Request Demo
What is Nimodipine used for?
15 June 2024
Nimodipine, a calcium channel blocker primarily used in the prevention and treatment of neurological conditions, is a medication with a fascinating history and significant clinical applications. Initially developed for managing hypertension, it is now primarily utilized for preventing cerebral vasospasm and the resultant ischemic deficits in patients suffering from subarachnoid hemorrhage. Marketed under various trade names, including Nimotop, Nimodip and Nymalize, nimodipine has carved out a unique niche in the medical landscape. Developed and researched extensively in institutions around the world, nimodipine continues to be a subject of clinical trials and studies, especially regarding its potential applications in other neurological disorders. This post aims to elucidate the specifics of nimodipine, including its mechanism of action, usage guidelines, side effects, and interactions with other drugs.
Nimodipine works primarily through its action as a calcium channel blocker, specifically targeting the L-type voltage-gated calcium channels found in the brain's smooth muscle cells. By inhibiting these channels, nimodipine reduces calcium influx into cells, which ultimately relaxes the smooth muscles of cerebral arteries. This vasodilation enhances blood flow to the brain, helping to alleviate the risks associated with cerebral vasospasm. Additionally, nimodipine has a high affinity for cerebral arteries over peripheral arteries, making it particularly effective in addressing conditions related to cerebral blood flow without significantly impacting systemic blood pressure. The neuroprotective effects of nimodipine have also been explored, suggesting potential benefits in treating conditions like traumatic brain injury and certain forms of dementia, although more research is needed to confirm these uses.
Nimodipine is typically administered orally, with patients usually taking the drug in tablet form. The standard dosage regimen recommends taking nimodipine every four hours, for a total of six doses per day. In the case of patients unable to swallow tablets, nimodipine can be administered via a nasogastric tube. It is critical to note that nimodipine should not be administered intravenously, as this can lead to severe hypotension and other cardiovascular complications. The onset of action for nimodipine is generally within 30 to 60 minutes, with peak plasma concentrations occurring approximately 1 to 2 hours post-ingestion. The drug's half-life is around 8 hours, necessitating frequent dosing to maintain therapeutic levels. Given its specific usage in subarachnoid hemorrhage, the treatment course usually extends for about 21 days to ensure comprehensive protection against vasospasm and subsequent ischemic events.
Like all medications, nimodipine comes with a range of potential side effects and contraindications that patients and healthcare providers should be aware of. Common side effects include hypotension, headache, nausea, and dizziness, often arising from its vasodilatory effects. Less common but more severe side effects may include bradycardia, palpitations, gastrointestinal disturbances, and an increased risk of bleeding. Because of the risk of severe hypotension, nimodipine is contraindicated in patients with existing severe hypotension, advanced heart failure, or in those who are concurrently taking other antihypertensive agents that could exacerbate this effect. Pregnant and nursing women should exercise caution and consult their healthcare provider before using nimodipine, as its safety in these populations has not been fully established. Furthermore, patients with liver impairment should be closely monitored due to the drug's metabolism in the liver, which could lead to elevated plasma levels and increased risk of adverse effects.
Interactions with other drugs are an important consideration when prescribing or using nimodipine. Calcium channel blockers can interact with various medications, potentially altering their efficacy or increasing the risk of adverse effects. For instance, concurrent use of nimodipine and other antihypertensive agents can amplify the blood-pressure-lowering effects, increasing the risk of severe hypotension. Additionally, drugs that inhibit the cytochrome P450 3A4 enzyme, such as certain antibiotics, antifungals, and antiretrovirals, can increase nimodipine plasma concentrations, potentially leading to toxicity. Conversely, drugs that induce the CYP3A4 enzyme, such as some anticonvulsants and rifampin, can decrease nimodipine levels, reducing its therapeutic efficacy. It is also crucial to avoid consuming grapefruit or grapefruit juice while taking nimodipine, as grapefruit can inhibit CYP3A4 and significantly elevate nimodipine levels. Patients should always inform their healthcare providers of all medications and supplements they are taking to avoid potential drug interactions.
