Request Demo
Last update 30 May 2026
IL-2(Shanghai Xinshengyuan Biological Medicine Co. Ltd.)
Last update 30 May 2026
Overview
Basic Info
Drug Type Interleukins |
Synonyms- |
Target |
Action agonists |
Mechanism IL-2R agonists(Interleukin-2 receptor agonists) |
Therapeutic Areas |
Active Indication- |
Inactive Indication |
Originator Organization |
Active Organization- |
Inactive Organization |
License Organization- |
Drug Highest PhaseDiscontinuedClinical |
First Approval Date- |
Regulation- |
Related
100 Clinical Results associated with IL-2(Shanghai Xinshengyuan Biological Medicine Co. Ltd.)
Login to view more data
100 Translational Medicine associated with IL-2(Shanghai Xinshengyuan Biological Medicine Co. Ltd.)
Login to view more data
100 Patents (Medical) associated with IL-2(Shanghai Xinshengyuan Biological Medicine Co. Ltd.)
Login to view more data
12,710
Literatures (Medical) associated with IL-2(Shanghai Xinshengyuan Biological Medicine Co. Ltd.)01 Dec 2026·Blood Research
STING-Dependent spontaneous platelet adhesion potentiates NK cell proinflammatory responses in pediatric crohn’s disease
Article
Author: Xu, Xu ; Yu, Yi ; Wang, Xinqiong ; Wang, Junqi ; Xu, Chundi ; Li, Jia ; Lv, Jiajia ; Zhang, Meng ; Xiao, Yuan ; Cao, Wei
BACKGROUND:
Platelets are hypothesized to participate in the pathogenesis of Crohn's disease (CD) by interacting with other inflammatory cells such as natural killer (NK) cells. In this study, we aimed to evaluate the effects of platelet-NK cell interactions, both in vitro and in vivo, along with the corresponding mechanisms.
METHODS:
Clinical data were collected from patients with CD and IL-10 receptor alpha (IL-10RA) mutations, with the control group being comprised of patients with functional abdominal pain. Platelets and NK cells from the patients' colon tissues were immunostained. Dextran sulfate sodium (DSS)-induced colitis models using wild type (WT) and Stimulator of Interferon Genes knockout (STING-/-) mice were evaluated. Both purified CD41+ and CD41-NK cells were cultured with IL-2 and STING inhibitor C-176 to determine in vitro cell proliferation and Type 3 (T3) cytokine expression. Flow cytometry, enzyme-linked immunosorbent assays, and RT-PCR were used to assess the expression of CD41, IL-17, and adhesion-related molecules in mouse and human NK cells.
RESULTS:
Circulating and intestinal platelets were higher in patients with IL-10RA mutations compared to CD patients and correlated positively with serum cytokines, fecal calprotectin (FCP), and blood NK cells. Gut inflammation and T3 cytokine expression in NK cells were significantly lower in STING-/- mice compared to WT mice. Platelet-adherent NK cells showed significant proliferation and enhanced T3 cytokine expression, whereas STING inhibition markedly suppressed platelet adhesion, cell proliferation, and T3 cytokine expression. The naïve lung tissue of mice also displayed similar platelet-NK cell interactions. Platelet adhesion on NK cells led to higher CD24 expression compared to CD41-NK cells and we observed relatively higher CD24 in the NK cells from patients with IL-10RA mutations compared to patients with CD.
CONCLUSIONS:
Spontaneous platelet adhesion via STING signaling potentiates NK cell proinflammatory response in CD.
01 Jul 2026·EUROPEAN JOURNAL OF MEDICINAL CHEMISTRY
Novel design of interleukin-2 derivatives with reversed pH and potent antitumor activity
Article
Author: Yi, Juntao ; Liu, Yu ; Wang, Zhaofeng ; Zhang, Yunxiao ; Zhao, Wenjie ; Hao, Xinlong ; Liu, Qiuyue ; Peng, Dezheng ; Tang, Dongfang ; Zheng, Yuzhou ; Zhong, Guyu
Interleukin-2 (IL-2) displays high affinity for IL-2Rα at physiological pH, but low affinity in the acidic tumor microenvironment (TME), which brings side effects and reduces anti-tumor activity. This pH-dependent affinity modulation is attributed to protonation/deprotonation states of key acidic and basic amino acid residues within their binding interface, significantly impacting complex formation. Therefore, we designed three classes of IL-2 derivatives via a single-step process combining protein oxidative refolding and site-specific cysteine modification using the four prepared redox pairs based on IL-2(K64C). Surface plasmon resonance screening identified ZAP-IL-2(K64C) and Ac-TSAP-IL-2(K64C) derivatives with lower affinity for IL-2Rα at physiological pH and higher affinity under acidic TME conditions. Furthermore, toxicity assessment demonstrated that the pH-reversed IL-2 derivatives significantly mitigated the severe side effects associated with wild-type (wt) IL-2. In anti-tumor efficacy studies, the pH-reversed IL-2 derivatives demonstrated superior efficacy compared to wt IL-2, achieving a 50% tumor inhibition rate (TIR) versus 35% for wt IL-2 monotherapy. Strikingly, combination therapy with the pH-reversed IL-2 derivatives and the anti-PD-1 elicited a significant synergistic effect, further elevating the TIR to 85%. Our study provides a promising strategy for developing next-generation IL-2 therapeutics characterized by enhanced efficacy and reduced toxicity.
05 Jun 2026·BRITISH JOURNAL OF CANCER
Tumour-infiltrating lymphocyte therapy in melanoma: ready for prime time?
