Request Demo
What is Nafcillin Sodium used for?
15 June 2024
Nafcillin Sodium is a penicillinase-resistant beta-lactam antibiotic that is used to treat infections caused by penicillinase-producing staphylococci. It is marketed under various trade names, including Unipen and Nafcil. This antibiotic is particularly effective against Gram-positive bacteria, especially staphylococci, making it a critical weapon in the fight against bacterial infections that are resistant to other penicillins. Nafcillin Sodium is often used in healthcare settings and is a go-to choice for clinicians when dealing with resistant bacterial strains.
The primary targets of Nafcillin Sodium are staphylococcal bacteria, including methicillin-sensitive Staphylococcus aureus (MSSA). It is usually reserved for severe infections such as osteomyelitis, endocarditis, and septicemia where penicillinase-producing staphylococci are the confirmed or suspected cause. Research institutions have extensively studied Nafcillin Sodium, particularly its efficacy and resistance patterns, to better understand how to use this drug in the clinical setting.
Despite being on the market for several decades, Nafcillin Sodium continues to be relevant due to ongoing research and development. New formulations and delivery methods are periodically investigated to improve patient outcomes and minimize side effects. The drug has undergone rigorous clinical trials to ensure its efficacy and safety, and ongoing research aims to address emerging resistance patterns.
Nafcillin Sodium belongs to the beta-lactam class of antibiotics, specifically the penicillinase-resistant penicillins. This characteristic makes it uniquely effective against bacteria that produce the enzyme penicillinase, which usually renders penicillin antibiotics ineffective. As a result, it is an invaluable drug in treating infections where other antibiotics fail.
The mechanism of action of Nafcillin Sodium involves inhibiting bacterial cell wall synthesis. Like other beta-lactam antibiotics, Nafcillin Sodium binds to penicillin-binding proteins (PBPs) located in the cell wall of susceptible bacteria. These PBPs are enzymes that play a critical role in the third and final stage of bacterial cell wall synthesis. By binding to these proteins, Nafcillin Sodium inhibits their activity, thereby preventing the cross-linking of peptidoglycan chains, which are essential components of the bacterial cell wall.
The inhibition of PBPs leads to the weakening of the bacterial cell wall, ultimately causing cell lysis and death. This mechanism is particularly effective against actively dividing bacteria that are in the process of synthesizing new cell walls. Since Nafcillin Sodium is resistant to the action of penicillinase, it remains effective against bacteria that produce this enzyme, making it a reliable option for treating staphylococcal infections.
Nafcillin Sodium can be administered in several ways, including intravenously (IV) and intramuscularly (IM). The route of administration often depends on the severity of the infection and the clinical setting. For severe infections, intravenous administration is preferred as it allows for higher plasma concentrations of the drug and quicker therapeutic effects.
Intravenous administration involves diluting the drug in a suitable IV fluid, such as saline, and infusing it over a specified period, usually 30 to 60 minutes. This method ensures rapid onset of action, typically within an hour, which is crucial for severe infections like septicemia or endocarditis. Intramuscular administration, on the other hand, involves injecting the drug directly into a large muscle mass, such as the gluteus or thigh muscles. This route is less commonly used due to the pain associated with IM injections and slower onset of action compared to IV administration.
The dosage of Nafcillin Sodium varies depending on the type and severity of the infection, the patient's age, weight, and kidney function. For adults, the typical dosage ranges from 1 to 2 grams every 4 to 6 hours. For pediatric patients, the dosage is usually calculated based on body weight. It is essential to complete the prescribed course of Nafcillin Sodium, even if symptoms improve before the medication is finished, to ensure the complete eradication of the bacteria and to prevent the development of antibiotic resistance.
Like all medications, Nafcillin Sodium has potential side effects, some of which can be serious. Common side effects include gastrointestinal disturbances such as nausea, vomiting, and diarrhea. Less frequently, patients may experience rash, fever, and injection site reactions such as pain and inflammation.
Severe side effects are rare but can occur. These may include hypersensitivity reactions, such as anaphylaxis, which is a medical emergency requiring immediate attention. Signs of anaphylaxis include difficulty breathing, swelling of the face and throat, and severe rash. Patients with a known allergy to penicillins should avoid using Nafcillin Sodium due to the risk of cross-reactivity.
