Last update 19 Sep 2024

Senzime AB
Last update 19 Sep 2024
Overview
Related
Comparison of Electromyography-based TetraGraph and Acceleromyography-based TOF-Watch SX Neuromuscular Monitors Under Clinical Conditions

Randomized Double---Blinded, Controlled Trial to Compare the Effectiveness of Sugammadex vs. Placebo to Prevent Residual Neuromuscular Block in the Post---Anesthesia Care Unit as Evaluated With a Non---Invasive Respiratory Volume Monitor
Local Metabolism of the Gastric Tube Reconstruction After Esophagectomy
100 Clinical Results associated with Senzime AB
Login to view more data
Login to view more data
01 Jun 2020Journal of Clinical Monitoring and ComputingQ3 · MEDICINE
Use of a novel non-invasive respiratory monitor to study changes in pulmonary ventilation during labor epidural analgesia
Q3 · MEDICINE
Article
Author: Choi, Lynn ; Chau, Anton ; Kodali, Bhavani Shankar ; Brayanov, Jordan ; Harvey, Brian C ; Palanisamy, Arvind ; Tsen, Lawrence C
01 Jan 2020Critical Care Medicine
1153: PREDICTING LOW MINUTE VENTILATION AND OXYGEN DESATURATION FROM EARLY POSTOPERATIVE DATA
Author: Vitale, Joseph ; Saha, Partha ; Essber, Hani ; Chelnick, David ; Hovsepyan, Karen ; Turan, Alparslan ; Adegboye, Janet ; Imsirovic, Jasmin ; Rivas, Eva
01 Feb 2019Journal of Clinical AnesthesiaQ2 · MEDICINE
Minute ventilation assessment in the PACU is useful to predict postoperative respiratory depression following discharge to the floor: A prospective cohort study
Q2 · MEDICINE
Article
Author: Zahedi, Farhad ; Schumann, Roman ; Bonney, Iwona ; Harvey, Brian
07 Feb 2024
100 Deals associated with Senzime AB
Login to view more data
100 Translational Medicine associated with Senzime AB
Login to view more data
Corporation Tree
Boost your research with our corporation tree data.
login
or
Pipeline
Pipeline Snapshot as of 06 Oct 2024
No data posted
Login to keep update
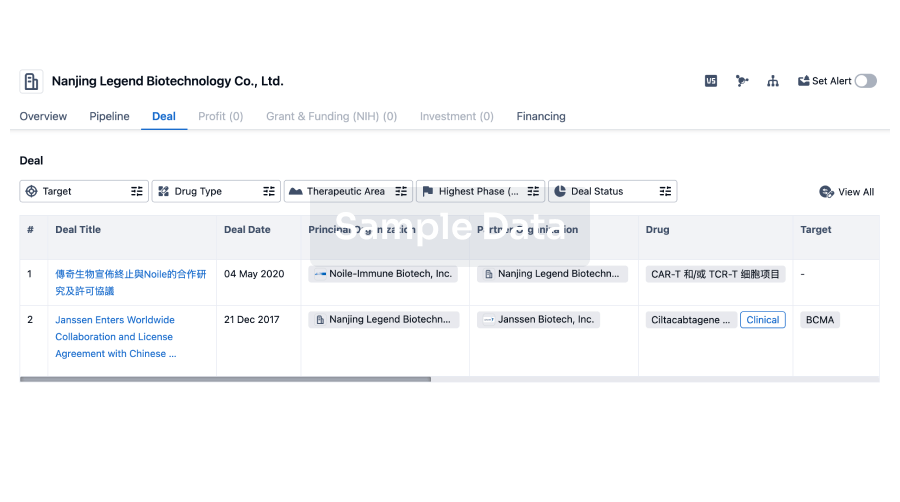
Deal
Boost your decision using our deal data.