Review
Author: Lorigan, Paul ; Oudit, Deemesh ; Abdulgawad, Ahmed ; Lim, Kok Haw Jonathan ; Thistlethwaite, Fiona ; Woodford, Rachel
Abstract:
Tumour infiltrating lymphocyte (TIL) therapy offers the potential for durable clinical benefit in select patients with advanced melanoma, especially after progression on treatment with immune checkpoint inhibitors and/or targeted therapies. The 2024 FDA approval of Lifileucel (Amtagvi), a commercially manufactured autologous TIL product, marks a key milestone in integrating advanced therapy medicinal products (ATMPs) into routine care for solid tumours. Health Canada has since approved Lifileucel, with regulatory and funding decisions across the UK and Europe still pending. In this Perspective, we review the evidence base and outline key considerations for national adoption of TIL therapy. Despite promising results from clinical trials, TIL therapy requires complex coordination, including patient selection, tumour procurement, manufacturing logistics, lymphodepletion, and IL-2 administration; all contingent on specialised infrastructure and well-considered integrated care pathways. While commercial centralisation may ease logistical barriers, the high cost of TIL therapy necessitates careful health economic evaluation. A nationally coordinated effort is required to harmonise clinical prioritisation strategies, maintain oversight by multidisciplinary specialist tumour boards, and consider investment in future-proof decentralised manufacturing capacity. Collaborations and peer support such as through the Advanced Therapy Treatment Centre (ATTC) Network will facilitate phased, experience-led rollout with equity-focused service design.
5
News (Medical) associated with IL-2(Shanghai Xinshengyuan Biological Medicine Co. Ltd.)16 Apr 2026
AGOURA HILLS, Calif., April 16, 2026 (GLOBE NEWSWIRE) -- Oncotelic Therapeutics, Inc. (OTCQB:OTLC) (“Oncotelic”, the “Company” or “We”), a clinical-stage biopharmaceutical company developing drugs for the treatment of orphan oncology indications, as well as antisense and small molecule injectable drugs for the treatment of cancer, today announced its financial results for the fiscal year ended December 31, 2025 (“FY 2025”), as compared to the fiscal year ended December 31, 2024 (“FY 2024”). The financial results are based on the 2025 Annual Report on Form 10-K (“Form 10-K”) as filed with the Securities and Exchange Commission (“SEC”) on April 15, 2026. The Company recorded net income after tax of approximately $249.0 million, compared to a net loss of approximately $4.8 million in the prior year. The net income was primarily driven by a non-cash increase in the estimated fair value of the Company’s investment in GMP Biotechnology Limited (“GMP Bio”), its joint venture (“JV”), of approximately $365.4 million, as determined by an independent third-party ASC-compliant valuation, partially offset by a deferred income tax provision of approximately $111.6 million. Highlights for FY 2025 and thereafter: 2025 marked a transformational year for Oncotelic, highlighted by the successful completion of its first combination immunotherapy trial, the formalization of Sapu Bio and Sapu Nano, subsidiaries of GMP Bio, in which the Company has 45% equity interests. Additional achievements included dedicated development platforms, expansion of the Company’s AI-enabled research capabilities, and continued advancement of its joint venture programs. Joint Venture Valuation and Investment In November 2025, the Company recorded a non-cash increase in the fair value of its investment in GMP Biotechnology Limited based on an independent third-party valuation, resulting in a gain of approximately $365.4 million and a carrying value of approximately $388.0 million. This increase reflects estimated development progress and market-based assumptions and does not represent product revenue or cash received. A corresponding deferred income tax liability of approximately $111.6 million was recorded. Sapu Bio and Sapu Nano: Dual-Platform Strategy During 2025, GMP Bio formalized its two primary subsidiaries. Sapu Bio concentrates on OT-101 (TGFβ2 antisense) clinical development, regulatory advancement, and biomarker-driven positioning. Sapu Nano serves as the dedicated nanomedicine arm of the JV, advancing the Deciparticle™ platform into clinical-stage assets, partnerships, and commercialization. Together they form a diversified and scalable development platform. Deciparticle™ Nanoparticle Platform The Deciparticle™ platform utilizes ultra-small amphiphilic constructs (below ~20 nanometers) enabling enhanced tumor penetration and distribution. The JV is advancing six candidates: Sapu-001 (paclitaxel), Sapu-003 (everolimus), Sapu-004 (carboplatin), Sapu-005 (palbociclib), and Sapu-006 (docetaxel), in addition to OT-101. Everolimus formulation development is complete with a global clinical trial enrolling in Australia. Palbociclib and docetaxel INDs are expected in 2026. The platform is protected by more than 15 patent families. OT-101 Clinical Program In March 2025, we completed a Phase 1 clinical trial (NCT04862767) evaluating OT-101 in combination with IL-2 in Seoul, South Korea for advanced or metastatic solid tumors. The combination showed a tolerable safety profile with no unexpected safety signals. The JV plans to advance OT-101 plus IL-2 into further studies exploring synergies with checkpoint inhibitors such as PD-1 blockers. Separately, the JV initiated a Phase 2/3 trial for OT-101 in pancreatic cancer and is actively enrolling participants. Over ten patent families have been filed related to TGFβ2 as a prognostic indicator for cancer survival. PDAOAI (“AI”) Platform PDAOAI, the Company’s proprietary AI-enabled knowledge platform, was significantly expanded during 2025 into a core infrastructure layer supporting research, biomarker discovery, and regulatory documentation. By late 2025, PDAOAI evolved into a large-scale knowledge platform built around a TGF-β-centric biomedical corpus of over 100,000 curated abstracts with semantic retrieval and cross-referencing capabilities. PDAOAI contributed to at least seven peer-reviewed publications during 2025 across biomarker discovery, tumor microenvironment analysis, nanoparticle drug delivery, and clinical outcome correlations — spanning ovarian, breast, pancreatic, hepatocellular, and glioblastoma tumor types. Notably, the Company identified a novel biomarker signature (High RICTOR / Low RPTOR) predictive of sensitivity to intravenous everolimus based on analysis of over 9,000 tumor samples. GMP Manufacturing Facility The JV’s GMP manufacturing facility in San Diego continued full-scale operations during 2025 under its Drug Manufacturing License from the State of California. The facility utilizes a streamlined “one-pot” manufacturing process for bulk drug production through to finished product, with capabilities for both nonclinical and Phase 1 clinical trial material production. In early 2025, the Company partnered with Shanghai Medicilon, Inc. to access its rapid IND development platform supporting up to 20 IND projects. Results of Operations Below is a presentation of our financial results comparing FY 2025 to FY 2024 and based on our results published in our Form 10-K filed with the SEC on April 15, 2026. FY 2025 compared to FY 2024 Financial Results Overview ONCOTELIC THERAPEUTICS, INC. AND SUBSIDIARIES CONSOLIDATED STATEMENTS OF OPERATIONS For the Year Ended December 31, 2025 2024
