Request Demo
Last update 22 Dec 2025
Atezolizumab
Last update 22 Dec 2025
Overview
Basic Info
Drug Type Monoclonal antibody |
Synonyms Anti-PDL-1-Genentech/Roche, Atezolizumab (Genetical Recombination), Atezolizumab (genetical recombination) (JAN) + [11] |
Target |
Action inhibitors |
Mechanism PDL1 inhibitors(Programmed death-ligand 1 inhibitors) |
Therapeutic Areas |
Active Indication |
Inactive Indication |
Originator Organization |
Active Organization |
Inactive Organization |
License Organization |
Drug Highest PhaseApproved |
First Approval Date United States (18 May 2016), |
RegulationBreakthrough Therapy (United States), Fast Track (United States), Accelerated Approval (United States), Orphan Drug (United States), Orphan Drug (Japan), Orphan Drug (Australia), Priority Review (Australia), Conditional marketing approval (China), Priority Review (China) |





Login to view timeline
Structure/Sequence
Sequence Code 122091L
Source: *****
Sequence Code 4720027H
Source: *****
Related
896
Clinical Trials associated with AtezolizumabNCT07235293
A Randomized, Open-label, Phase 2b Study to Compare the Efficacy of DSP107 in Combination With Atezolizumab Versus Fruquintinib in Patients With Advanced Microsatellite Stable Colorectal Cancer
NCT07276100
Fecal Microbiota Transplantation to RESCUE Patients With Unresectable Hcc Progressors to First Line Therapy With AtezolizUmaB and Bevacizumab
NCT06492954
Phase 1b Trial of Atezolizumab in Combination With Stereotactic Body Radiation Therapy (SBRT) and Surgery in Patients With Pulmonary Recurrence of Osteosarcoma
100 Clinical Results associated with Atezolizumab
Login to view more data
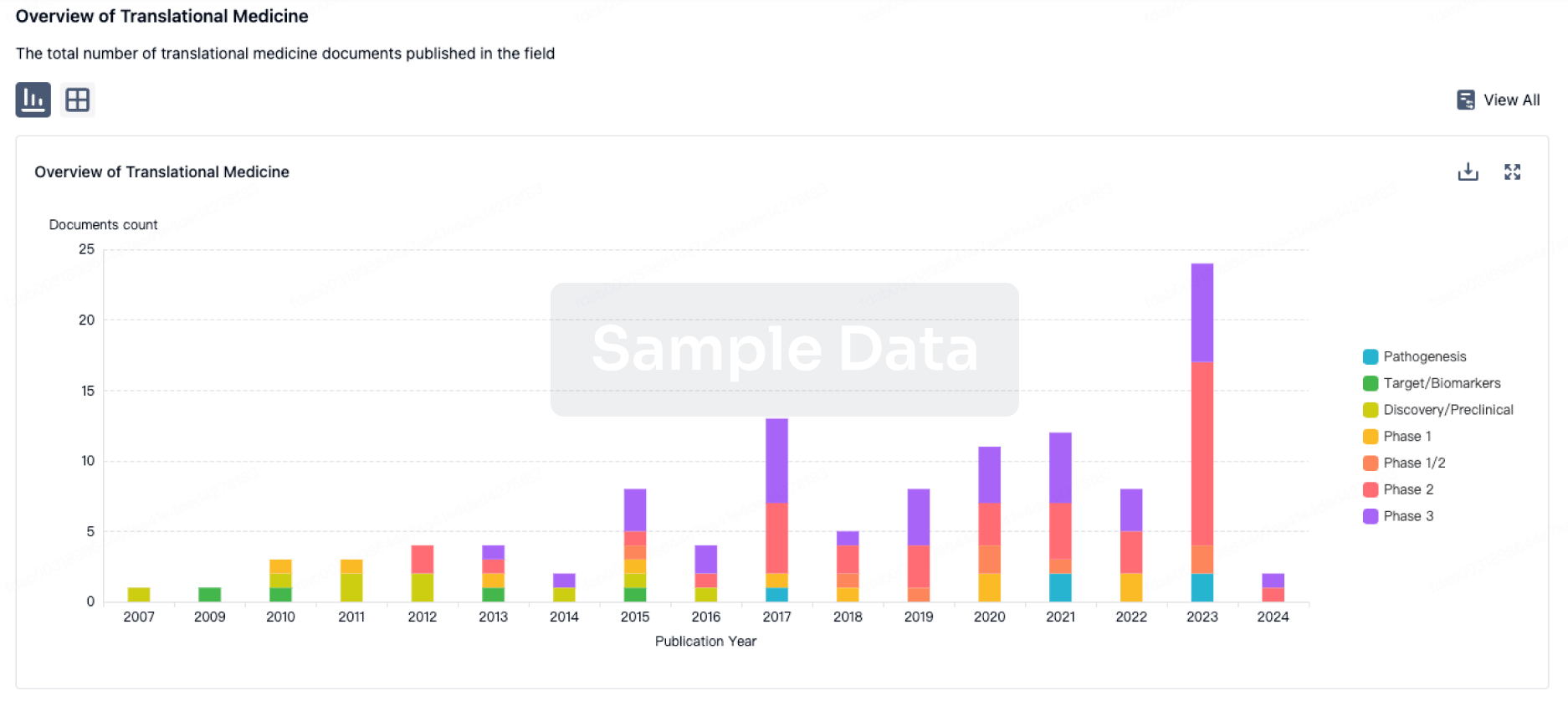
100 Translational Medicine associated with Atezolizumab