Nephrotoxicity is another potential severe side effect, particularly in patients with pre-existing kidney conditions or those receiving high doses of the drug. Symptoms of nephrotoxicity include changes in urine output, edema, and elevated blood urea nitrogen (BUN) and creatinine levels. It is essential to monitor kidney function regularly in patients receiving Nafcillin Sodium, especially those with underlying kidney issues.
Nafcillin Sodium can also cause liver toxicity, manifesting as elevated liver enzymes and, in rare cases, jaundice. Regular monitoring of liver function tests is recommended for patients on prolonged Nafcillin Sodium therapy. Other rare side effects include hematologic abnormalities such as neutropenia, thrombocytopenia, and eosinophilia.
Certain medications can interact with Nafcillin Sodium, potentially altering its effectiveness or increasing the risk of side effects. One of the most significant drug interactions occurs with warfarin, an anticoagulant. Nafcillin Sodium can enhance the metabolism of warfarin, reducing its anticoagulant effect and increasing the risk of thromboembolic events. It is crucial to monitor the International Normalized Ratio (INR) more frequently in patients taking both medications and adjust the warfarin dose as necessary.
Another notable interaction is with probenecid, a medication used to treat gout. Probenecid can inhibit the renal excretion of Nafcillin Sodium, leading to higher plasma levels of the antibiotic and an increased risk of toxicity. While this interaction can be used therapeutically to prolong the action of Nafcillin Sodium, it requires careful monitoring to avoid adverse effects.
Nafcillin Sodium may also interact with other beta-lactam antibiotics, such as cephalosporins and carbapenems, as well as with medications that affect renal function, such as diuretics and aminoglycosides. It is essential to review a patient's medication list thoroughly before initiating Nafcillin Sodium therapy to identify and manage potential drug interactions.
In conclusion, Nafcillin Sodium is a crucial antibiotic in the treatment of penicillinase-producing staphylococcal infections. Its penicillinase-resistant properties make it highly effective against resistant bacterial strains, and ongoing research continues to enhance our understanding of its use and efficacy. By understanding its mechanism of action, proper administration methods, potential side effects, and drug interactions, healthcare providers can optimize the therapeutic benefits of Nafcillin Sodium while minimizing risks to patients.
The primary targets of Nafcillin Sodium are staphylococcal bacteria, including methicillin-sensitive Staphylococcus aureus (MSSA). It is usually reserved for severe infections such as osteomyelitis, endocarditis, and septicemia where penicillinase-producing staphylococci are the confirmed or suspected cause. Research institutions have extensively studied Nafcillin Sodium, particularly its efficacy and resistance patterns, to better understand how to use this drug in the clinical setting.
Despite being on the market for several decades, Nafcillin Sodium continues to be relevant due to ongoing research and development. New formulations and delivery methods are periodically investigated to improve patient outcomes and minimize side effects. The drug has undergone rigorous clinical trials to ensure its efficacy and safety, and ongoing research aims to address emerging resistance patterns.
Nafcillin Sodium belongs to the beta-lactam class of antibiotics, specifically the penicillinase-resistant penicillins. This characteristic makes it uniquely effective against bacteria that produce the enzyme penicillinase, which usually renders penicillin antibiotics ineffective. As a result, it is an invaluable drug in treating infections where other antibiotics fail.
The mechanism of action of Nafcillin Sodium involves inhibiting bacterial cell wall synthesis. Like other beta-lactam antibiotics, Nafcillin Sodium binds to penicillin-binding proteins (PBPs) located in the cell wall of susceptible bacteria. These PBPs are enzymes that play a critical role in the third and final stage of bacterial cell wall synthesis. By binding to these proteins, Nafcillin Sodium inhibits their activity, thereby preventing the cross-linking of peptidoglycan chains, which are essential components of the bacterial cell wall.