Operating expenses:
Research and development $4,357 $- General and administrative 3,182,242 376,013 Goodwill impairment (See note 2 and 3) - 3,200,000 Total operating expenses 3,186,599 3,576,013
Income/(Loss) from operations (3,186,599) (3,576,013)Other income (expense):
Change in fair value of investment in GMP Bio 365,346,775 - Interest expense, net (885,488) (857,723)Reimbursement for expenses - related party - 22,937 Change in fair value of derivative on debt 353,572 (280,402)Loss on debt conversion (1,058,976) (88,258)Miscellaneous income 5,631 - Total other income (expense) 363,761,514 (1,203,446)Net income (loss) before income taxes 360,574,915 (4,779,459)Provision for income taxes (111,550,000) - Net income (loss) after income taxes 249,024,915 (4,779,459)Net income (loss) before non-controlling interests 249,024,915 (4,779,459)Net loss attributable to non-controlling interests (254,917) (255,527)Net income (loss) attributable to Oncotelic Therapeutics, Inc. $249,279,832 $(4,523,932)
Basic net income (loss) per share attributable to common stock $0.59 $(0.01)Basic weighted average common stock outstanding 421,045,524 404,396,473
Basic and diluted net income (loss) per share attributable to common stock $0.59 $(0.01)Basic and diluted weighted average common stock outstanding 422,234,747 404,396,473
We recorded a higher net income per basic share of $0.59 for the year ended December 31, 2025, as compared to net loss per basic share of $0.01 for the year ended December 31, 2024. The Company had no product revenue for either period. We recorded net income of approximately $249.3 million attributable to Oncotelic Therapeutics, Inc. for the year ended December 31, 2025, compared to a net loss of approximately $4.5 million for the year ended December 31, 2024. The higher net income was primarily due to recording a non-cash increase in the estimated fair value of our investment in GMP Bio of approximately $365.3 million, based on an independent third-party ASC-compliant valuation. This non-cash gain was partially offset by a provision for deferred income taxes of approximately $111.6 million, higher general and administrative expenses of approximately $2.8 million primarily driven by stock-based compensation of approximately $2.4 million incurred for common stock and preferred stock issued in connection with services and approximately $0.2 million to settle litigation related to an ex-employee, higher loss on conversion of debt of approximately $1.0 million, partially offset by a favorable change in the value of derivatives on debt of approximately $0.6 million and lower interest expense of approximately $28 thousand. All operational costs associated with OT-101 and the nanoparticle platform are substantially covered by the JV, significantly reducing our direct financial burden until such time we make a determination to commence development of our own compounds. “The independent third-party valuation of our JV’s pipeline represents a significant milestone for the Company and validates the strategic investments we have made since forming the joint venture in 2022. With the successful completion of our Phase 1 OT-101/IL-2 combination trial, the advancement of six Deciparticle™ nanoparticle candidates into various stages of development, and the continued expansion of our PDAOAI platform which contributed to seven peer-reviewed publications this year, the underlying value drivers are tangible and progressing. We are now focused on the next phase of value realization — advancing the JV toward a potential Hong Kong IPO, pursuing a national exchange uplisting for the Company, and converting our pipeline progress into clinical and commercial milestones,” said Vuong Trieu, CEO of Oncotelic. “The progress made by the Company, through GMP Bio, the joint venture with Dragon, over such a short period of time is very impressive. We expect to continue to see significant progress and shareholder value creation by the Company through our ownership in GMP Bio,” said Amit Shah, CFO of Oncotelic. About Oncotelic Oncotelic (f/k/a Mateon Therapeutics, Inc.), was formed in the State of New York in 1988 as OXiGENE, Inc., was reincorporated in the State of Delaware in 1992, and changed its name to Mateon Therapeutics, Inc. in 2016, and Oncotelic Therapeutics, Inc. in November 2020. Oncotelic conducts business activities through Oncotelic and its wholly-owned subsidiaries, Oncotelic, Inc., a Delaware corporation, PointR Data, Inc. (“PointR”), a Delaware corporation, Pet2DAO, Inc., a Delaware corporation; and EdgePoint AI, Inc. (“Edgepoint”), a Delaware Corporation for which there are non-controlling interests, (Oncotelic, Oncotelic Inc., PointR, Pet2DAO and Edgepoint are collectively called the Company). The Company is currently developing OT-101, in addition to five additional compounds, for various cancers and COVID-19 through its joint venture GMP Bio, with Dragon, Artemisinin for COVID-19 and AI technologies for clinical development and manufacturing. In addition, GMP Bio is developing 5 additional nanoparticle compounds in the JV, which has the potential of significant revenues and value. The Company also acquired apomorphine for Parkinson’s Disease, erectile dysfunction and female sexual dysfunction. In addition, the Company is evaluating the further development of its product candidates OXi4503, as a treatment for acute myeloid leukemia and myelodysplastic syndromes, and CA4P, in combination with a checkpoint inhibitor for the treatment of advanced metastatic melanoma. The Company is also planning to address the animal health industry through Pet2DAO. Our principal corporate office is in the United States at 29397 Agoura Road, Suite 107, Agoura Hills, CA 91301 (telephone: 650-635-7000). Our internet address is www.oncotelic.com. Oncotelic’s Cautionary Note on Forward-Looking Statements Any statements contained in this Press Release that are not statements