Request Demo
What is Pentostatin used for?
14 June 2024
Pentostatin, also known by its trade name Nipent, is a purine nucleoside analog used primarily for the treatment of hairy cell leukemia (HCL). This chemotherapeutic agent is a potent inhibitor of adenosine deaminase, an enzyme crucial for the proliferation of lymphocytes. Initially discovered and developed by researchers at the National Cancer Institute, pentostatin has since become a pivotal part of the therapeutic regimen for patients suffering from various types of leukemia. Additionally, it has shown promise in treating other lymphoproliferative disorders such as chronic lymphocytic leukemia (CLL) and T-cell lymphomas.
Since its approval by the FDA in the early 1990s, pentostatin has undergone numerous clinical trials to explore its efficacy and safety profile. While it is not as widely known as other chemotherapeutic agents, its specific mechanism of targeting lymphoid malignancies has made it invaluable for certain patient populations. The ongoing research continues to investigate its potential in combination therapies, as well as its application in other oncological settings.
Pentostatin operates by inhibiting the enzyme adenosine deaminase, which plays a crucial role in purine metabolism. Adenosine deaminase is responsible for the deamination of adenosine and deoxyadenosine, converting them into inosine and deoxyinosine, respectively. Inhibition of this enzyme leads to an accumulation of adenosine and deoxyadenosine, particularly in lymphocytes.
The accumulation of deoxyadenosine triphosphate (dATP) interferes with DNA synthesis and repair. dATP acts as an inhibitor of ribonucleotide reductase, an enzyme essential for the production of deoxyribonucleotides from ribonucleotides. This inhibition disrupts the balance of deoxynucleotide pools required for DNA synthesis, leading to increased DNA strand breaks and apoptosis of rapidly dividing cells, such as malignant lymphocytes.
By specifically targeting the enzyme adenosine deaminase, pentostatin is able to selectively induce apoptosis in lymphoid cells without significantly affecting other cell types. This specificity is particularly beneficial in treating diseases like HCL, where the malignant cells are predominantly of lymphoid origin.
Pentostatin is typically administered intravenously, often in an outpatient setting. The standard dosage involves a 4 mg/m² intravenous infusion given every other week. The duration of the infusion is generally around 20 to 30 minutes, ensuring that the drug is delivered efficiently and safely into the bloodstream.
The onset of action for pentostatin can vary depending on the individual patient and the type of leukemia being treated. In cases of HCL, clinical responses are often observed within a few weeks to a few months of initiating therapy. For other types of lymphoid malignancies, the timeline may differ, and close monitoring by healthcare providers is essential to assess the drug's efficacy and adjust the treatment regimen as necessary.
Patients receiving pentostatin should adhere strictly to the prescribed dosage and schedule, as deviations can affect the drug's therapeutic outcomes. Regular blood tests and medical examinations are critical to monitor the patient's response to treatment and to detect any potential adverse effects early on.
While pentostatin is effective in treating certain types of leukemia, it is not without its side effects. Common adverse reactions include myelosuppression, which can lead to anemia, neutropenia, and thrombocytopenia. These conditions increase the risk of infections and bleeding, necessitating vigilant monitoring of blood counts and appropriate supportive care measures.
Other side effects may include nausea, vomiting, rash, fatigue, and liver enzyme abnormalities. Due to its immunosuppressive effects, patients may also experience a higher susceptibility to infections, making infection prophylaxis and prompt treatment of any infections crucial components of patient care.
Contraindications for pentostatin use include severe renal impairment, as the drug is primarily excreted by the kidneys. Patients with significant renal dysfunction may accumulate the drug to toxic levels, leading to severe adverse effects. Additionally, pentostatin should not be used concurrently with fludarabine, another purine analog, due to the increased risk of severe pulmonary toxicity and potential fatality.
Pentostatin can interact with several other medications, which may alter its efficacy or increase the risk of adverse effects. For instance, concomitant use of pentostatin and allopurinol, a drug used to manage hyperuricemia and gout, can exacerbate toxicity. Allopurinol inhibits xanthine oxidase, an enzyme involved in the metabolism of purines, potentially leading to increased levels of pentostatin and heightened risk of side effects.
Additionally, immunosuppressive agents such as corticosteroids and other chemotherapeutic drugs can compound the immunosuppressive effects of pentostatin, elevating the risk of infections and hematologic complications. Medications that affect renal function, such as nonsteroidal anti-inflammatory drugs (NSAIDs) and certain antibiotics, can alter the clearance of pentostatin, necessitating careful dose adjustments and monitoring.