login
or
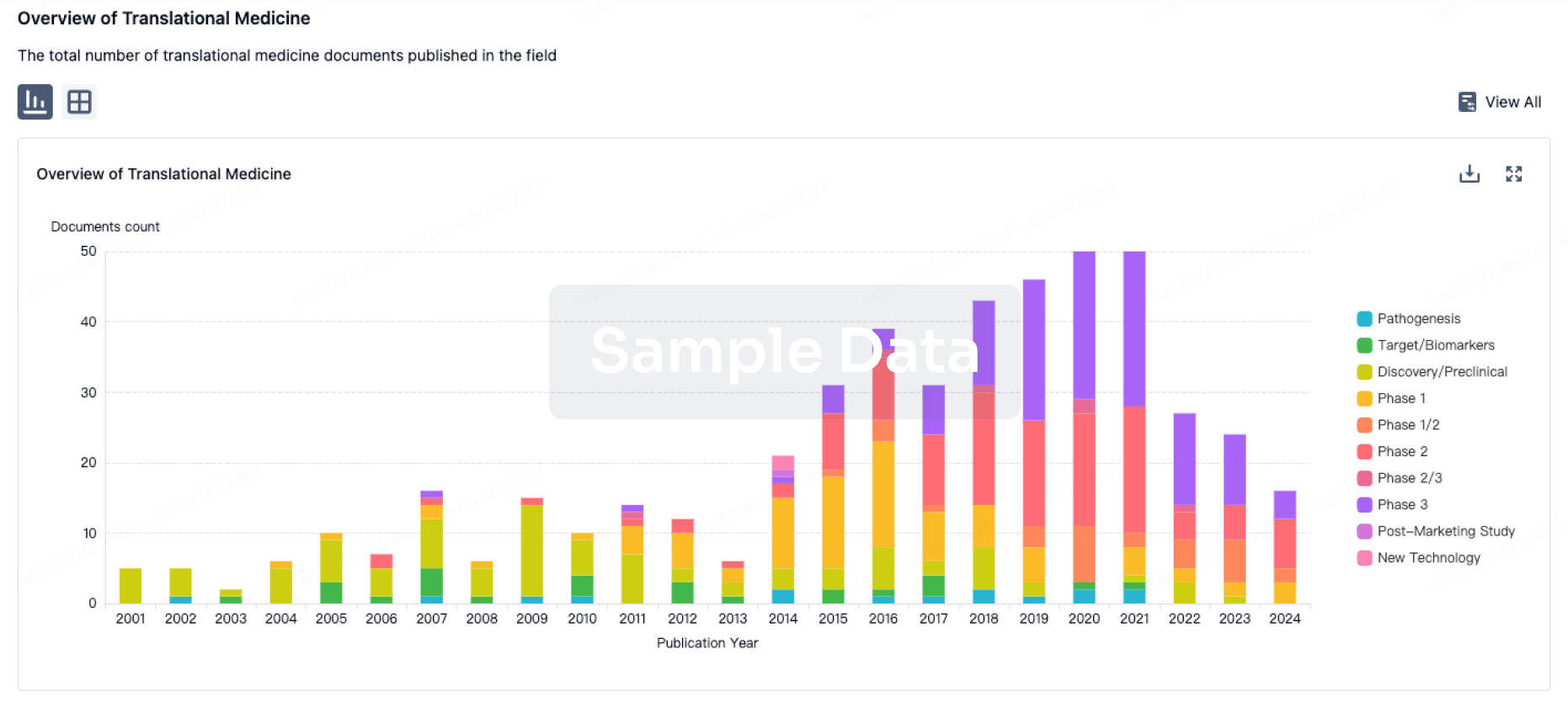
Translational Medicine
Boost your research with our translational medicine data.
login
or
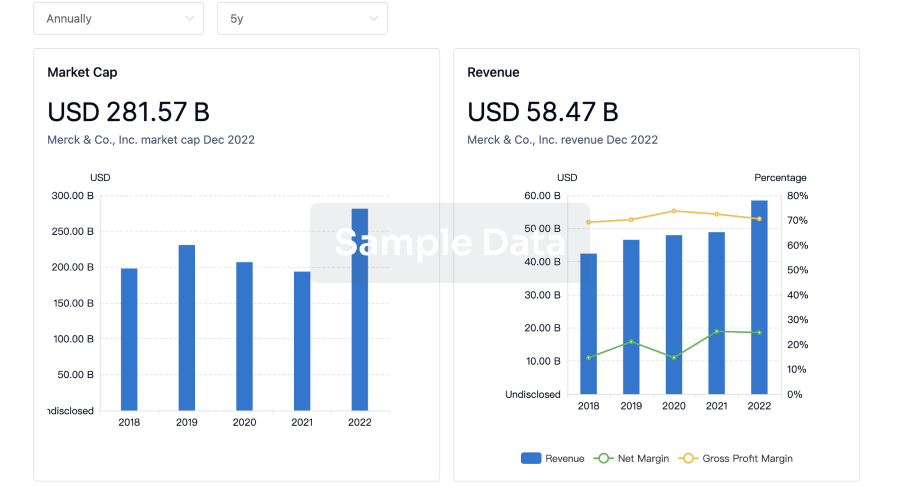
Profit
Explore the financial positions of over 360K organizations with Synapse.