Login to view more data
100 Patents (Medical) associated with Atezolizumab
Login to view more data
4,499
Literatures (Medical) associated with Atezolizumab01 Apr 2026DEN open
A Rare Case of Immune‐related Adverse Events Localized to the Small Intestine
Article
Author: Morikawa, Ryo ; Taguchi, Towako ; Fukuda, Masayoshi ; Okamoto, Ryuichi ; Fujii, Toshimitsu ; Kanaya, Ryosuke ; Nemoto, Yasuhiro ; Yamamoto, Kurara ; Ohtsuka, Kazuo ; Shimizu, Hiromichi
ABSTRACT:
Enterocolitis is a common gastrointestinal manifestation of immune‐related adverse events (irAEs); however, only a few studies have reported on irAE enteritis with localized active inflammation in the small intestine. Here, we report the case of a 74‐year‐old man who developed diarrhea, abdominal pain, and oral intake difficulty and was subsequently hospitalized after receiving atezolizumab for pulmonary adenocarcinoma. Computed tomography and enterocolonoscopy revealed active inflammation in the small intestine but not in the colon, leading to the final diagnosis of irAE enteritis. After initiating prednisolone at a dose of 60 mg/day, his symptoms improved rapidly, and a follow‐up enterocolonoscopy revealed a marked reduction in inflammation. Being a relatively rare gastrointestinal toxicity, irAE enteritis often goes unrecognized due to diagnostic challenges, but can lead to serious AEs such as perforation. Therefore, even if colonoscopy findings are normal, a thorough examination of the small intestine is essential for patients who develop gastrointestinal symptoms while undergoing immune checkpoint inhibitor therapy. We herein report a rare case of irAE enteritis confirmed through endoscopic and pathological examination, which has not been previously reported.
