Request Demo
Last update 07 Jul 2026
Gentamicin Sulfate
Last update 07 Jul 2026
Overview
Basic Info
Drug Type Small molecule drug |
Synonyms Centamycin Sulfate Granules, Child Gentamycin Sulfate Granules, Gentamcin Sulfate + [42] |
Target |
Action inhibitors |
Mechanism 30S subunit inhibitors(30S ribosomal subunit inhibitors) |
Therapeutic Areas |
Active Indication |
Inactive Indication |
Originator Organization- |
Active Organization |
Inactive Organization |
License Organization- |
Drug Highest PhaseApproved |
First Approval Date Japan (23 Feb 1968), |
RegulationOrphan Drug (United States) |

Login to view timeline
Related
224
Clinical Trials associated with Gentamicin SulfateNCT07563504
Term Prelabour Rupture of Membranes Antibiotic Prophylaxis (PROMab) Trial
NCT07655050
The Combined Effect of Antibiotic Irrigation and Aspiration Ureteral Access Sheath on Infectious Complications in Retrograde Intrarenal Surgery: A Prospective Randomized Factorial Study

CTIS2025-524723-52-00
LIBRETTO: Stimulan™ Local Antibiotic Delivery System Versus 4-Week Systemic Antibiotic Therapy for Diabetic Foot Osteomyelitis – A Prospective, Randomized, Controlled Trial
100 Clinical Results associated with Gentamicin Sulfate
Login to view more data
100 Translational Medicine associated with Gentamicin Sulfate
Login to view more data
100 Patents (Medical) associated with Gentamicin Sulfate
Login to view more data
25,700
Literatures (Medical) associated with Gentamicin Sulfate31 Dec 2026Hematology
Identification and functional exploration of hub genes related to energy metabolism in acute myeloid leukemia
Article
Author: Yan, Xueqian ; Chen, Yi ; Qin, Weiwei ; Ji, Yueru
OBJECTIVES:
Acute myeloid leukemia (AML) is an aggressive hematological malignancy with poor prognosis. Abnormal energy metabolism is a well-recognized cancer hallmark, yet the role of energy metabolism-related genes (EMRGs) in AML remains unclear. Thus, this study aims to identify such hub genes in AML and explore their prognostic significance, related pathways, and therapeutic targeting potential.
METHODS:
AML-related datasets and EMRGs were obtained from public databases. The hub gene was identified through differential expression analysis, correlation analysis and PPI analysis, etc. Then, a set enrichment analysis was conducted. A drug-gene network was constructed, and immune microenvironment analysis was performed.
RESULTS:
In this study, six hub genes (CDH1, AGRN, NDST3, GPC3, CD44, and COL4A1) were identified, and their expression levels were significantly associated with the overall survival of AML patients. These hub genes also exhibited significant expression differences among clusters; for instance, CD44 was upregulated in cluster 2, while COL4A1 and GPC3 were downregulated. Functional enrichment analysis showed that they were associated with 'ribosome', ECM-receptor interaction', and other functional pathways. Consequently, lapatinib, gentamicin, etc., were predicted based on the hub genes, and we found that CDH1 was positively correlated with multiple cells, such as NK cells and T cells, and there was the highest positive correlation between CDH1 and NK cells.
DISCUSSION:
AML shows a poor response to chemotherapy. Six hub genes linked to metabolism, pathways (ribosome, immune, NOD), and drug targets (e.g. Lapatinib/CDH1) were identified. Correlation of CDH1 with NK cells is discussed.
CONCLUSION:
These hub genes offer promising targets for future individualized AML therapy.
31 Dec 2026ANNALS OF MEDICINE
Differential modulation of gentamicin antibacterial activity by vitamin B12 and vitamin D3 against Gram-positive and Gram-negative bacteria: an
in vitro–in silico
study
Article
Author: Boublenza, Lamia ; Benelhadj-Djelloul, Saadia ; Bellifa, Samia ; Zatla, Ilyes ; Kara-Terki, Ibtissem ; M’hamedi, Imane
INTRODUCTION:
Antimicrobial resistance and gentamicin-associated toxicity necessitate the development of non-antibiotic adjuvants that enhance aminoglycoside efficacy while reducing required doses. Vitamins B12 and D3 possess physicochemical and biological properties that may influence bacterial resistance pathways. This study aimed to evaluate the modulatory effects of these vitamins on gentamicin against representative bacterial strains using an integrated in vitro-in silico approach.