login
or
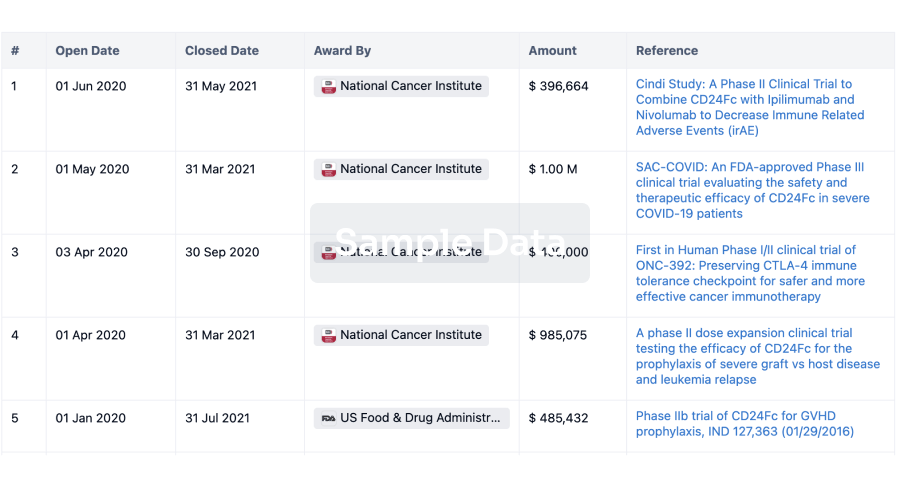
Grant & Funding(NIH)
Access more than 2 million grant and funding information to elevate your research journey.
login
or
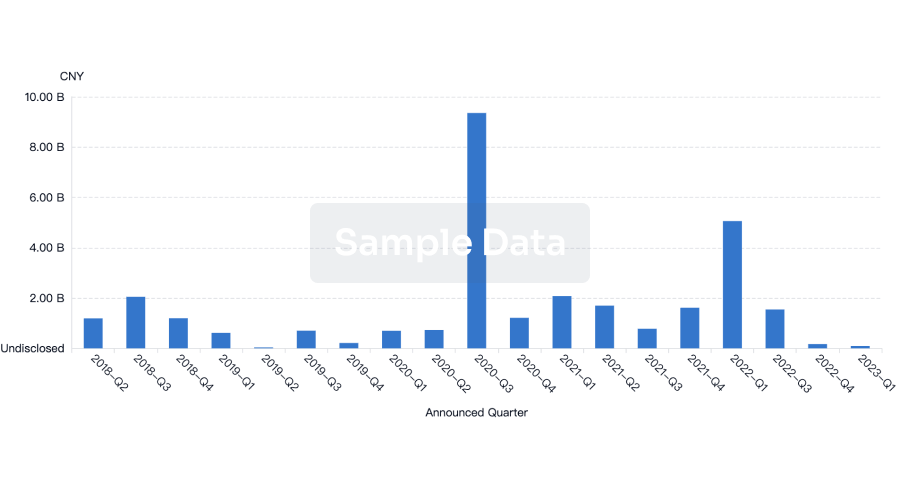
Investment
Gain insights on the latest company investments from start-ups to established corporations.
login
or
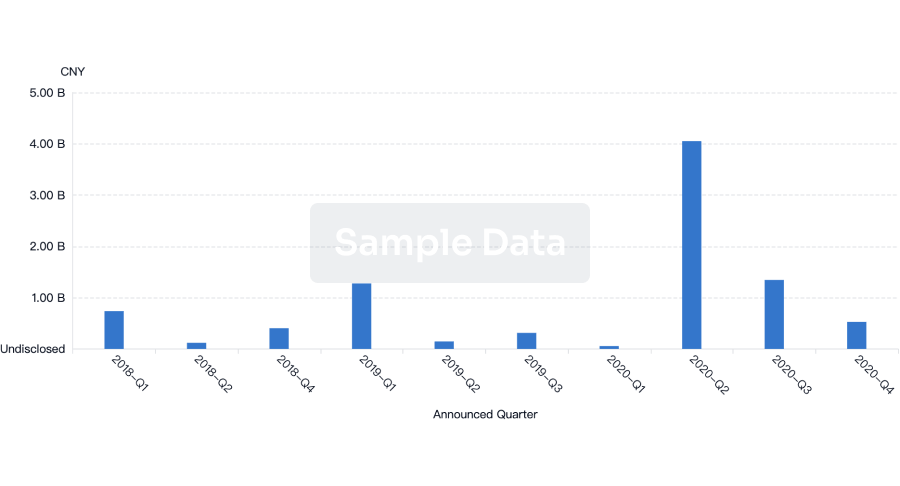
Financing
Unearth financing trends to validate and advance investment opportunities.
login
or
Chat with Hiro
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free