01 Apr 2026DEN open
A Case of Obstructive Jaundice due to Bile Duct Tumor Thrombus of Hepatocellular Carcinoma Diagnosed by Peroral Cholangioscopy
Article
Author: Tokumaru, Tomoko ; Endo, Mizuki ; Kinoshita, Keisuke ; Uchida, Takuro ; Murakami, Kazunari ; Okamoto, Kazuhisa ; Saito, Tomoko ; Kodama, Masaaki ; Iwao, Masao ; Arakawa, Mie
Abstract:
While hepatocellular carcinoma (HCC) often invades the portal or hepatic vein to form tumor thrombus, tumor thrombus in the bile duct is rare. In such cases, differentiation from intrahepatic cholangiocarcinoma is difficult, and the tumor often appears as a smooth, yellowish‐white, polypoid mass within the bile duct lumen. We report herein a case of obstructive jaundice due to bile duct tumor thrombus of HCC diagnosed by peroral cholangioscopy (POCS). A 64‐year‐old man presented with epigastralgia and jaundice. Contrast‐enhanced computed tomography revealed an irregular mass with hypoenhancement in liver segment S8, along with dilatation of the right intrahepatic bile duct due to the invading tumor. The hepatic mass was poorly visualized on ultrasound, making percutaneous liver tumor biopsy difficult. POCS was performed after endoscopic retrograde cholangiopancreatography for biopsy of the intrahepatic bile duct tumor thrombus. POCS clearly revealed a smooth, yellowish‐white, polypoid tumor in the right intrahepatic bile duct, and a biopsy of the tumor was performed under POCS. Based on the pathological findings, HCC was diagnosed, and chemotherapy with atezolizumab and bevacizumab was initiated.
01 Jan 2026Value in Health Regional Issues
Real-World Effectiveness and Cost-Utility Analysis of Second-Line Immunotherapy for Non-Oncogene-Addicted Advanced Non-Small Cell Lung Cancer
Article
Author: Preedachitkul, Rinrada ; Chitpim, Natthakan ; Khunakorncharatphong, Anon ; Thamlikitkul, Lucksamon ; Horugsa, Chulamas ; Sawasdisara, Sasiporn ; Srinonprasert, Varalak
OBJECTIVES:
To determine the cost-effectiveness of second-line immune checkpoint inhibitors (ICIs) compared with chemotherapy in patients with advanced non-small cell lung cancer (NSCLC) using real-world patient-level treatment effectiveness, cost, and utility data.
METHODS:
Medical records of patients with NSCLC receiving second-line ICIs or chemotherapy at Siriraj Hospital, Bangkok, Thailand from January 2016 to May 2023 were reviewed to evaluate treatment effectiveness and direct medical costs. Patients receiving treatment from July 2023 to March 2024 were interviewed to determine utility and direct nonmedical costs. A semi-Markov model was used to analyze the lifetime costs and health outcomes from societal perspective. One-way and probabilistic sensitivity analyses and scenario analyses were performed.
RESULTS:
Data were collected from 209 patients (72 and 137 patients received second-line ICIs and chemotherapy, respectively). Second-line ICIs significantly improved overall survival (hazard ratio 0.64, 95% confidence interval 0.47-0.89, P = .008) and increased the quality-adjusted life-years (QALYs) from 0.54 to 1.11, resulting in QALY gain of 0.57; lifetime cost increased from 17 204 US dollar (USD) to 34 424 USD. Second-line ICI incremental cost-effectiveness ratio was 30 104 USD/QALY. Scenario analysis revealed that second-line ICIs were more cost-effective than chemotherapy for healthier patients (Eastern Cooperative Oncology Group 0-1) with incremental cost-effectiveness ratio of 9856 USD/QALY. Considering Thailand's willingness-to-pay threshold of 4444 USD/QALY, second-line ICIs could be cost-effective if the cost of atezolizumab was reduced by 86%.
CONCLUSION:
Second-line ICIs significantly improved survival in advanced NSCLC but are not cost-effective in Thailand. Drug price negotiation and patient subgroup prioritization would help make second-line ICIs more accessible.