In conclusion, nimodipine is a unique and valuable medication primarily used for preventing cerebral vasospasm in patients with subarachnoid hemorrhage. Its ability to selectively target cerebral arteries makes it particularly effective in this role while minimizing systemic side effects. However, like all medications, nimodipine requires careful administration and monitoring to avoid adverse effects and interactions with other drugs. Ongoing research continues to explore its potential applications in other neurological conditions, promising to further expand its clinical utility. For patients and healthcare providers, understanding the specifics of nimodipine's use, side effects, and drug interactions is essential for optimizing treatment outcomes and ensuring patient safety.
Nimodipine works primarily through its action as a calcium channel blocker, specifically targeting the L-type voltage-gated calcium channels found in the brain's smooth muscle cells. By inhibiting these channels, nimodipine reduces calcium influx into cells, which ultimately relaxes the smooth muscles of cerebral arteries. This vasodilation enhances blood flow to the brain, helping to alleviate the risks associated with cerebral vasospasm. Additionally, nimodipine has a high affinity for cerebral arteries over peripheral arteries, making it particularly effective in addressing conditions related to cerebral blood flow without significantly impacting systemic blood pressure. The neuroprotective effects of nimodipine have also been explored, suggesting potential benefits in treating conditions like traumatic brain injury and certain forms of dementia, although more research is needed to confirm these uses.
Nimodipine is typically administered orally, with patients usually taking the drug in tablet form. The standard dosage regimen recommends taking nimodipine every four hours, for a total of six doses per day. In the case of patients unable to swallow tablets, nimodipine can be administered via a nasogastric tube. It is critical to note that nimodipine should not be administered intravenously, as this can lead to severe hypotension and other cardiovascular complications. The onset of action for nimodipine is generally within 30 to 60 minutes, with peak plasma concentrations occurring approximately 1 to 2 hours post-ingestion. The drug's half-life is around 8 hours, necessitating frequent dosing to maintain therapeutic levels. Given its specific usage in subarachnoid hemorrhage, the treatment course usually extends for about 21 days to ensure comprehensive protection against vasospasm and subsequent ischemic events.
Like all medications, nimodipine comes with a range of potential side effects and contraindications that patients and healthcare providers should be aware of. Common side effects include hypotension, headache, nausea, and dizziness, often arising from its vasodilatory effects. Less common but more severe side effects may include bradycardia, palpitations, gastrointestinal disturbances, and an increased risk of bleeding. Because of the risk of severe hypotension, nimodipine is contraindicated in patients with existing severe hypotension, advanced heart failure, or in those who are concurrently taking other antihypertensive agents that could exacerbate this effect. Pregnant and nursing women should exercise caution and consult their healthcare provider before using nimodipine, as its safety in these populations has not been fully established. Furthermore, patients with liver impairment should be closely monitored due to the drug's metabolism in the liver, which could lead to elevated plasma levels and increased risk of adverse effects.
Interactions with other drugs are an important consideration when prescribing or using nimodipine. Calcium channel blockers can interact with various medications, potentially altering their efficacy or increasing the risk of adverse effects. For instance, concurrent use of nimodipine and other antihypertensive agents can amplify the blood-pressure-lowering effects, increasing the risk of severe hypotension. Additionally, drugs that inhibit the cytochrome P450 3A4 enzyme, such as certain antibiotics, antifungals, and antiretrovirals, can increase nimodipine plasma concentrations, potentially leading to toxicity. Conversely, drugs that induce the CYP3A4 enzyme, such as some anticonvulsants and rifampin, can decrease nimodipine levels, reducing its therapeutic efficacy. It is also crucial to avoid consuming grapefruit or grapefruit juice while taking nimodipine, as grapefruit can inhibit CYP3A4 and significantly elevate nimodipine levels. Patients should always inform their healthcare providers of all medications and supplements they are taking to avoid potential drug interactions.
In conclusion, nimodipine is a unique and valuable medication primarily used for preventing cerebral vasospasm in patients with subarachnoid hemorrhage. Its ability to selectively target cerebral arteries makes it particularly effective in this role while minimizing systemic side effects. However, like all medications, nimodipine requires careful administration and monitoring to avoid adverse effects and interactions with other drugs. Ongoing research continues to explore its potential applications in other neurological conditions, promising to further expand its clinical utility. For patients and healthcare providers, understanding the specifics of nimodipine's use, side effects, and drug interactions is essential for optimizing treatment outcomes and ensuring patient safety.