of historical fact are forward-looking statements. In some cases, you can identify forward-looking statements by terminology such as “may,” “will,” “should,” “expect,” “intend,” “plan,” “anticipate,” “believe,” “estimate,” “predict,” “potential,” “continue,” “assumption” or the negative of these terms or other comparable terminology. Statements concerning: our expectations on the timing, success of the JV’s product approvals, commercialization of the JVs products and results of operations of the JV: our expectations on the timing, success, or valuation our JV’s planned initial public offering; the timing, success or continuing valuation of our equity interest in the JV; our ability to secure future debt or equity financing needed to meet operating costs; the timing, costs and other limitations involved in obtaining regulatory approval for any product candidate; the expected efficacy of our product candidates compared to competitive products; anticipated results of our research and development programs as well as preclinical and clinical trials; expected market size, market acceptance for our product candidates; our ability to enter into future partnerships, joint ventures or other corporate transactions, ability of us being able to obtain additional resources, including debt or equity funding, and the expected benefits to be derived from those transactions; the anticipated impact of regulatory and legislative changes in the United States and foreign countries on our product candidates and operations; anticipated trends in revenues, operating expenses or financial position and results of operations; and our estimates regarding anticipated operating income or losses, future performance, future revenues and projected expense; are all forward-looking statements. Forward-looking statements reflect current views about future events and are based on our currently available financial, economic and competitive data and on current business plans. Forward-looking statements are not guarantees of future performance and our actual results may differ significantly from the results discussed or implied in the forward-looking statements. Factors that might cause such differences include, but are not limited to, the factors included in “Risk Factors,” in our Form 10K and the other registration statements and reports that we file with the SEC. The forward-looking statements contained in this press release are based on our current expectations and beliefs concerning future developments and their potential effects on us. We undertake no obligation to update or revise any forward- looking statements, whether as a result of new information, future events or otherwise, except as may be required under applicable securities laws. You should consider the inherent limitations on, and risks associated with, forward-looking statements and not unduly rely on the accuracy of predictions contained in such forward-looking statements. This press release may also include market data related to our business and industry. These market data may include projections that are based on a number of assumptions. While we believe these assumptions to be reasonable and sound as of the date of this press release, if these assumptions turn out to be incorrect, actual results may materially differ from the projections based on these assumptions. As a result, the markets for our product candidates may not grow at the rates projected by these data, or at all. The failure of these markets to grow at these projected rates may have a material adverse effect on our business, results of operations, financial condition and the market price of our common stock. In addition, the Company expects to remeasure the fair value of its investment in GMP Biotechnology Limited on a quarterly basis in accordance with applicable accounting standards, including Accounting Standards Codification (“ASC”) 820, Fair Value Measurement. Such remeasurements are based on significant estimates and assumptions, including clinical development progress, regulatory milestones, market conditions, and comparable company data. As a result, the value of this investment, and the corresponding impact on the Company’s financial statements, may fluctuate materially from period to period, including based on the success or failure of drug development activities within the joint venture pipeline. These fluctuations are non-cash in nature and may not be indicative of the Company’s underlying operating performance or future cash flows. Investor & Media ContactOncotelic Therapeutics, Inc.Investor Relationsir@oncotelic.com Corporate CommunicationsIBNAustin, Texaswww.InvestorBrandNetwork.com512.354.7000 OfficeEditor@InvestorBrandNetwork.com
Phase 1Financial Statement
24 Mar 2026
This case study demonstrates how DelveInsight supported an oncology-focused pharmaceutical client in assessing investment opportunities in IL-2 therapies. Through a comprehensive epidemiology-driven analysis spanning refractory cancers, autoimmune conditions, and inflammatory disorders, DelveInsight identified the addressable patient population, projected market trends across the 7MM through 2034, and uncovered critical treatment gaps.
LAS VEGAS, March 24, 2026 /PRNewswire/ -- In the rapidly evolving landscape of immunotherapy, precision patient segmentation is the cornerstone of successful drug development and market entry. A leading pharmaceutical company specializing in oncology turned to DelveInsight for actionable insights of IL-2 target patient pool and market forecast analysis to optimize investment strategies across multiple therapeutic domains. This analysis spans the 7MM (United States, EU4 [Germany, France, Italy, Spain], the United Kingdom, and Japan) with detailed projections extending through 2034, positioning stakeholders to capitalize on emerging opportunities in the IL-2 therapy space.
Unlock the complete IL-2 patient pool analysis case study:
The Challenge: Navigating a Fragmented and Complex IL-2 Market
The company faced a critical strategic decision, as IL-2-based therapies gained momentum across multiple disease indications, spanning refractory cancers, autoimmune diseases, and inflammatory conditions, the organization needed to assess investment viability with unprecedented precision. The existing data landscape was fragmented, lacking the epidemiological depth, patient segmentation granularity, and forward-looking forecasts required to support informed R&D prioritization and go-to-market strategy. The company's core requirements were multifaceted.
First, they required a detailed identification and segmentation of target patient populations across diverse IL-2-relevant indications in major markets.