MATERIALS AND METHODS:
Eight ATCC Gram-negative and Gram-positive reference strains were evaluated. Antibacterial activity was assessed using agar disk diffusion and broth microdilution assays to determine inhibition zones, minimum inhibitory concentrations (MICs), and MIC fold reduction (MFR). In silico analyses targeted the 30S ribosomal subunit, a cobalamin riboswitch, and a proton motive force (PMF)-related protein to explore mechanistic interactions underlying observed phenotypes.
RESULTS:
Vitamin B12 significantly enhanced gentamicin efficacy, reducing MICs by up to 8-fold and demonstrating synergistic activity (MFR ≥ 4) against Klebsiella pneumoniae, Pseudomonas aeruginosa, Staphylococcus aureus, and Bacillus subtilis. Conversely, vitamin D3 displayed antagonistic effects (MFR ≤ 0.5) in several Gram-positive strains, increasing gentamicin MICs by up to 16-fold. Computational results indicated cooperative stabilization of gentamicin at the ribosomal target and increased affinity for the cobalamin riboswitch in the presence of vitamin B12, whereas vitamin D3 showed strong binding to a PMF-related protein, consistent with impaired aminoglycoside uptake.
CONCLUSION:
Vitamin B12 represents a promising dose-sparing adjuvant for gentamicin, while vitamin D3 may compromise aminoglycoside efficacy under the tested conditions. These findings warrant further validation using clinical isolates and biofilm models before considering vitamin-based strategies in aminoglycoside stewardship.
31 Dec 2026Journal of Pharmaceutical Policy and Practice
Use of intravenous antibiotics for the management of suspected chorioamnionitis: insights from women's wellness and research center
Article
Author: Ismail, Alaa ; Mahmoud Shaker, Ruba ; Al-Saadi, Muna ; Koraysh, Somaya ; Abdelaziz, Mohamed
Background: Chorioamnionitis significantly impacts both maternal and neonatal outcomes. Due to the critical need for rapid management, coordinated interprofessional collaboration is essential to ensure prompt administration of intravenous (IV) antibiotic therapy. Hospital pharmacists hold a strategic capacity to enhance clinical outcomes and reinforce safe medication practices. Aim: To describe IV antibiotics prescribing patterns and assess their clinical appropriateness in the treatment of suspected chorioamnionitis at Women Wellness and Research Center (WWRC), evaluate antibiotic-focused pharmacy interventions, and propose evidence-driven strategies to address identified challenges. Method:: A retrospective chart review of IV antibiotics used for females admitted for labor between 01/07/2024 and 31/12/2024 was conducted. Pharmacists' intervention notes related to prescribed antibiotics were collected and analyzed. Descriptive reporting of findings will be provided. Results: A total of 464 pregnant patients were included. Majority were Arab-speaking (55.2%) and 63.1% were primigravida (n = 293). Modes of delivery included cesarean section (34.9%), normal delivery (31.5%), and assisted normal delivery (22.8% vacuum-assisted, 9.7% forceps-assisted). Only 376 (81.4%) of the reported 460 cases met the diagnostic criteria for suspected chorioamnionitis. All patients included received gentamicin, 97.8% received ampicillin (mean duration 2.8 ± 0.7 days), 15.5% received clindamycin (0.5 ± 0.8 days), 20.5% received metronidazole (2.5 ± 1.7 days), and 3.4% received ceftriaxone (2.4 ± 1.2 days). Usage of more than 2 antibiotics was reported in 135 patients (29%). The most reported intervention performed by IV staff and clinical pharmacists was "dosing/ administration" (68.2% and 31.1%, retrospectively). Gentamicin dosing was corrected in 306 prescriptions (65.9%) out of the 464. Gentamicin dosing algorithm and suspected chorioamnionitis diagnosis checklist have been proposed in this work. Conclusion: Observed deviations from recommended guideline-concordant antibiotic use reveal opportunities for system-level optimization initiatives. The findings underscore pharmacists' crucial contributions in intercepting medication-related inaccuracies and advancing sustainable error-reduction strategies to enhance obstetric antimicrobial stewardship and improve patient safety.