The inhibition of PBPs leads to the weakening of the bacterial cell wall, ultimately causing cell lysis and death. This mechanism is particularly effective against actively dividing bacteria that are in the process of synthesizing new cell walls. Since Nafcillin Sodium is resistant to the action of penicillinase, it remains effective against bacteria that produce this enzyme, making it a reliable option for treating staphylococcal infections.
Nafcillin Sodium can be administered in several ways, including intravenously (IV) and intramuscularly (IM). The route of administration often depends on the severity of the infection and the clinical setting. For severe infections, intravenous administration is preferred as it allows for higher plasma concentrations of the drug and quicker therapeutic effects.
Intravenous administration involves diluting the drug in a suitable IV fluid, such as saline, and infusing it over a specified period, usually 30 to 60 minutes. This method ensures rapid onset of action, typically within an hour, which is crucial for severe infections like septicemia or endocarditis. Intramuscular administration, on the other hand, involves injecting the drug directly into a large muscle mass, such as the gluteus or thigh muscles. This route is less commonly used due to the pain associated with IM injections and slower onset of action compared to IV administration.
The dosage of Nafcillin Sodium varies depending on the type and severity of the infection, the patient's age, weight, and kidney function. For adults, the typical dosage ranges from 1 to 2 grams every 4 to 6 hours. For pediatric patients, the dosage is usually calculated based on body weight. It is essential to complete the prescribed course of Nafcillin Sodium, even if symptoms improve before the medication is finished, to ensure the complete eradication of the bacteria and to prevent the development of antibiotic resistance.
Like all medications, Nafcillin Sodium has potential side effects, some of which can be serious. Common side effects include gastrointestinal disturbances such as nausea, vomiting, and diarrhea. Less frequently, patients may experience rash, fever, and injection site reactions such as pain and inflammation.
Severe side effects are rare but can occur. These may include hypersensitivity reactions, such as anaphylaxis, which is a medical emergency requiring immediate attention. Signs of anaphylaxis include difficulty breathing, swelling of the face and throat, and severe rash. Patients with a known allergy to penicillins should avoid using Nafcillin Sodium due to the risk of cross-reactivity.
Nephrotoxicity is another potential severe side effect, particularly in patients with pre-existing kidney conditions or those receiving high doses of the drug. Symptoms of nephrotoxicity include changes in urine output, edema, and elevated blood urea nitrogen (BUN) and creatinine levels. It is essential to monitor kidney function regularly in patients receiving Nafcillin Sodium, especially those with underlying kidney issues.
Nafcillin Sodium can also cause liver toxicity, manifesting as elevated liver enzymes and, in rare cases, jaundice. Regular monitoring of liver function tests is recommended for patients on prolonged Nafcillin Sodium therapy. Other rare side effects include hematologic abnormalities such as neutropenia, thrombocytopenia, and eosinophilia.
Certain medications can interact with Nafcillin Sodium, potentially altering its effectiveness or increasing the risk of side effects. One of the most significant drug interactions occurs with warfarin, an anticoagulant. Nafcillin Sodium can enhance the metabolism of warfarin, reducing its anticoagulant effect and increasing the risk of thromboembolic events. It is crucial to monitor the International Normalized Ratio (INR) more frequently in patients taking both medications and adjust the warfarin dose as necessary.
Another notable interaction is with probenecid, a medication used to treat gout. Probenecid can inhibit the renal excretion of Nafcillin Sodium, leading to higher plasma levels of the antibiotic and an increased risk of toxicity. While this interaction can be used therapeutically to prolong the action of Nafcillin Sodium, it requires careful monitoring to avoid adverse effects.
Nafcillin Sodium may also interact with other beta-lactam antibiotics, such as cephalosporins and carbapenems, as well as with medications that affect renal function, such as diuretics and aminoglycosides. It is essential to review a patient's medication list thoroughly before initiating Nafcillin Sodium therapy to identify and manage potential drug interactions.
In conclusion, Nafcillin Sodium is a crucial antibiotic in the treatment of penicillinase-producing staphylococcal infections. Its penicillinase-resistant properties make it highly effective against resistant bacterial strains, and ongoing research continues to enhance our understanding of its use and efficacy. By understanding its mechanism of action, proper administration methods, potential side effects, and drug interactions, healthcare providers can optimize the therapeutic benefits of Nafcillin Sodium while minimizing risks to patients.