1,526
News (Medical) associated with Atezolizumab19 Dec 2025
Drug ApprovalImmunotherapyBiosimilar
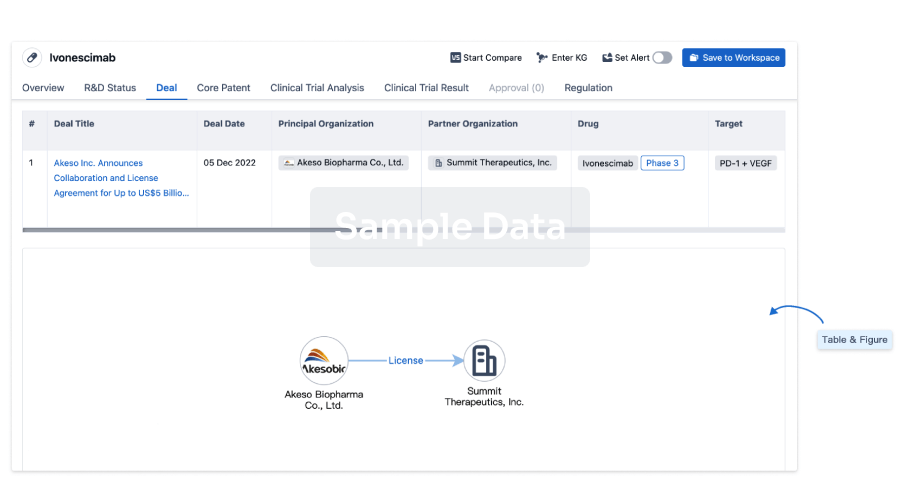
100 Deals associated with Atezolizumab
Login to view more data
External Link
| KEGG | Wiki | ATC | Drug Bank |
|---|---|---|---|
| D10773 | Atezolizumab |
R&D Status
Approved
10 top approved records. to view more data
Login
| Indication | Country/Location | Organization | Date |
|---|---|---|---|
| Extranodal NK-T-Cell Lymphoma | Japan | 19 Sep 2025 | |
| Advanced Lung Non-Small Cell Carcinoma | European Union | 25 Jul 2024 | |
| Advanced Lung Non-Small Cell Carcinoma | Iceland | 25 Jul 2024 | |
| Advanced Lung Non-Small Cell Carcinoma | Liechtenstein | 25 Jul 2024 | |
| Advanced Lung Non-Small Cell Carcinoma | Norway | 25 Jul 2024 | |
| Breast Cancer | Canada | 13 Mar 2024 | |
| Alveolar Soft Part Sarcoma | United States | 09 Dec 2022 | |
| PD-L1 positive Non-Small Cell Lung Cancer | Japan | 26 May 2022 | |
| BRAF V600 mutation-positive Melanoma | United States | 30 Jul 2020 | |
| PD-L1 positive Triple Negative Breast Cancer | Japan | 19 Jan 2018 | |
| Advanced Hepatocellular Carcinoma | European Union | 20 Sep 2017 | |
| Advanced Hepatocellular Carcinoma | Iceland | 20 Sep 2017 | |
| Advanced Hepatocellular Carcinoma | Liechtenstein | 20 Sep 2017 | |
| Advanced Hepatocellular Carcinoma | Norway | 20 Sep 2017 | |
| Advanced Triple-Negative Breast Carcinoma | European Union | 20 Sep 2017 | |
| Advanced Triple-Negative Breast Carcinoma | Iceland | 20 Sep 2017 | |
| Advanced Triple-Negative Breast Carcinoma | Liechtenstein | 20 Sep 2017 | |
| Advanced Triple-Negative Breast Carcinoma | Norway | 20 Sep 2017 | |
| Extensive stage Small Cell Lung Cancer | European Union | 20 Sep 2017 | |
| Extensive stage Small Cell Lung Cancer | Iceland | 20 Sep 2017 |
Developing
10 top R&D records. to view more data
Login
| Indication | Highest Phase | Country/Location | Organization | Date |
|---|---|---|---|---|
| Bladder Cancer | NDA/BLA | China | 25 Feb 2019 | |
| Lymphoproliferative Disorders | Phase 3 | United Kingdom | 25 Oct 2023 | |
| Melanoma | Phase 3 | United Kingdom | 25 Oct 2023 | |
| Microsatellite instability-high cancer | Phase 3 | United Kingdom | 25 Oct 2023 | |
| Turcot Syndrome | Phase 3 | United Kingdom | 25 Oct 2023 | |
| Muscle Invasive Bladder Carcinoma | Phase 3 | Belgium | 03 May 2021 | |
| Muscle Invasive Bladder Carcinoma | Phase 3 | Hong Kong | 03 May 2021 | |
| Muscle Invasive Bladder Carcinoma | Phase 3 | Mexico | 03 May 2021 | |
