Request Demo
What is Fenoterol Hydrobromide used for?
15 June 2024
Fenoterol Hydrobromide is a bronchodilator that is frequently employed in the treatment of lung conditions such as asthma and chronic obstructive pulmonary disease (COPD). Marketed under several trade names, including Berotec and Berodual, this beta-2 adrenergic agonist is designed to relax the muscles in the airways, thereby facilitating easier breathing. It targets the beta-2 adrenergic receptors located in the bronchial smooth muscle, leading to bronchodilation. Research institutions around the world have explored its efficacy and safety profiles extensively, with clinical trials and peer-reviewed studies validating its role in respiratory therapy. Initially approved for medical use several decades ago, Fenoterol Hydrobromide continues to be a cornerstone in the management of obstructive airway diseases.
Fenoterol Hydrobromide is classified as a short-acting beta-2 adrenergic agonist (SABA). Its primary indication is for the relief and prevention of bronchospasm associated with asthma and COPD. This drug has undergone various phases of clinical trials, aimed at ensuring its effectiveness while minimizing potential risks. Over the years, the research has broadened to include pediatric applications and combinations with other bronchodilators and anti-inflammatory medications, enhancing its utility in diverse patient populations.
The mechanism of action of Fenoterol Hydrobromide revolves around its ability to stimulate beta-2 adrenergic receptors in the bronchial smooth muscle. Upon binding to these receptors, Fenoterol Hydrobromide activates adenylate cyclase, which catalyzes the conversion of ATP to cyclic AMP (cAMP). The increased concentration of cAMP leads to the activation of protein kinase A (PKA), which in turn phosphorylates and inactivates myosin light-chain kinase. This series of biochemical events results in the relaxation of smooth muscle cells in the bronchi, leading to bronchodilation and improved airflow.
Moreover, Fenoterol Hydrobromide exhibits some degree of selectivity for beta-2 over beta-1 adrenergic receptors, which are predominantly found in the heart. This selectivity helps in minimizing cardiovascular side effects, although higher doses may still influence heart rate and myocardial contractility due to residual beta-1 receptor stimulation.
Fenoterol Hydrobromide can be administered via several routes, including inhalation, oral tablet, and intravenous injection, although inhalation is the most common method. The inhalation route is preferred because it delivers the drug directly to the site of action, allowing for rapid onset and reduced systemic side effects. When inhaled, the onset of action typically occurs within 5 minutes, reaching peak effect within 30 minutes, and lasting for about 4-6 hours.
For acute asthma attacks or sudden bronchospasm, Fenoterol Hydrobromide is often administered via a metered-dose inhaler (MDI) or a nebulizer. The dosage can vary depending on the severity of the condition, but common practice involves 1-2 inhalations as needed, with a maximum number of inhalations per day as advised by a healthcare provider. For chronic management, it can be used regularly, although it is crucial to adhere to prescribed dosages to avoid tolerance and adverse effects.
Despite its efficacy, Fenoterol Hydrobromide is not without side effects. Common side effects include tremors, nervousness, and headaches, which are generally mild and transient. Palpitations, tachycardia, and muscle cramps can also occur, especially at higher doses. In rare cases, severe side effects such as paradoxical bronchospasm, hypotension, or chest pain may manifest, necessitating immediate medical attention.
Contraindications for Fenoterol Hydrobromide include patients with known hypersensitivity to the drug, as well as those with tachyarrhythmias or hypertrophic obstructive cardiomyopathy. Caution is advised when administering Fenoterol Hydrobromide to patients with cardiovascular disorders, hyperthyroidism, or diabetes, as it may exacerbate these conditions.
Drug interactions are an important consideration with Fenoterol Hydrobromide. Co-administration with other beta-adrenergic agonists can potentiate the effects, increasing the risk of cardiovascular side effects. Conversely, beta-blockers, particularly non-selective ones, can antagonize the bronchodilatory effects of Fenoterol Hydrobromide, potentially leading to reduced efficacy.
Monoamine oxidase inhibitors (MAOIs) and tricyclic antidepressants can also amplify the cardiovascular side effects of Fenoterol Hydrobromide, necessitating caution and possible dosage adjustments. Moreover, corticosteroids, diuretics, and xanthine derivatives like theophylline may enhance the hypokalemic effect of Fenoterol Hydrobromide, increasing the risk of cardiac arrhythmias. Consequently, regular monitoring of potassium levels is recommended when these drugs are used concomitantly.