Second, they needed robust market sizing and revenue projections segmented by indication and geography through 2034. Third, the organization sought a comprehensive competitive landscape evaluation to assess positioning relative to emerging IL-2 competitors and alternative therapeutic modalities.
Finally, they needed KOL insights and unmet medical need assessments to validate clinical development priorities and identify high-value therapeutic opportunities.
IL-2 Continues to Anchor Innovation in Immuno-Oncology
IL-2, one of the earliest immunotherapies to receive approval, continues to be an important component in the advancing landscape of immuno-oncology. The development of next-generation IL-2 variants, including modified forms such as pegylated IL-2, highlights its potential for sustained clinical relevance, particularly as a backbone therapy in combination treatment strategies.
Beyond oncology, IL-2 also demonstrates therapeutic promise across a range of other conditions, including autoimmune and inflammatory disorders. Its capacity to stimulate T-cell activation, promote the expansion of regulatory T cells, and modulate immune responses positions IL-2 as a versatile candidate for diseases where precise immune regulation is essential.
DelveInsight analysis yielded striking insights into the addressable patient population and market dynamics across the 7MM. Among all target indications, Atopic Dermatitis represented the largest patient pool, comprising approximately
39 million prevalent cases across the 7MM in 2024. Meanwhile, NSCLC emerged as the second major opportunity area, with millions of patients suffering from advanced disease amenable to IL-2-based therapeutic approaches.
Within specific geographies, notable patterns emerged. In the US market, Atopic Dermatitis dominated the IL-2 addressable population, while rarer indications such as Aplastic Anemia represented limited but critical unmet needs. Across EU4 and the UK, Germany accounted for the highest prevalence of Atopic Dermatitis-related cases, suggesting differential market entry priorities by indication and geography. These insights fundamentally shaped the client's indication prioritization strategy, directing R&D investment and clinical trial design toward the highest-potential segments.
Beyond epidemiological segmentation, DelveInsight constructed a forecasting model spanning 2020–2034, enabling the client to anticipate market evolution across multiple scenarios. The model integrated critical dynamics shaping the IL-2 landscape: demographic shifts and aging population trends, evolving smoking prevalence and lung cancer incidence, accelerating biomarker testing adoption across countries, and the rapid emergence of novel therapeutic modalities and combination approaches.
The quantitative findings underscored a substantial market opportunity. In 2023, the IL-2 market size across the 7MM was valued at approximately
USD 6 million, representing an early-stage but rapidly expanding therapeutic category. Notably, two indications, Atopic Dermatitis and NSCLC, emerged as the primary revenue drivers, expected to generate the most substantial market value by 2034 due to the highest level of clinical development activity and regulatory authorization trajectories.
Get the
Interleukin-2 Market Report to explore in-depth epidemiological insights, emerging trends, and strategic forecasts shaping the future of IL-2-based therapies.
DelveInsight's Multi-Dimensional Solution
To address the challenges, DelveInsight deployed a sophisticated, evidence-based analytical framework integrating multiple data streams and methodologies by providing
Epidemiology-driven analysis spanning twelve target indications: Non-Segmental Vitiligo (NSV), Aplastic Anemia, Amyotrophic Lateral Sclerosis (ALS), Peripheral T-cell lymphoma (PTCL), Cutaneous T-cell lymphoma (CTCL), Ovarian cancer, Head and neck squamous cell carcinoma (HNSCC), Melanoma, Atopic Dermatitis, Alopecia Areata, Non-small cell lung cancer (NSCLC), and Mucosal Melanoma.
Current IL-2 market size across the 7MM by therapeutic application and drug uptake, with forecasts through 2034 based on disease prevalence, emerging therapies, and evolving treatment guidelines.
List of key companies, including Mural Oncology, Nektar Therapeutics, Cue Biopharma, Anaveon, Corvus Pharmaceuticals, Philogen, Krystal Biotech, Innovent Biologics, and others, active in the IL-2 space, along with their pipelines, product portfolios, market presence, and competitive strategies to highlight differentiation opportunities.
Key unmet needs in treating refractory cancers, autoimmune, and inflammatory diseases, along with market growth drivers such as advancing IL-2 research and demand for personalized therapies.
Real-world evidence sourced from healthcare databases and patient registries, country-specific epidemiological data from cancer registries and regional health authorities, peer-reviewed scientific literature and meta-analyses, and primary qualitative research through structured interviews with KOLs spanning oncology, immunology, and dermatology.
Curious how DelveInsight's insights can shape your IL-2 strategy or biopharma investment decisions?
Request a proposal today to discover how our customized solutions can help achieve your strategic objectives
Competitive Intelligence Services Tailored to Oncology Domain
: DelveInsight's competitive intelligence services deliver real-time, precise insights across therapeutic domains, with oncology being one of our key areas of expertise. We provide in-depth analysis of advancements across both prevalent and rare conditions, including NSCLC, Melanoma, Ovarian Cancer, Head and Neck Squamous Cell Carcinoma, Pancreatic Cancer, Breast Cancer, Acute Myeloid Leukemia, and others. Our services track competitor pipelines, clinical trial progress, regulatory shifts, and patent landscapes, offering a comprehensive view of the evolving oncology market. By leveraging these insights, stakeholders can identify emerging threats, seize growth opportunities, and craft strategic moves to stay ahead in this dynamic space.
Rare Disease Consulting Services
: In the rare disease space, one of our fortes, we deliver intelligence that helps clients overcome the unique challenges of niche markets. Our analysts monitor global R&D progress, competitive developments, and shifting regulatory landscapes to provide tailored insights that guide product positioning and investment strategies. From in-depth conference evaluations to detailed competitor analyses, we help clients de-risk decision-making, strengthen portfolios, and efficiently advance therapies from development to market.