| Muscle Invasive Bladder Carcinoma | Phase 3 | Singapore | 03 May 2021 | |
| Locally advanced breast cancer | Phase 3 | United States | 29 Mar 2021 |


Login to view more data
Clinical Result
Clinical Result
Indication
Phase
Evaluation
View All Results
Phase 3 | 837 | (Experimental Arm: Cabozantinib + Atezolizumab) | utoqxrqofz(xprawnxfqr) = bxisukbudp ctbjwthfdl (hhuuyhcaym, nviukfbicd - uilxcspart) View more | - | 11 Dec 2025 | ||
(Control Arm: Sorafenib) | utoqxrqofz(xprawnxfqr) = gjwotavuau ctbjwthfdl (hhuuyhcaym, znrsihkwcw - eicsclhmvq) View more | ||||||
Not Applicable | Neoplasms PD-1 | PD-L1 | CTLA-4 | 84,885 | qtzavthbcs(pketdrrrxx) = xgeprluqct yqeqjhcvwf (qtubcylcrj ) View more | Positive | 06 Dec 2025 | ||
qtzavthbcs(pketdrrrxx) = abzxvezuxl yqeqjhcvwf (qtubcylcrj ) View more | |||||||
Not Applicable | 11 | uqxcaokftf(abjyhwkuie) = fddkkwjupp fgzitqmitd (vqljooibew ) View more | Positive | 05 Dec 2025 | |||
Phase 2 | 20 | rnjdufwuup(kgouuwzvds) = jqnwtcgjdd exwpicpnfe (qveduvmnnx, 18.8 - 58.2) View more | Positive | 05 Dec 2025 | |||
Not Applicable | Extensive stage Small Cell Lung Cancer First line | 1,096 | zycxpdpmnv(vybozfwxpi) = vndwlrfxqw mmzvkxfalq (mdtmqqiisr ) View more | Negative | 05 Dec 2025 | ||
zycxpdpmnv(vybozfwxpi) = eowplkszhv mmzvkxfalq (mdtmqqiisr ) View more | |||||||
Not Applicable | Unresectable Hepatocellular Carcinoma First line | 3,222 | ppwtmdcigk(fdqadxkmkt): HR = 0.98 (95.0% CI, 0.24 - 4.1) | Positive | 05 Dec 2025 | ||
Phase 2 | 41 | mmprlcrddp(mrpnaodlnp) = rmhddyxesx tvsgbgzmdd (sxagqhrqqk, mrwcbrlinb - pndcawztue) View more | - | 04 Dec 2025 | |||
Phase 3 | Recurrent ovarian cancer PD-L1-positive | 574 | tlnzgjdvyr(rfrmqijdnw) = mgjnricvoo umrrjjfrkc (ldrddoqkzj ) View more | Negative | 03 Dec 2025 | ||
tlnzgjdvyr(rfrmqijdnw) = ijscieockw umrrjjfrkc (ldrddoqkzj ) View more | |||||||
Phase 2 | Non-Small Cell Lung Cancer EGFR mutation‐positive | 23 | (EGFR mutation-positive metastatic non-squamous NSCLC who failed EGFR-TKIs) | nqdgrovdpe(kcebawqkiq) = idqcejjcgd kfbgwwevwf (xqaifvlgef ) View more | Negative | 01 Dec 2025 | |
Phase 3 | 595 | Placebo (Placebo + Chemotherapy) | mksasavfqr(fpjwdppbdk) = ftuhotqxnq fqetcgywku (smmjcqzfsh, rglkekwayl - zokifjyezg) View more | - | 12 Nov 2025 | ||
(Atezolizumab + Chemotherapy) | mksasavfqr(fpjwdppbdk) = kbriwhzfci fqetcgywku (smmjcqzfsh, zqqdqvnrtl - uwbmzsslqu) View more |
Login to view more data
Translational Medicine
Boost your research with our translational medicine data.