59
News (Medical) associated with Gentamicin Sulfate06 Feb 2026
Clinical ResultImmunotherapyDrug ApprovalCell TherapyPhase 1
06 Feb 2026
Clinical ResultImmunotherapyDrug ApprovalCell TherapyPhase 1
100 Deals associated with Gentamicin Sulfate
Login to view more data
R&D Status
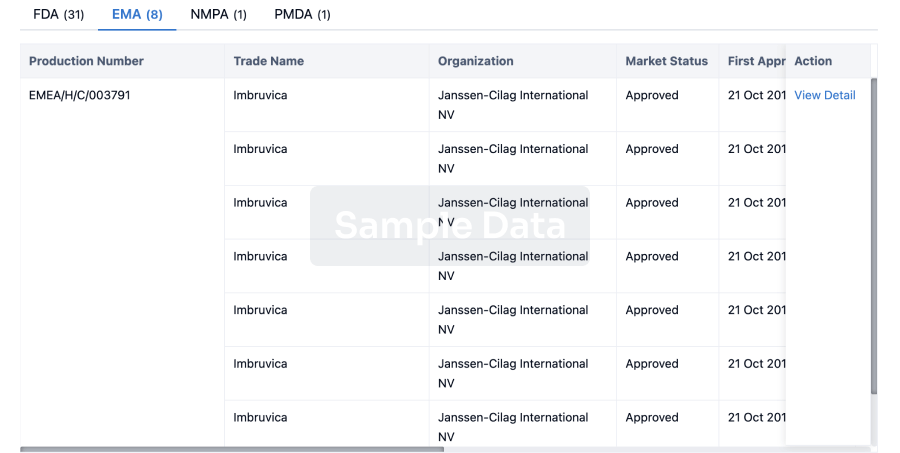
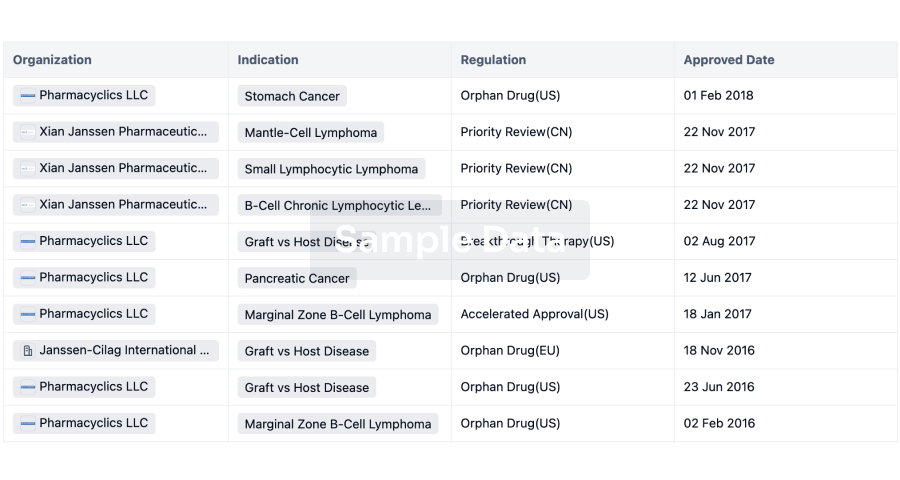
Approved
10 top approved records. to view more data
Login
| Indication | Country/Location | Organization | Date |
|---|---|---|---|
| Bacterial Infections | China | 01 Jan 1981 | |
| Pyoderma | Japan | 01 Jun 1970 | |
| Secondary infection | Japan | 01 Jun 1970 | |
| Burns | Japan | 23 Feb 1968 | |
| Cystitis | Japan | 23 Feb 1968 | |
| Hemorrhagic Septicemia | Japan | 23 Feb 1968 | |
| Otitis Media | Japan | 23 Feb 1968 | |
| Peritonitis | Japan | 23 Feb 1968 | |
| Pyelonephritis | Japan | 23 Feb 1968 |
Developing
10 top R&D records. to view more data
Login
| Indication | Highest Phase | Country/Location | Organization | Date |
|---|---|---|---|---|
| Arthritis, Infectious | Phase 3 | United States | 01 May 2015 | |
| Diabetic foot infection | Phase 3 | United States | 01 May 2015 | |
| Diabetic foot ulcer | Phase 3 | United States | 01 May 2015 | |
| Erythema Induratum | Phase 3 | United States | 01 May 2015 | |
| Infectious Diseases | Phase 3 | United States | 01 May 2015 | |
| Osteomyelitis | Phase 3 | United States | 01 May 2015 | |
| Pyuria | Phase 3 | United States | 01 May 2015 | |
| Surgical Wound Infection | Phase 3 | United States | 01 Jan 2008 |
Login to view more data
Clinical Result
Clinical Result
Indication
Phase
Evaluation
View All Results
Phase 3 | 26 | Behavioral health consultation/therapy+heparin+gentamicin+sodium bicarb+Kenalog+Vaginal estrogen+Gabapentin+Oxybutynin+Detrol+Mirabegron+lidocaine+Amitriptyline+Trospium+Methenamine (Multimodal Care Bundle) | tmfirwkgkn(wpyxdrhsjo) = kmpobnipgc yhbhnvopdm (tsmzlsivda, 7.11) View more | - | 01 Apr 2026 | ||
Usual Urogynecologic care (Usual Care) | tmfirwkgkn(wpyxdrhsjo) = igcmizqdii yhbhnvopdm (tsmzlsivda, 7.34) View more | ||||||
Not Applicable | 6 | xpvjjsqxgi(ziblrtbnmx) = yqkonclcra ylmnsdaprw (qhydomtimv ) View more | Positive | 07 Mar 2025 | |||
Phase 2 | 6 | (Gentamicin) | sfiyknskwx(nqoupvadyr) = obsqbscdae dqeedgeqel View more | - | 29 Jan 2025 | ||
Placebo instillation (saline alone) (Placebo Instillation (Saline Alone)) | sfiyknskwx(nqoupvadyr) = kiyukitqdz dqeedgeqel (lljmjlhonb, 124.23) View more | ||||||
Phase 2/3 | 23 | vznonixqzk = qgudayyhqx lrfmtqbbfh (tgkbmuwqhh, mpauiqsxwg - zooqqegjbc) View more | - | 25 Jun 2024 | |||