Patients should inform their healthcare providers of all medications they are taking, including over-the-counter drugs, supplements, and herbal products, to ensure that potential drug interactions are identified and managed appropriately. This comprehensive approach is essential to maximize the therapeutic benefits of pentostatin while minimizing the risk of adverse effects and drug interactions.
Since its approval by the FDA in the early 1990s, pentostatin has undergone numerous clinical trials to explore its efficacy and safety profile. While it is not as widely known as other chemotherapeutic agents, its specific mechanism of targeting lymphoid malignancies has made it invaluable for certain patient populations. The ongoing research continues to investigate its potential in combination therapies, as well as its application in other oncological settings.
Pentostatin operates by inhibiting the enzyme adenosine deaminase, which plays a crucial role in purine metabolism. Adenosine deaminase is responsible for the deamination of adenosine and deoxyadenosine, converting them into inosine and deoxyinosine, respectively. Inhibition of this enzyme leads to an accumulation of adenosine and deoxyadenosine, particularly in lymphocytes.
The accumulation of deoxyadenosine triphosphate (dATP) interferes with DNA synthesis and repair. dATP acts as an inhibitor of ribonucleotide reductase, an enzyme essential for the production of deoxyribonucleotides from ribonucleotides. This inhibition disrupts the balance of deoxynucleotide pools required for DNA synthesis, leading to increased DNA strand breaks and apoptosis of rapidly dividing cells, such as malignant lymphocytes.
By specifically targeting the enzyme adenosine deaminase, pentostatin is able to selectively induce apoptosis in lymphoid cells without significantly affecting other cell types. This specificity is particularly beneficial in treating diseases like HCL, where the malignant cells are predominantly of lymphoid origin.
Pentostatin is typically administered intravenously, often in an outpatient setting. The standard dosage involves a 4 mg/m² intravenous infusion given every other week. The duration of the infusion is generally around 20 to 30 minutes, ensuring that the drug is delivered efficiently and safely into the bloodstream.
The onset of action for pentostatin can vary depending on the individual patient and the type of leukemia being treated. In cases of HCL, clinical responses are often observed within a few weeks to a few months of initiating therapy. For other types of lymphoid malignancies, the timeline may differ, and close monitoring by healthcare providers is essential to assess the drug's efficacy and adjust the treatment regimen as necessary.
Patients receiving pentostatin should adhere strictly to the prescribed dosage and schedule, as deviations can affect the drug's therapeutic outcomes. Regular blood tests and medical examinations are critical to monitor the patient's response to treatment and to detect any potential adverse effects early on.
While pentostatin is effective in treating certain types of leukemia, it is not without its side effects. Common adverse reactions include myelosuppression, which can lead to anemia, neutropenia, and thrombocytopenia. These conditions increase the risk of infections and bleeding, necessitating vigilant monitoring of blood counts and appropriate supportive care measures.
Other side effects may include nausea, vomiting, rash, fatigue, and liver enzyme abnormalities. Due to its immunosuppressive effects, patients may also experience a higher susceptibility to infections, making infection prophylaxis and prompt treatment of any infections crucial components of patient care.
Contraindications for pentostatin use include severe renal impairment, as the drug is primarily excreted by the kidneys. Patients with significant renal dysfunction may accumulate the drug to toxic levels, leading to severe adverse effects. Additionally, pentostatin should not be used concurrently with fludarabine, another purine analog, due to the increased risk of severe pulmonary toxicity and potential fatality.
Pentostatin can interact with several other medications, which may alter its efficacy or increase the risk of adverse effects. For instance, concomitant use of pentostatin and allopurinol, a drug used to manage hyperuricemia and gout, can exacerbate toxicity. Allopurinol inhibits xanthine oxidase, an enzyme involved in the metabolism of purines, potentially leading to increased levels of pentostatin and heightened risk of side effects.
Additionally, immunosuppressive agents such as corticosteroids and other chemotherapeutic drugs can compound the immunosuppressive effects of pentostatin, elevating the risk of infections and hematologic complications. Medications that affect renal function, such as nonsteroidal anti-inflammatory drugs (NSAIDs) and certain antibiotics, can alter the clearance of pentostatin, necessitating careful dose adjustments and monitoring.