login
or
Deal
Boost your decision using our deal data.
login
or
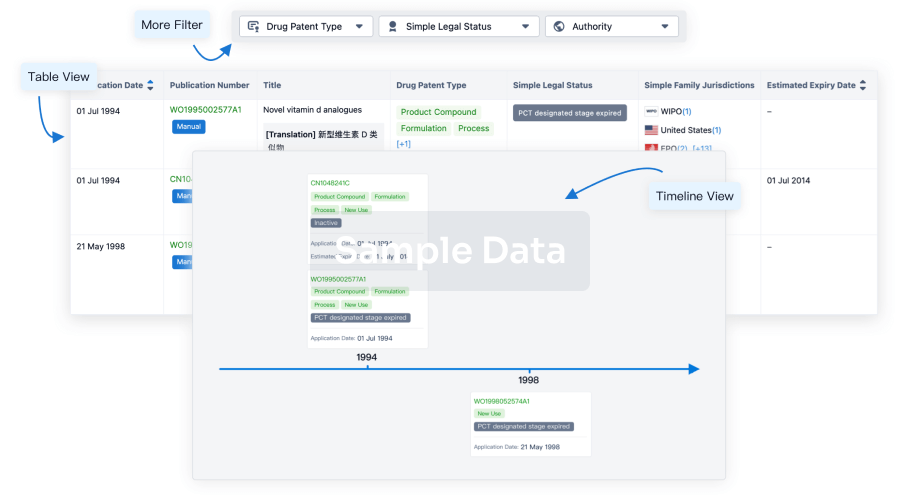
Core Patent
Boost your research with our Core Patent data.
login
or
Clinical Trial
Identify the latest clinical trials across global registries.
login
or
Approval
Accelerate your research with the latest regulatory approval information.
login
or
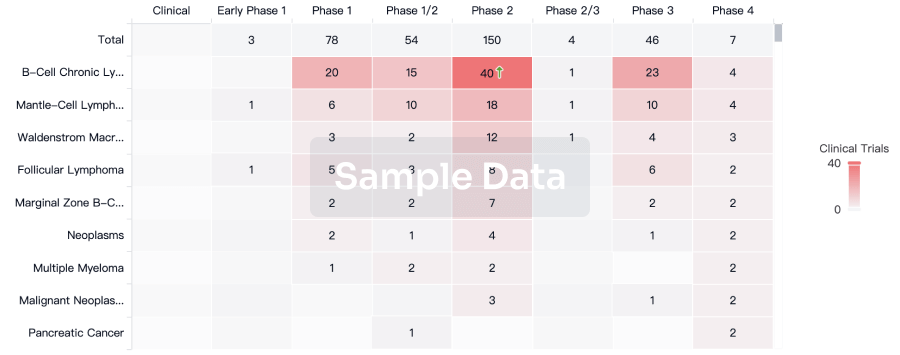
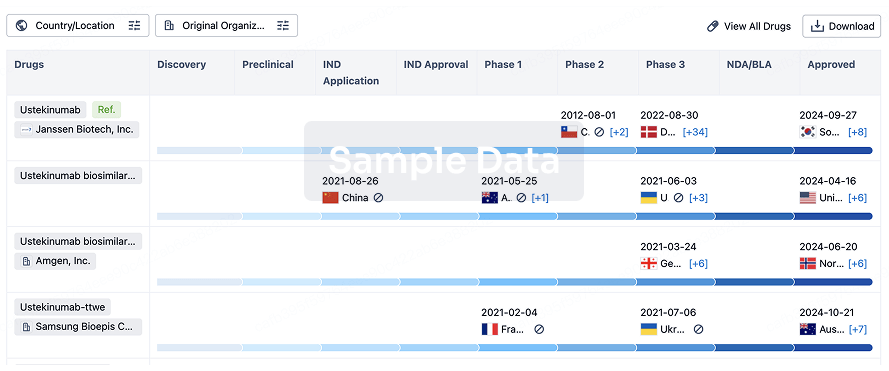
Biosimilar
Competitive landscape of biosimilars in different countries/locations. Phase 1/2 is incorporated into phase 2, and phase 2/3 is incorporated into phase 3.
