Request Demo
Last update 15 Jul 2026
Sorafenib Tosylate
Last update 15 Jul 2026
Overview
Basic Info
Drug Type Small molecule drug |
Synonyms N-(4-Chloro-3-(trifluoromethyl)phenyl)-N'-(4-(2-(N-methylcarbamoyl)-4-pyridyloxy)phenyl)urea, SORAFENIB, Sorafenib tosilate + [16] |
Action inhibitors, antagonists |
Mechanism BRAF inhibitors(Serine/threonine-protein kinase B-raf inhibitors), CRAF inhibitors(C-Raf kinase inhibitors), FLT3 inhibitors(Tyrosine-protein kinase receptor FLT3 inhibitors) |
Therapeutic Areas |
Active Indication |
Inactive Indication |
Originator Organization |
Active Organization |
Inactive Organization |
License Organization |
Drug Highest PhaseApproved |
First Approval Date United States (01 Dec 2005), |
RegulationOrphan Drug (United States), Orphan Drug (European Union), Orphan Drug (Japan), Priority Review (China) |




Login to view timeline
Structure/Sequence
Molecular FormulaC28H24ClF3N4O6S |
InChIKeyIVDHYUQIDRJSTI-UHFFFAOYSA-N |
CAS Registry475207-59-1 |
Related
885
Clinical Trials associated with Sorafenib TosylateChiCTR2600120015
Single-Center Prospective Study of Homoharringtonine Combined with Azacitidine and Venetoclax in the Treatment of Adult Patients with Newly Diagnosed Acute Myeloid Leukemia
NCT06227221
A Phase 2, Randomized, Placebo Controlled Study Investigating the Efficacy and Safety of Sorafenib in New-Onset Type 1 Diabetes Mellitus
NCT07264010
Sorafenib Combined With Venetoclax as Pre-emptive Therapy Strategy for Measurable Residual Disease Persisting Acute Myeloid Leukemia: a Prospective, Single-arm, Multicenter Clinical Study
100 Clinical Results associated with Sorafenib Tosylate
Login to view more data
100 Translational Medicine associated with Sorafenib Tosylate
Login to view more data
100 Patents (Medical) associated with Sorafenib Tosylate
Login to view more data
13,047
Literatures (Medical) associated with Sorafenib Tosylate31 Dec 2026Artificial Cells Nanomedicine and Biotechnology
The unmasking of two-faced portrait in sorafenib-resistant surroundings via systems pharmacology concept: a brightness or a silhouette
Article
Author: Kim, Dong Joon ; Oh, Ki-Kwang ; Suk, Ki-Tae ; Lee, Kyeong Jin ; Eom, Jung-A ; Kwon, Goo-Hyun
This study aimed to identify novel key targets and mechanisms for repurposing strategies and mitigating sorafenib (SFB) resistance using the GEO transcriptomic dataset GSE94550 within a systems pharmacology framework. Potential counteracting molecules against SFB were retrieved from chemical repositories, followed by molecular docking tests (MDT), Kaplan-Meier survival analysis, and density functional theory (DFT) assessments to evaluate therapeutic potential. PPI networks were constructed using STRING and R to characterize the relationships between upregulated and downregulated genes. The most relevant signalling pathways associated with major targets were determined to elucidate the upstream regulatory mechanisms. Among the differentially expressed genes, APOB emerged as a pivotal regulator (log2FC ≥ +2 or ≤ -2), modulating fifteen genes, including eleven upregulated and four downregulated nodes. At stricter thresholds (log2FC ≥ +3 or ≤ -3 and ≥ +4 or ≤ -4), CD44 was identified as a key upregulated target. Its inhibition - particularly by verbacoside - was strongly associated with suppression of the ECM-receptor interaction pathway, suggesting a significant therapeutic axis. This study illuminates the molecular landscape of SFB-resistant environments through an integrative network approach and highlights verbacoside as a promising agent capable of attenuating SFB resistance, supporting its potential role in combination therapy.