Patients should inform their healthcare providers of all medications they are taking, including over-the-counter drugs, supplements, and herbal products, to ensure that potential drug interactions are identified and managed appropriately. This comprehensive approach is essential to maximize the therapeutic benefits of pentostatin while minimizing the risk of adverse effects and drug interactions.
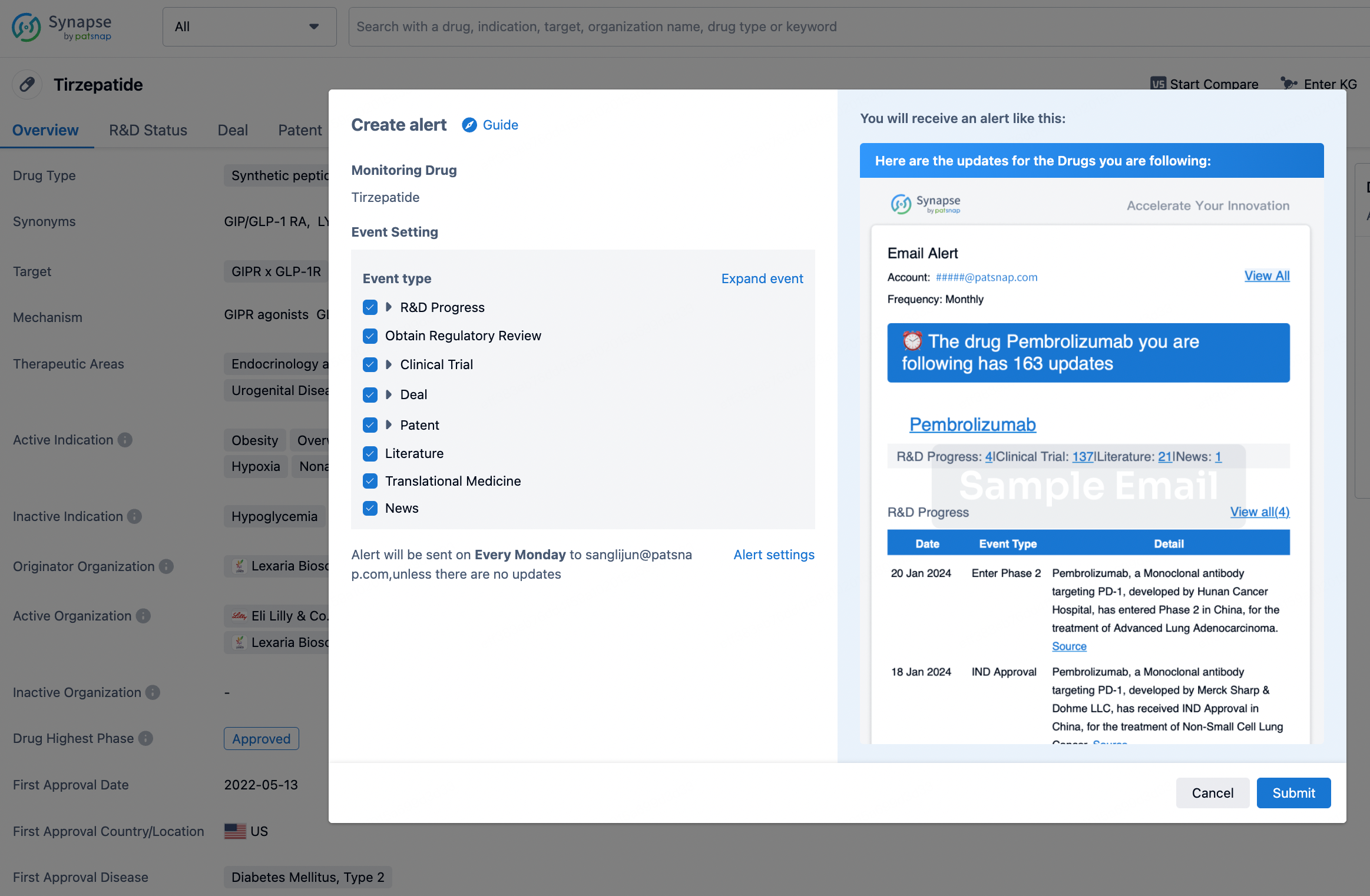
How to obtain the latest development progress of all drugs?
In the Synapse database, you can stay updated on the latest research and development advances of all drugs. This service is accessible anytime and anywhere, with updates available daily or weekly. Use the "Set Alert" function to stay informed. Click on the image below to embark on a brand new journey of drug discovery!
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.