Epidemiology Database
: The AI-driven epidemiology database is an extensive repository that covers more than 500 disease indications and provides 10-year epidemiological forecasts across the seven major markets (the US, EU4, the UK, and Japan). It combines AI capabilities with validated, expert-curated epidemiology insights to help users gain a deeper understanding of disease burden, detailed epidemiological segmentation, and long-term trends across multiple indications and geographies. Built to support forecasting, portfolio strategy, and commercial decision-making, the platform offers actionable insights that strengthen data-driven planning for pharmaceutical and healthcare stakeholders.
Patient Pool Forecasting
: DelveInsight recognizes the complexities pharmaceutical and biotech companies face when estimating and selecting the most suitable patient segments for drug development. Making the right choice is crucial for optimizing outcomes while navigating challenges such as determining the appropriate line of therapy, minimizing patient burden, evaluating diagnostic impact, and projecting drug uptake. DelveInsight provides actionable insights and analytics to support these decisions, enabling companies to target patient populations with the greatest unmet needs, thereby enhancing clinical outcomes and streamlining drug development.
Pharma Consulting Services
: Our healthcare consulting services turn complex market data into actionable strategies for pharmaceutical, biotech, and medical device companies. We help clients uncover new revenue streams, assess market potential, and successfully navigate commercialization challenges. With deep expertise in clinical trial design, market intelligence, and strategic consulting, our team partners with clients to optimize decision-making, accelerate innovation pipelines, and improve business outcomes.
Schedule a call today to leverage our expertise and stay ahead in the competitive market
About
DelveInsight
DelveInsight is a leading Business Consultant and Market Research firm focused exclusively on life sciences. It supports pharma companies by providing comprehensive end-to-end solutions to improve their performance. Get hassle-free access to all the healthcare and pharma market research reports through our subscription-based platform PharmDelve
.
Contact Us
Shruti Thakur
[email protected]
+14699457679
Logo:
SOURCE DelveInsight Business Research, LLP
21%
more press release views with
Request a Demo
Immunotherapy
20 Jan 2026
HOUSTON--(BUSINESS WIRE)--Coya Therapeutics, Inc. (NASDAQ: COYA) (“Coya” or the “Company”), a clinical-stage biotechnology company developing biologics intended to enhance Treg function, releases the following letter to stockholders from Chief Executive Officer Dr. Arun Swaminathan.
Dear Fellow Stockholders,
Coya enters 2026 with strong momentum and a clear sense of purpose. I believe we are exceptionally well positioned to advance our mission of delivering potentially transformational therapies for patients suffering from devastating neurodegenerative diseases. Scientifically, the neurodegeneration field increasingly recognizes combination-based therapeutic strategies such as ours as a promising path forward for diseases driven by complex, multifactorial biology. Clinically, we are driving towards major clinical catalysts in ALS and FTD. We believe each program has the potential to meaningfully address unmet needs. Our studies are designed to evaluate whether combination-based regulatory T-cell modulation can stabilize or alter disease progression—an outcome that, if confirmed, would represent a significant advance for patients and a defining milestone for the Company. Moreover, we anticipate additional datasets in 2026 which we believe are poised to add to our body of work on Treg biology.
Operational and Regulatory Execution/Momentum
Last year we received two important IND approvals for COYA 302—one in Amyotrophic Lateral Sclerosis (ALS) and one in Frontotemporal Dementia (FTD). We have now initiated our ALSTARS trial in ALS. That study is advancing as planned. We are actively enrolling and patients are already being dosed. Recruitment has been further strengthened by acceptance of our Clinical Trial Application (CTA) by Health Canada, enabling the activation of Canadian sites in addition to more than 20 U.S. clinical sites.
Scientific Validation and Expanding Data Generation Built on Nobel Prize–Recognized Treg Biology
Our scientific approach continues to be validated at the highest levels. In 2025, the Nobel Prize in Physiology or Medicine was awarded to our Scientific Advisory Board member, Dr. Shimon Sakaguchi, for his pioneering work in elucidating regulatory T-cell (Treg) biology.
Importantly, across four investigator-initiated clinical studies of our combination-based regulatory T-cell (Treg) modulation approach, we have observed stabilization of disease progression in treated patient cohorts, including ALS and FTD. Stabilizing clinical progression in neurodegenerative diseases, historically characterized by relentless functional decline, is a clinically meaningful signal and reinforces our belief in the potential of Treg-targeted combination strategies to alter disease trajectory. While investigator-initiated studies are not confirmatory, these results suggest a potentially unifying mechanism in neurodegeneration. In sum, we believe these observations provide early clinical validation of our approach and underpin our confidence in advancing COYA 302 in the ALSTARS Trial and a prospective clinical study in patients with FTD. In addition, these observations also encourage our pursuit of later-stage development in other indications.
New Translational Datasets to be provided in 2026
During 2026 we plan to present further translational and clinical datasets across our programs, including biomarker, proteomics, and single-cell data. These data are expected to further elucidate the role of regulatory T cells in modulating neuroinflammation and neurodegeneration, while providing deeper insight into target engagement, pathway modulation, and patient-level biology. We believe these datasets will meaningfully strengthen the mechanistic foundation underlying our combination-based therapeutic approach and support future clinical, regulatory, and partnering discussions.
Financial Strength and Fiduciary Discipline
In 2025, we further strengthened our balance sheet, including the receipt of $8.4 million in non-dilutive funding from our strategic partner, Dr. Reddy’s Laboratories. We enter 2026 with approximately $46.8 million in cash (unaudited) as of 31st December 2025, no debt, and a projected cash runway into the second half of 2027—extending beyond the anticipated topline readout of the ALSTARS trial.