31 Dec 2026JOURNAL OF MEDICAL ECONOMICS
Cost-effectiveness analysis of atezolizumab and bevacizumab as first-line systemic therapy in unresectable hepatocellular carcinoma in Malaysia
Article
Author: Chaiyakunapruk, Nathorn ; Patikorn, Chanthawat ; Sulaiman Shah, Audi Adawiah ; Wong, Yoke Fui ; Mohamed, Rosmawati
AIM:
This study aims to evaluate the cost-effectiveness of atezolizumab plus bevacizumab as first-line systemic therapy for unresectable hepatocellular carcinoma (uHCC) in Malaysia, compared with the current standard treatments in the Malaysian Ministry of Health (MOH) to inform public healthcare decision‑making.
MATERIALS AND METHODS:
A cost-effectiveness analysis was conducted from the MOH perspective, following the national pharmacoeconomic guidelines (2019). The study compared atezolizumab plus bevacizumab with sorafenib and lenvatinib, respectively, using a partitioned survival model to project health outcomes and costs over a lifetime horizon. Clinical efficacy data were sourced from published trials and network meta-analyses. Cost inputs reflected local healthcare resource use and prices, using 2024 Malaysian Ringgit values inflated via the Consumer Price Index for Health. Costs and outcomes were discounted at 3% annually. Deterministic and probabilistic sensitivity analyses were performed to assess the impact of key parameter uncertainties on the results.
RESULTS:
Atezolizumab plus bevacizumab provided the highest quality-adjusted life years (QALYs) and life years compared to sorafenib and lenvatinib. Sorafenib was dominated by lenvatinib due to lower QALYs and higher costs and excluded from further analysis. Compared to lenvatinib, atezolizumab plus bevacizumab yielded 0.873 additional QALYs and RM 44,863 additional cost, resulting in an incremental cost-effectiveness ratio (ICER) of RM 51,399 per QALY gained (∼0.906 GDP/capita at Malaysia's 2024 GDP/capita RM 56,734).
CONCLUSIONS:
Atezolizumab plus bevacizumab is cost-effective compared to lenvatinib and sorafenib across willingness-to-pay (WTP) values of one to three times Malaysia's GDP per capita. These findings provide evidence to inform public health policy that expanding funding and adoption of atezolizumab plus bevacizumab is likely to improve health outcomes cost-effectively.
31 Dec 2026ANNALS OF MEDICINE
Molecular targeted therapy in combination with chemotherapy for the treatment of platinum-resistant/refractory ovarian cancer (PROC): a systematic review and network meta-analysis
Review
Author: E., Shaolong ; Ying, Tianshu ; Ying, Huanchun
BACKGROUND:
Although single-agent chemotherapy is the most common approach for treating platinum-resistant or refractory ovarian cancer (PROC), there is growing evidence that combining molecular targeted agents with chemotherapy is beneficial, especially for certain patient groups. However, the most effective combination regimen remains elusive.
OBJECTIVES:
This Bayesian network meta-analysis (NMA) aims to identify the best combination therapy for PROC.
METHODS:
Relevant studies were searched in PubMed, EMBASE, Web of Science and the Cochrane Central Register of Controlled Trials from their inception until October 2024. The primary outcomes were overall survival (OS), progression-free survival (PFS) and adverse events (AEs). Statistical analyses were performed using the GEMTC package (1.0-2) and R 4.2.0. This review was registered in PROSPERO (CRD42023428414).
RESULTS:
Our analysis of 22 randomized controlled trials (RCTs) (n = 3408) demonstrated that chemotherapy combinations with bevacizumab (hazard ratio (HR) = 0.52-0.65), sorafenib (HR = 0.65, 95% confidence interval (CI): 0.45-0.93) or adavosertib (HR = 0.56, 95%CI: 0.35-0.90) significantly improved OS and PFS versus chemotherapy alone. Notably, adavosertib + gemcitabine was associated with an increased risk of grade 3-4 AEs (relative risk (RR) = 1.8, 95%CI: 1.3-2.7), but these were generally manageable.
CONCLUSIONS:
Bevacizumab-based combinations demonstrate consistent benefits across multiple regimens for PROC. Paclitaxel + bevacizumab emerges as the optimal balance of efficacy and safety. Topotecan + sorafenib could be an alternative for patients who are ineligible for anti-angiogenic therapy.