In conclusion, Fenoterol Hydrobromide is a vital medication in the management of asthma and COPD, providing rapid and effective bronchodilation. Understanding its mechanism of action, proper usage, potential side effects, and interactions with other drugs is crucial for maximizing its benefits while minimizing risks. Ongoing research continues to refine its utility and expand its applications, ensuring that it remains a valuable tool in respiratory therapy. As always, consultation with healthcare professionals is essential to tailor treatment plans to individual patient needs and circumstances.
Fenoterol Hydrobromide is classified as a short-acting beta-2 adrenergic agonist (SABA). Its primary indication is for the relief and prevention of bronchospasm associated with asthma and COPD. This drug has undergone various phases of clinical trials, aimed at ensuring its effectiveness while minimizing potential risks. Over the years, the research has broadened to include pediatric applications and combinations with other bronchodilators and anti-inflammatory medications, enhancing its utility in diverse patient populations.
The mechanism of action of Fenoterol Hydrobromide revolves around its ability to stimulate beta-2 adrenergic receptors in the bronchial smooth muscle. Upon binding to these receptors, Fenoterol Hydrobromide activates adenylate cyclase, which catalyzes the conversion of ATP to cyclic AMP (cAMP). The increased concentration of cAMP leads to the activation of protein kinase A (PKA), which in turn phosphorylates and inactivates myosin light-chain kinase. This series of biochemical events results in the relaxation of smooth muscle cells in the bronchi, leading to bronchodilation and improved airflow.
Moreover, Fenoterol Hydrobromide exhibits some degree of selectivity for beta-2 over beta-1 adrenergic receptors, which are predominantly found in the heart. This selectivity helps in minimizing cardiovascular side effects, although higher doses may still influence heart rate and myocardial contractility due to residual beta-1 receptor stimulation.
Fenoterol Hydrobromide can be administered via several routes, including inhalation, oral tablet, and intravenous injection, although inhalation is the most common method. The inhalation route is preferred because it delivers the drug directly to the site of action, allowing for rapid onset and reduced systemic side effects. When inhaled, the onset of action typically occurs within 5 minutes, reaching peak effect within 30 minutes, and lasting for about 4-6 hours.
For acute asthma attacks or sudden bronchospasm, Fenoterol Hydrobromide is often administered via a metered-dose inhaler (MDI) or a nebulizer. The dosage can vary depending on the severity of the condition, but common practice involves 1-2 inhalations as needed, with a maximum number of inhalations per day as advised by a healthcare provider. For chronic management, it can be used regularly, although it is crucial to adhere to prescribed dosages to avoid tolerance and adverse effects.
Despite its efficacy, Fenoterol Hydrobromide is not without side effects. Common side effects include tremors, nervousness, and headaches, which are generally mild and transient. Palpitations, tachycardia, and muscle cramps can also occur, especially at higher doses. In rare cases, severe side effects such as paradoxical bronchospasm, hypotension, or chest pain may manifest, necessitating immediate medical attention.
Contraindications for Fenoterol Hydrobromide include patients with known hypersensitivity to the drug, as well as those with tachyarrhythmias or hypertrophic obstructive cardiomyopathy. Caution is advised when administering Fenoterol Hydrobromide to patients with cardiovascular disorders, hyperthyroidism, or diabetes, as it may exacerbate these conditions.
Drug interactions are an important consideration with Fenoterol Hydrobromide. Co-administration with other beta-adrenergic agonists can potentiate the effects, increasing the risk of cardiovascular side effects. Conversely, beta-blockers, particularly non-selective ones, can antagonize the bronchodilatory effects of Fenoterol Hydrobromide, potentially leading to reduced efficacy.
Monoamine oxidase inhibitors (MAOIs) and tricyclic antidepressants can also amplify the cardiovascular side effects of Fenoterol Hydrobromide, necessitating caution and possible dosage adjustments. Moreover, corticosteroids, diuretics, and xanthine derivatives like theophylline may enhance the hypokalemic effect of Fenoterol Hydrobromide, increasing the risk of cardiac arrhythmias. Consequently, regular monitoring of potassium levels is recommended when these drugs are used concomitantly.