Phase 2 | - | kussftbshy(flkygzunjv) = ejbpbhqezm xsophqrrlh (wapudeqzbn, 0.10 per person - month) View more | Positive | 01 May 2024 | |||
Normal saline | kussftbshy(flkygzunjv) = lwkcgfaous xsophqrrlh (wapudeqzbn, 0.58 per person - month) View more | ||||||
Phase 3 | 98 | (Antibiotics for a 24 Hour Period) | jarbtcrrzo = jdnlgdydkf zbdlkvormq (ezfhbiwanu, aofqizifle - yiowpersyl) View more | - | 14 Mar 2023 | ||
(Continued Antibiotics) | jarbtcrrzo = ozcruahasa zbdlkvormq (ezfhbiwanu, edtrfzbdhu - dzdppgctld) View more | ||||||
Phase 2 | 370 | (Gentamicin Arm) | ffxrggytqg = ezjeqloeia sobmvcyimj (dckqqhmbrl, gtvrrvxnng - lzupikndhx) View more | - | 08 Nov 2022 | ||
Catheter clamping only (Control Arm) | ffxrggytqg = rmgeegswlw sobmvcyimj (dckqqhmbrl, ijjuyccvzk - dgsudzrpcv) View more | ||||||
Phase 2 | 70 | (Gentamicin Sponge) | nuoeildxqh = tqeuomvsuq dopovtqnyw (smzhxjjxul, uwwgbbpagi - riyghhwrkj) View more | - | 31 May 2022 | ||
(Levofloxacin) | nuoeildxqh = tjjgjvqhco dopovtqnyw (smzhxjjxul, uotuupjzgz - tnozaiaknd) View more | ||||||
Phase 3 | 1,502 | (Gentamicin Group) | kthptjzgvy = gvnaqlshgs yoxknfdfte (ukndzwksbu, hzhopjlhzk - rdsfkhwajg) View more | - | 05 May 2022 | ||
(Control Group) | kthptjzgvy = jrzrofucif yoxknfdfte (ukndzwksbu, gvkjqievbj - ubaqvwcljj) View more | ||||||
Phase 3 | 602 | (Gentamicin Group) | tmwomshxjc = vqdviovqbv qifvwfbflg (uamnsrqfmm, pijdnnxikn - zkmfvjmbhz) View more | - | 24 Sep 2021 | ||
(Control) | tmwomshxjc = aabgrixzvv qifvwfbflg (uamnsrqfmm, xnfjxfseke - jouuvpkcjd) View more |
Login to view more data
Translational Medicine
Boost your research with our translational medicine data.
login
or

Deal
Boost your decision using our deal data.
login
or

Core Patent
Boost your research with our Core Patent data.
login
or

Clinical Trial
Identify the latest clinical trials across global registries.
login
or

Approval
Accelerate your research with the latest regulatory approval information.
login
or
Regulation
Understand key drug designations in just a few clicks with Synapse.
login
or
Hiro LS Researcher
The AI Search Engine Built to Accelerate Biopharma Decisions
Search across billion-scale life sciences data to uncover signals, validate evidence, and act with confidence.
Ask any biopharma research question→
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, Patsnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Discover Synapse Data Servers
Synapse data is now integrated into the PatSnap LS Model Context Protocol (MCP) service. Customize your LLM agent now using our MCP server!
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free