login
or
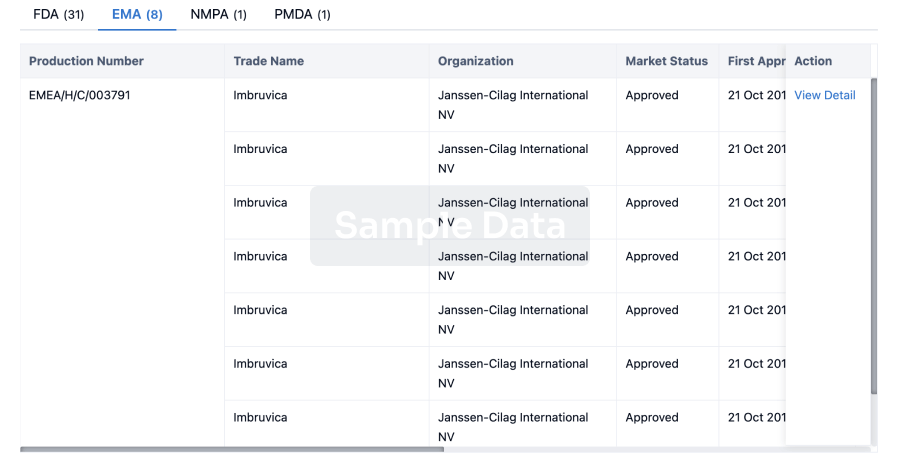
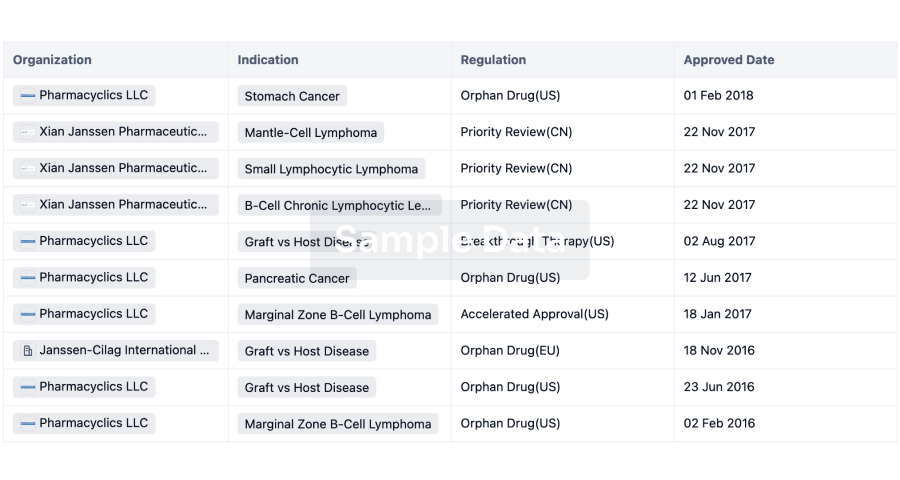
Regulation
Understand key drug designations in just a few clicks with Synapse.
login
or
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free