515
News (Medical) associated with Sorafenib Tosylate14 Jul 2026
Phase 3Clinical Result
10 Jul 2026
Clinical ResultPhase 3Drug ApprovalNDAADC
08 Jun 2026
Phase 2ImmunotherapyASCOClinical ResultCell Therapy
100 Deals associated with Sorafenib Tosylate
Login to view more data
External Link
| KEGG | Wiki | ATC | Drug Bank |
|---|---|---|---|
| D06272 | Sorafenib Tosylate |
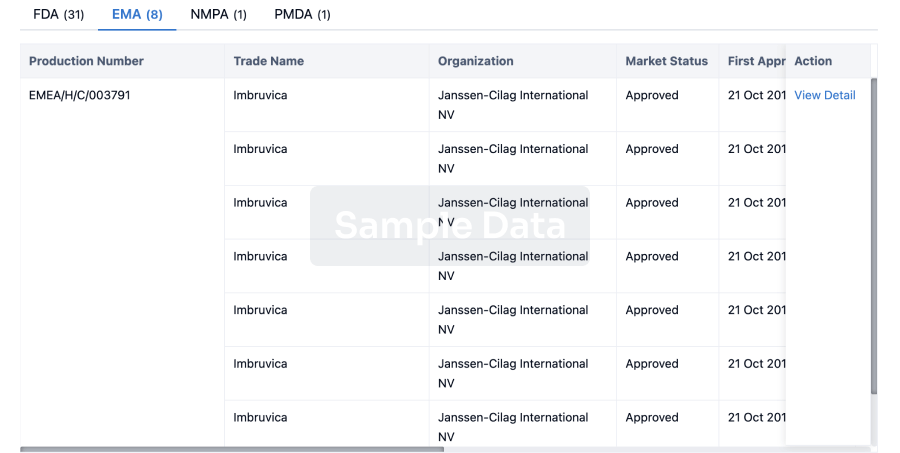
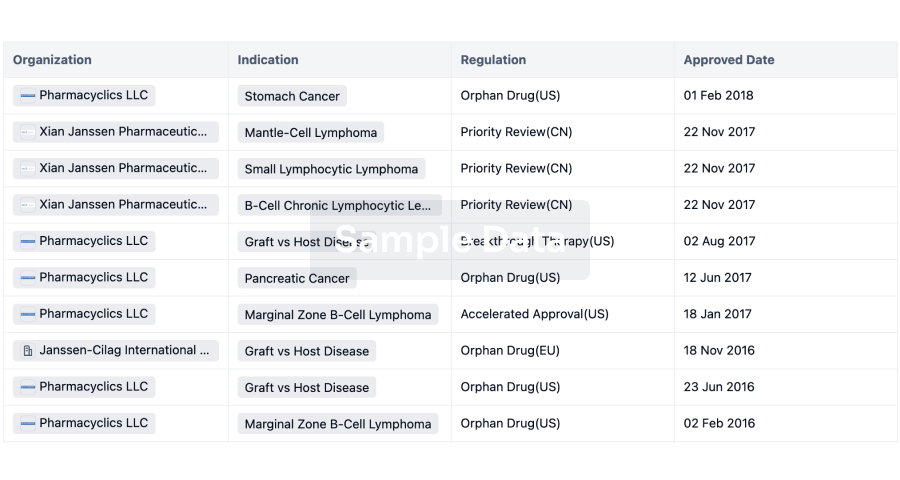
R&D Status
Approved
10 top approved records. to view more data
Login
| Indication | Country/Location | Organization | Date |
|---|---|---|---|
| Thyroid Cancer | United States | 22 Nov 2013 | |
| Unresectable Hepatocellular Carcinoma | United States | 16 Nov 2007 | |
| Advanced Hepatocellular Carcinoma | Australia | 27 Sep 2006 | |
| Differentiated Thyroid Gland Carcinoma | European Union | 19 Jul 2006 | |
| Differentiated Thyroid Gland Carcinoma | Iceland | 19 Jul 2006 | |
| Differentiated Thyroid Gland Carcinoma | Liechtenstein | 19 Jul 2006 | |
| Differentiated Thyroid Gland Carcinoma | Norway | 19 Jul 2006 | |
| Hepatocellular Carcinoma | European Union | 19 Jul 2006 | |
| