
login
or
Regulation
Understand key drug designations in just a few clicks with Synapse.
login
or
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free