This financial position allows us to remain highly focused on execution while preserving strategic flexibility.
2026 Priorities and Clinical Programs
Our efforts in 2026 will be squarely focused on advancing our ALS and FTD programs toward key value-creating milestones.
COYA 302 in ALS
The ALSTARS Phase 2 trial is actively enrolling and dosing patients. Additional U.S. and Canadian sites are soon expected to come fully online. We are targeting full enrollment in the second half of 2026, with a topline data readout anticipated in the first quarter of 2027.
COYA 302 in FTD
Results from an investigator-initiated trial of low-dose IL-2 and CTLA4-Ig demonstrated robust target engagement, including statistically significant and sustained increases in regulatory T-cell numbers and suppressive function beginning as early as two weeks post-dosing and maintained through the 22-week treatment period. The cognitive measures were stable, with no decline on either the Montreal Cognitive Assessment (MoCA) or the CDR-FTLD.
These results support advancement of COYA 302 into a Phase 2a study in patients with FTD, for which we have received FDA clearance. As previously disclosed, the Alzheimer’s Drug Discovery Foundation invested $5 million in Coya based on its conviction in our combination-therapy approach. We are working closely with leading key opinion leaders and expect to initiate this study in the second quarter of 2026. Coya retains full global rights to this indication, which we believe represents a meaningful long-term value opportunity.
COYA 303 in Alzheimer’s Disease
COYA 303, our proprietary combination of low-dose IL-2 and a GLP-1 receptor agonist, has demonstrated compelling preclinical synergy across multiple biomarkers relevant to neurodegenerative disease. While recent Novo Nordisk EVOKE and EVOKE+ studies evaluating semaglutide monotherapy in mild Alzheimer’s disease did not show clinical efficacy, they did demonstrate some improvement in key biomarkers. We believe the synergy demonstrated from our in vitro and in vivo studies of our proprietary combination of low-dose IL-2 and a GLP-1 receptor agonist (COYA 303) may make this combination a viable approach in Alzheimer’s disease.
In 2026, we will continue to pursue capital-efficient strategies to advance this program, including strategic partnerships and non-dilutive funding opportunities.
Strategic Partnerships
Our collaboration with Dr. Reddy’s Laboratories continues to strengthen and provides substantial value beyond non-dilutive milestone payments. Our teams remain closely aligned in advancing the ALSTARS trial and preparing for potential future commercialization activities. We expect this partnership to deepen further in 2026.
We are also evaluating additional strategic opportunities. Japan represents a significant ALS market where we retain full rights, and we plan to advance discussions with potential partners accordingly. More broadly, as immunology and neuroscience increasingly converge, we see multiple opportunities to expand the reach of our platform through combination strategies and novel collaborations.
Looking Ahead
In summary, throughout 2026, Coya will be actively advancing two COYA 302 clinical programs: one in ALS and the other in FTD—two diseases with profound unmet medical need and an estimated combined market opportunity of $2–$4 billion. Our confidence is grounded in three pillars:
Highly validated science rooted in Nobel Prize–recognized discoveries in regulatory T-cell biology that established the central role of Tregs in immune homeostasis and the control of pathologic inflammation.
A combination based therapeutic strategy that targets multiple aspects of the immune system increases the probability of technical and regulatory success.
Consistent and encouraging clinical and translational data across multiple studies and indications, supplemented by the generation of additional translational biology datasets in 2026 that we anticipate will further elucidate the role of regulatory T cells in modulating neuroinflammation and neurodegeneration and support our mechanistic and clinical rationale.
With a strong balance sheet and runway extending beyond our next major clinical inflection point, we believe Coya is well positioned to execute on its strategy and deliver meaningful long-term value.
On behalf of the entire Coya team, thank you for your continued support and confidence. Our management team and board of directors are considerable shareholders along with you, aligning our collective interests. We only win if you win. We are deeply grateful to our employees, investigators, clinical partners, and—most importantly—the patients and families who make our work possible. We look forward to updating you on our continued progress throughout the year.
Sincerely yours,
Arun Swaminathan, Ph.D.
Chief Executive Officer
Coya Therapeutics, Inc.
About Coya Therapeutics, Inc.
Headquartered in Houston, TX, Coya Therapeutics, Inc. (Nasdaq: COYA) is a clinical-stage biotechnology company developing proprietary treatments focused on the biology and potential therapeutic advantages of regulatory T cells (“Tregs”) to target systemic inflammation and neuroinflammation. Dysfunctional Tregs underlie numerous conditions, including neurodegenerative, metabolic, and autoimmune diseases. This cellular dysfunction may lead to sustained inflammation and oxidative stress resulting in lack of homeostasis of the immune system.
Coya’s investigational product candidate pipeline leverages multiple therapeutic modalities aimed at restoring the anti-inflammatory and immunomodulatory functions of Tregs. Coya’s therapeutic platforms include Treg-enhancing biologics, Treg-derived exosomes, and autologous Treg cell therapy.
For more information about Coya, please visit www.coyatherapeutics.com
About COYA 302
COYA 302 is an investigational and proprietary biologic combination therapy with a dual immunomodulatory mechanism of action intended to enhance the anti-inflammatory function of regulatory T cells (Tregs) and suppress the inflammation produced by activated monocytes and macrophages. COYA 302 comprises proprietary low dose interleukin-2 (LD IL-2) and CTLA-4 Ig and is being developed for subcutaneous administration for the treatment of patients with ALS and other neurodegenerative diseases. These mechanisms may have additive or synergistic effects.
Coya is currently conducting the ALSTARS Trial, a Phase 2, randomized, multi-center, double-blind, placebo-controlled study to evaluate the efficacy and safety of COYA 302 for the treatment of ALS (ClinicalTrials.gov Identifier: NCT 07161999).