In conclusion, Fenoterol Hydrobromide is a vital medication in the management of asthma and COPD, providing rapid and effective bronchodilation. Understanding its mechanism of action, proper usage, potential side effects, and interactions with other drugs is crucial for maximizing its benefits while minimizing risks. Ongoing research continues to refine its utility and expand its applications, ensuring that it remains a valuable tool in respiratory therapy. As always, consultation with healthcare professionals is essential to tailor treatment plans to individual patient needs and circumstances.
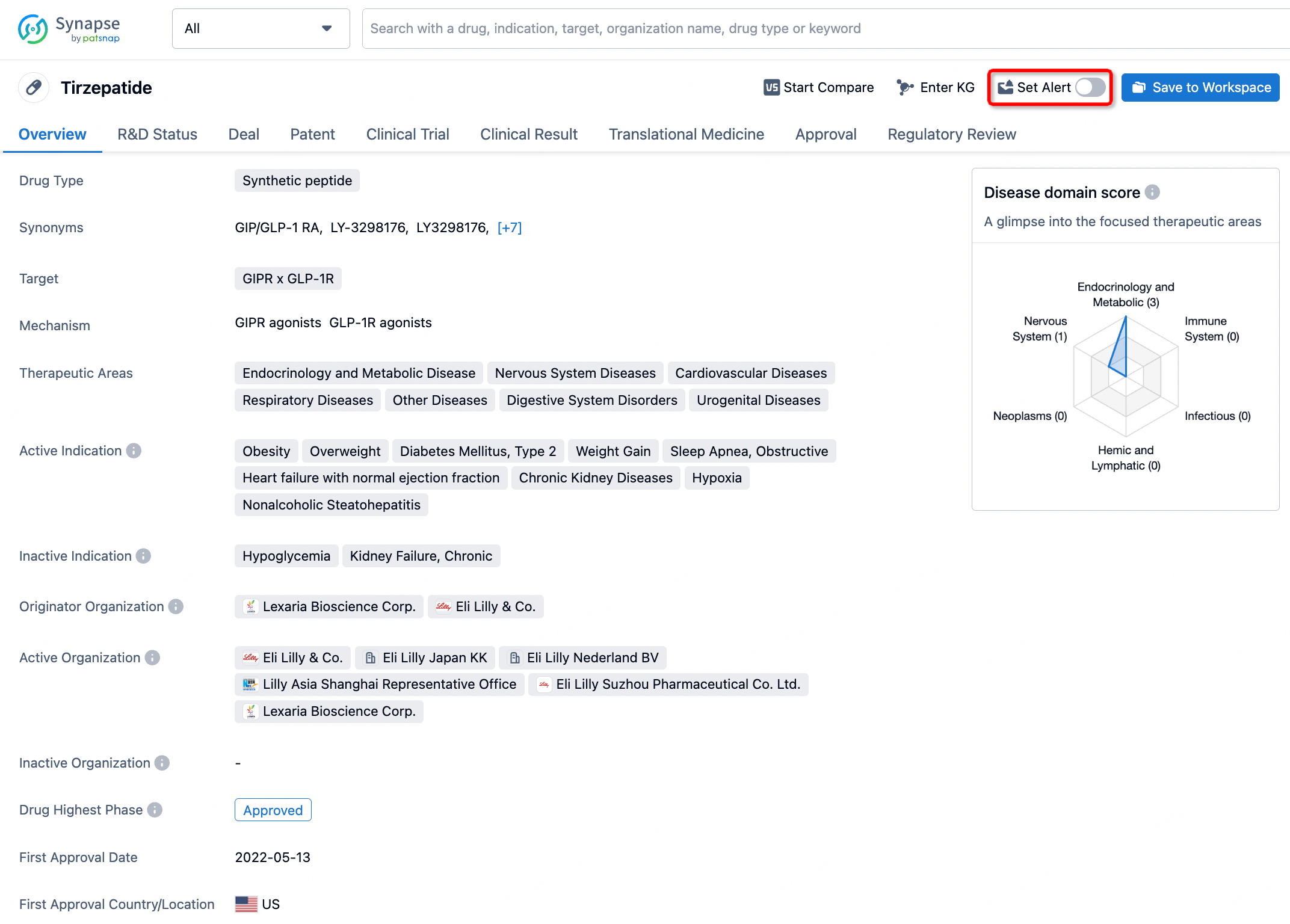
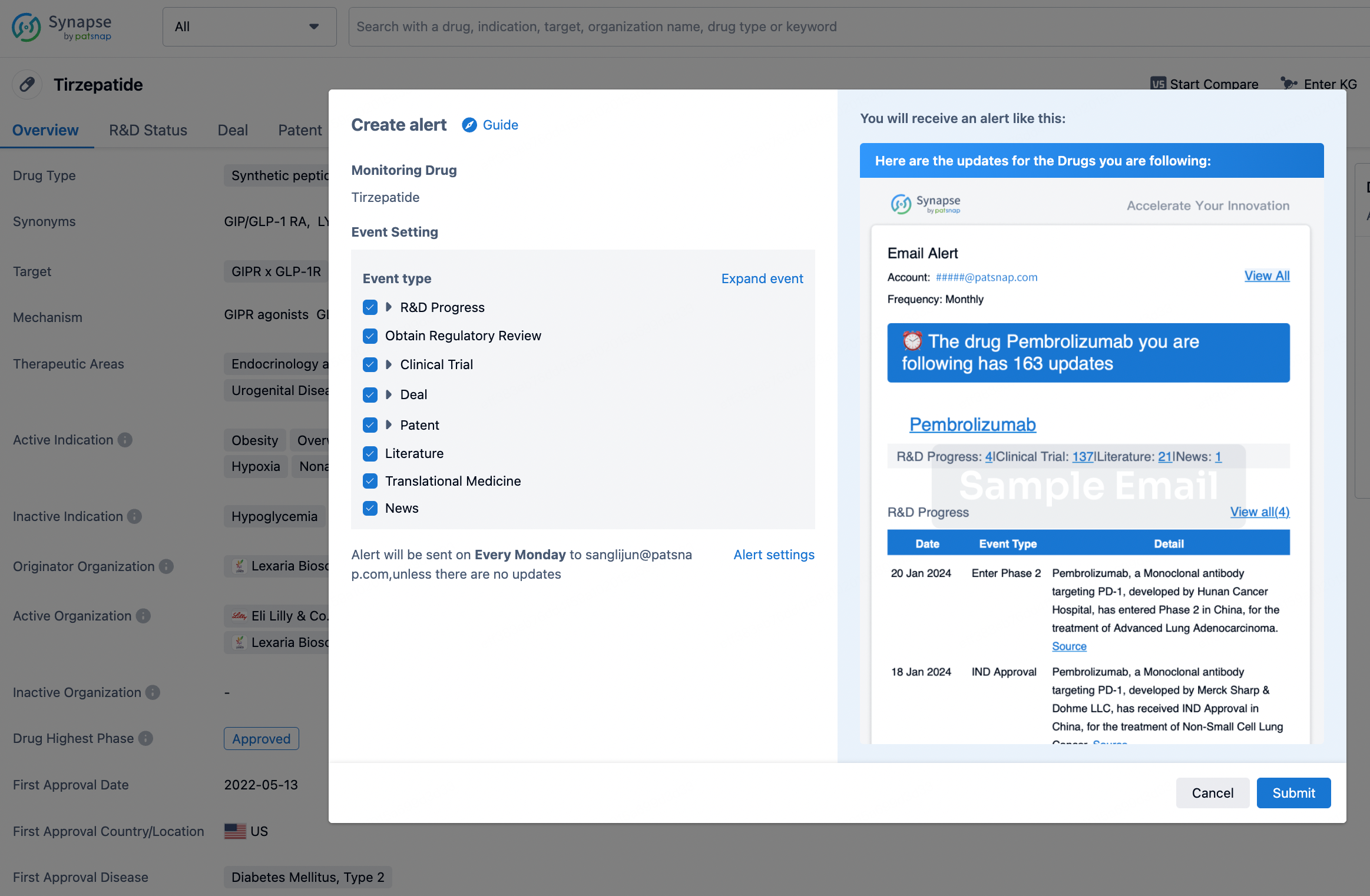
How to obtain the latest development progress of all drugs?
In the Synapse database, you can stay updated on the latest research and development advances of all drugs. This service is accessible anytime and anywhere, with updates available daily or weekly. Use the "Set Alert" function to stay informed. Click on the image below to embark on a brand new journey of drug discovery!
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.