How to obtain the latest development progress of all drugs?
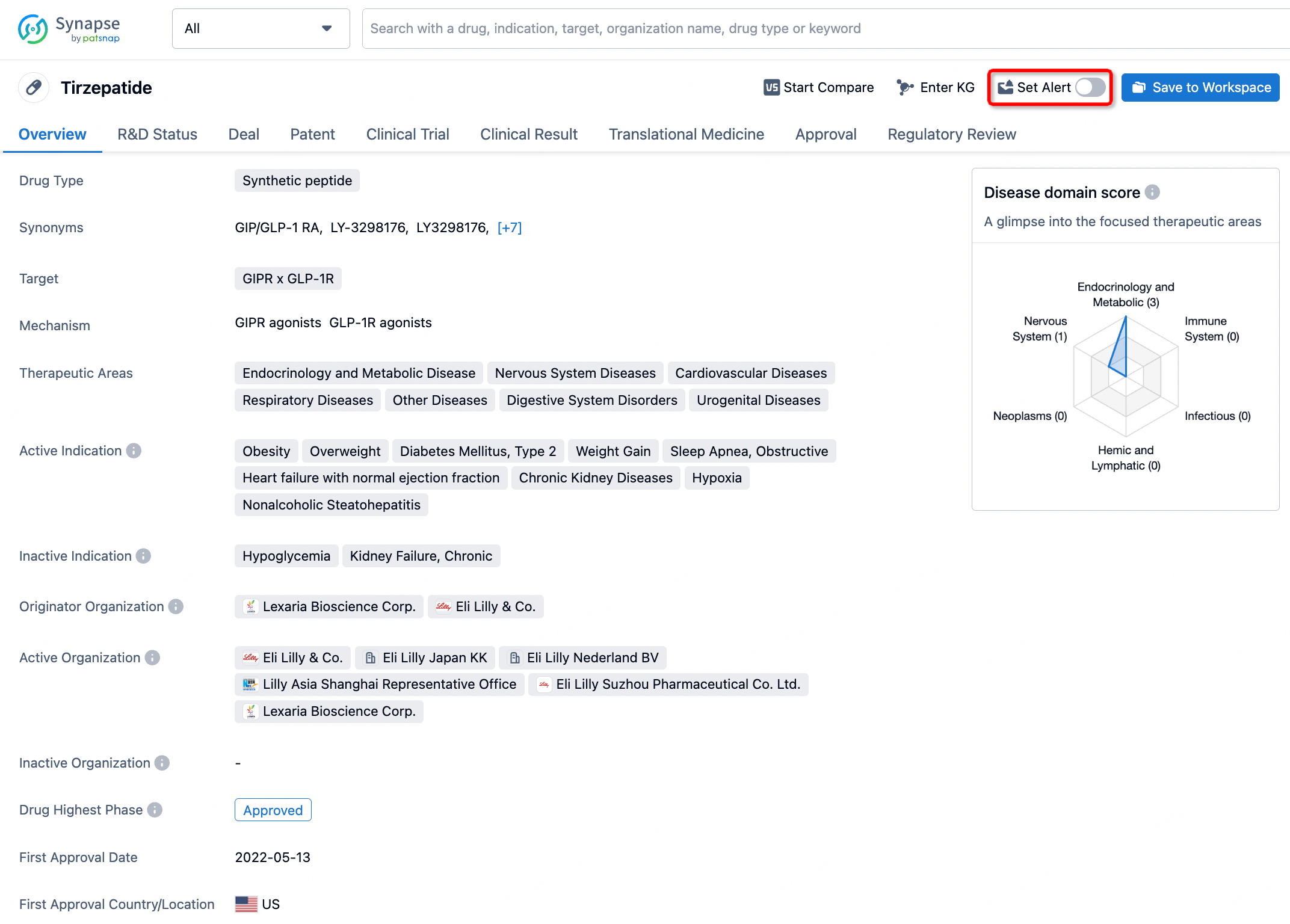
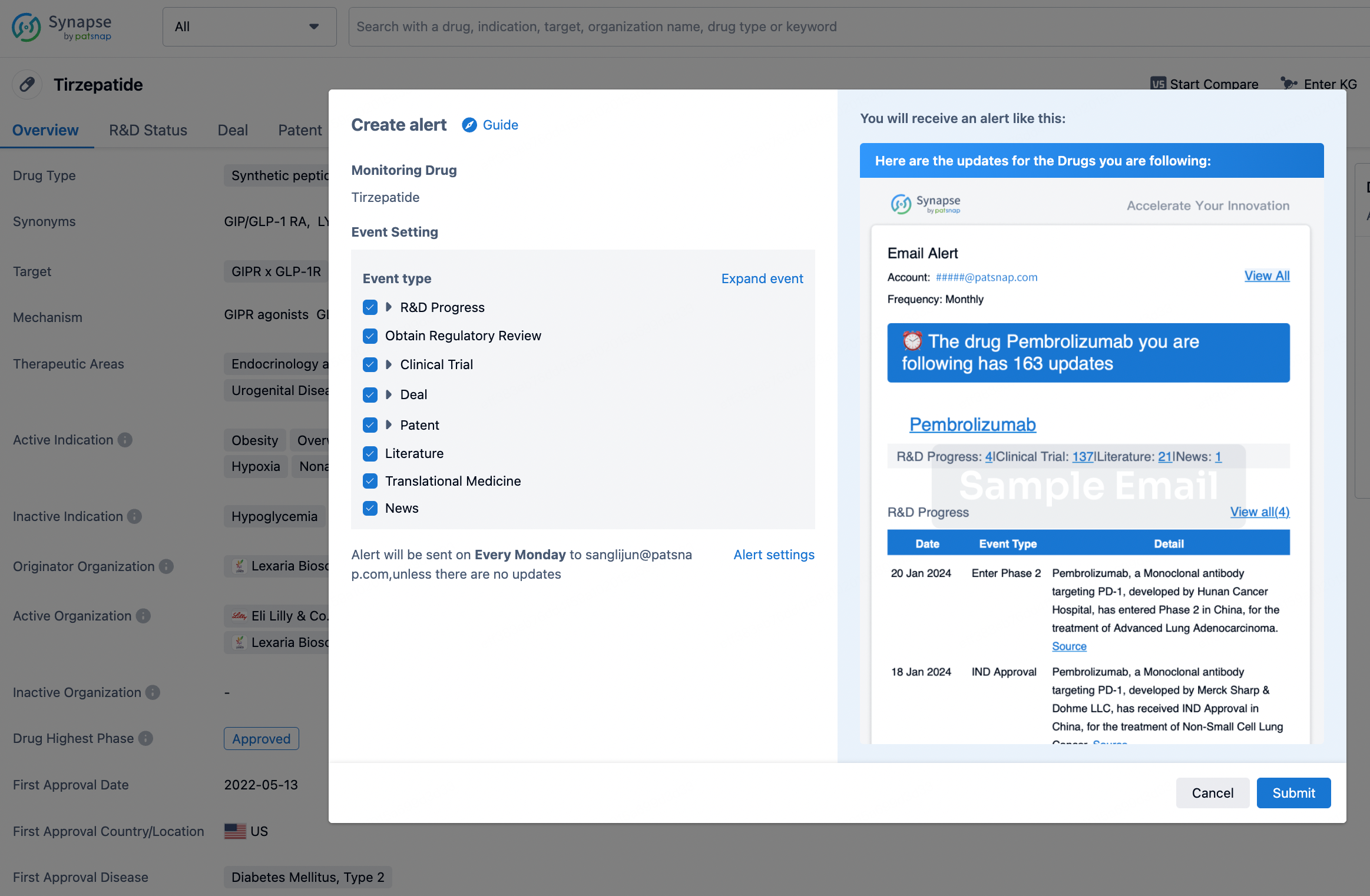
In the Synapse database, you can stay updated on the latest research and development advances of all drugs. This service is accessible anytime and anywhere, with updates available daily or weekly. Use the "Set Alert" function to stay informed. Click on the image below to embark on a brand new journey of drug discovery!
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.