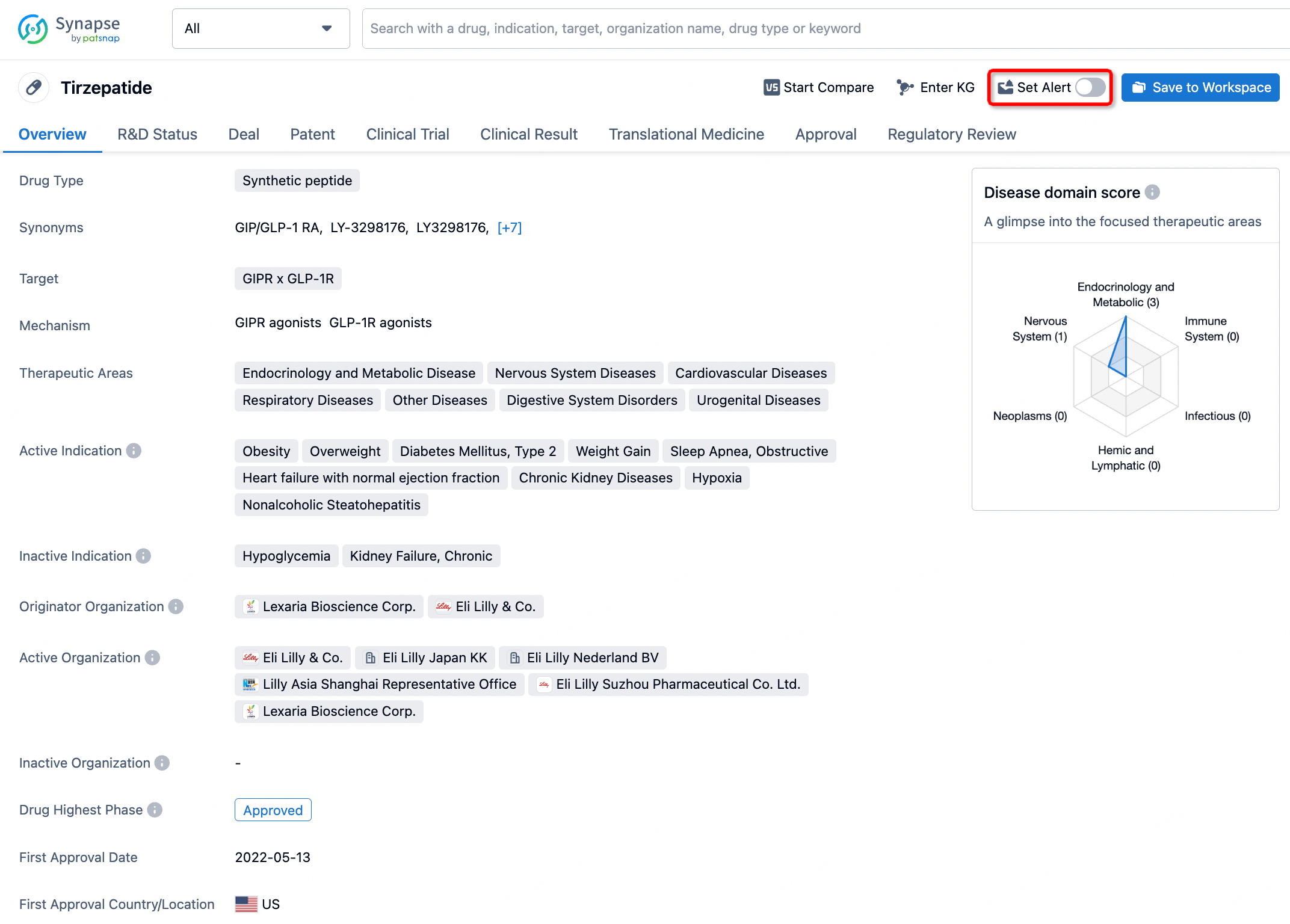
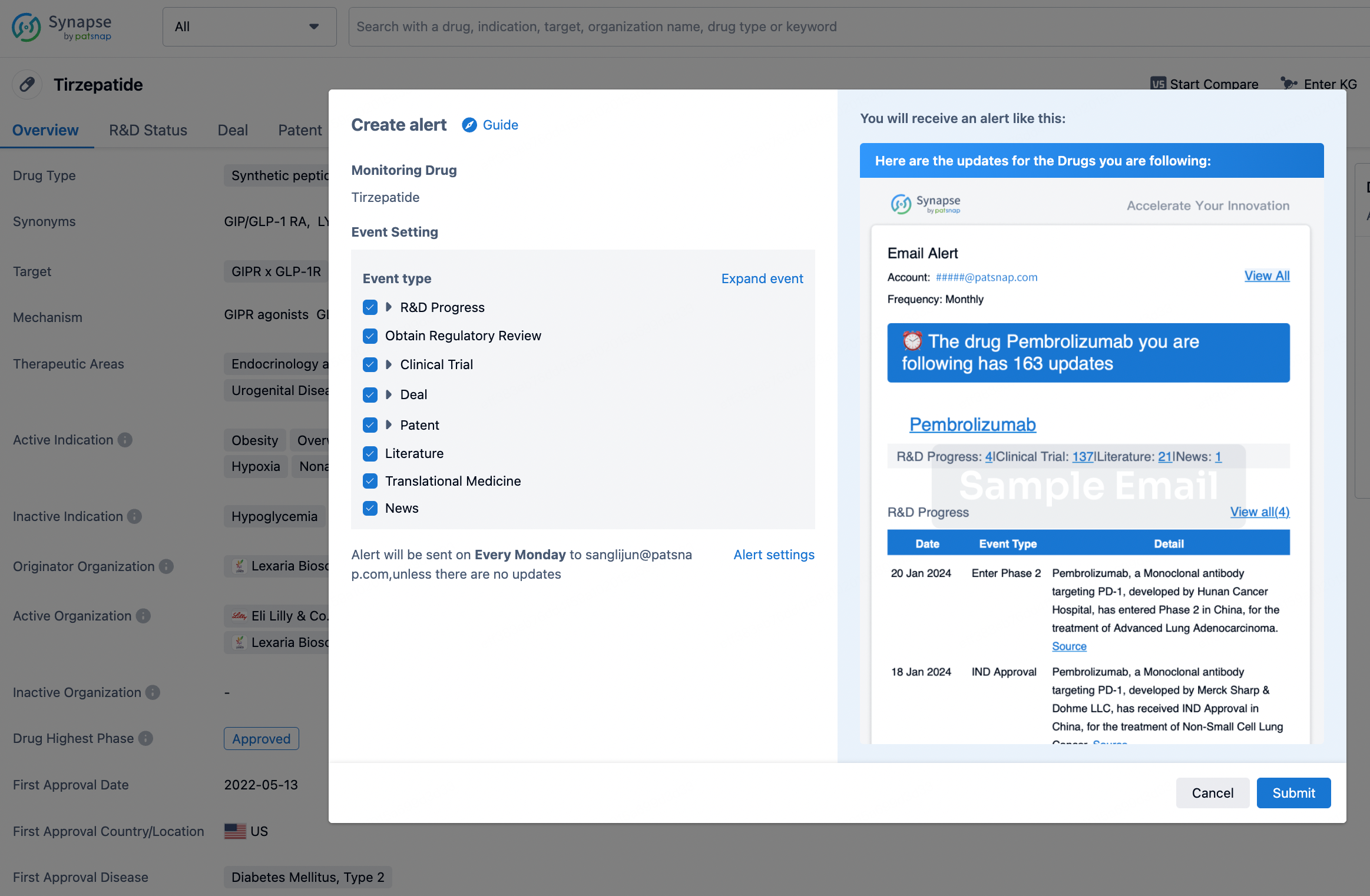
How to obtain the latest development progress of all drugs?
In the Synapse database, you can stay updated on the latest research and development advances of all drugs. This service is accessible anytime and anywhere, with updates available daily or weekly. Use the "Set Alert" function to stay informed. Click on the image below to embark on a brand new journey of drug discovery!
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.