COYA 302 is an investigational product not yet approved by the FDA or any other regulatory agency.
Forward-Looking Statements
This press release contains “forward-looking” statements that are based on our management’s beliefs and assumptions and on information currently available to management. Forward-looking statements include all statements other than statements of historical fact contained in this presentation, including information concerning our current and future financial performance, business plans and objectives, current and future clinical and preclinical development activities, timing and success of our ongoing and planned clinical trials and related data, the timing of announcements, updates and results of our clinical trials and related data, our ability to obtain and maintain regulatory approval, the potential therapeutic benefits and economic value of our product candidates, competitive position, our anticipated cash runway, industry environment and potential market opportunities. The words “believe,” “may,” “will,” “estimate,” “continue,” “anticipate,” “intend,” “expect,” and similar expressions are intended to identify forward-looking statements.
Forward-looking statements are subject to known and unknown risks, uncertainties, assumptions and other factors including, but not limited to, those related to risks associated with the success, cost and timing of our product candidate development activities and ongoing and planned clinical trials; our plans to develop and commercialize targeted therapeutics; the progress and timing of patient enrollment and dosing in our preclinical or clinical trials; the ability of our product candidates to achieve applicable endpoints in the clinical trials; our exploratory clinical signals may not be predictive of outcomes in larger, randomized controlled trials; the safety profile of our product candidates; the potential for data from our clinical trials to support a marketing application, as well as the timing of these events; our ability to obtain funding for our operations; development and commercialization of our product candidates; the timing of and our ability to obtain and maintain regulatory approvals; anticipated interactions with the FDA under Fast Track designation; the rate and degree of market acceptance and clinical utility of our product candidates; the size and growth potential of the markets for our product candidates, and our ability to serve those markets; our commercialization, marketing and manufacturing capabilities and strategy; future agreements with third parties in connection with the commercialization of our product candidates; our expectations regarding our ability to obtain and maintain intellectual property protection; our dependence on third party manufacturers; the success of competing therapies or products that are or may become available; our ability to attract and retain key scientific or management personnel; our ability to identify additional product candidates with significant commercial potential consistent with our commercial objectives; ; and our estimates regarding expenses, future revenue, capital requirements and needs for additional financing.
We have based these forward-looking statements largely on our current expectations and projections about future events and trends that we believe may affect our financial condition, results of operations, business strategy, short-term and long-term business operations and objectives, and financial needs. Moreover, we operate in a very competitive and rapidly changing environment, and new risks may emerge from time to time. It is not possible for our management to predict all risks, nor can we assess the impact of all factors on our business or the extent to which any factor, or combination of factors, may cause actual results to differ materially from those contained in any forward-looking statements we may make. In light of these risks, uncertainties and assumptions, the forward-looking events and circumstances discussed herein may not occur and actual results could differ materially and adversely from those anticipated or implied in the forward-looking statements. Although our management believes that the expectations reflected in our forward-looking statements are reasonable, we cannot guarantee that the future results, levels of activity, performance or events and circumstances described in the forward-looking statements will be achieved or occur. We undertake no obligation to publicly update any forward-looking statements, whether written or oral, that may be made from time to time, whether as a result of new information, future developments or otherwise.
Phase 2Clinical ResultFast Track
100 Deals associated with IL-2(Shanghai Xinshengyuan Biological Medicine Co. Ltd.)
Login to view more data
R&D Status
10 top R&D records. to view more data
Login
| Indication | Highest Phase | Country/Location | Organization | Date |
|---|---|---|---|---|
| Gastrointestinal Neoplasms | Clinical | China | - |
Login to view more data
Clinical Result
Clinical Result
Indication
Phase
Evaluation
View All Results
| Study | Phase | Population | Analyzed Enrollment | Group | Results | Evaluation | Publication Date |
|---|
Phase 1 | 5 | csmdgymzfk(zqieexafmq) = ywipgcdtgd jbdyyppycj (jktgdlwpme ) View more | - | 10 Feb 2012 |
Login to view more data
Translational Medicine
Boost your research with our translational medicine data.
login
or

Deal
Boost your decision using our deal data.
login
or

Core Patent
Boost your research with our Core Patent data.
login
or

Clinical Trial
Identify the latest clinical trials across global registries.
login
or

Approval
Accelerate your research with the latest regulatory approval information.
login
or

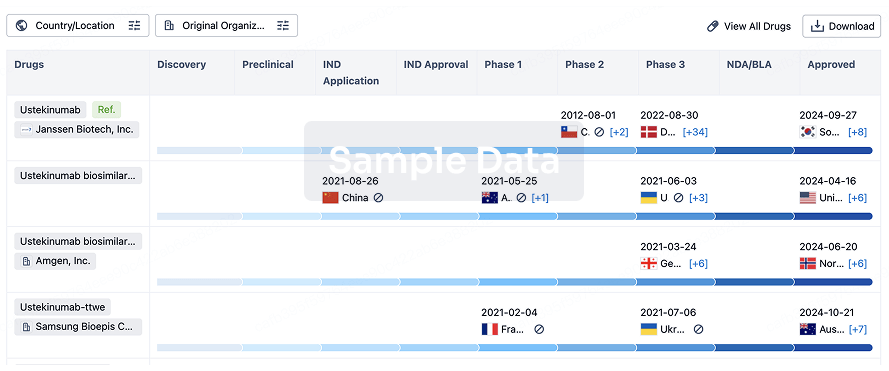
Biosimilar
Competitive landscape of biosimilars in different countries/locations. Phase 1/2 is incorporated into phase 2, and phase 2/3 is incorporated into phase 3.
login
or
Regulation
Understand key drug designations in just a few clicks with Synapse.
login
or

AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free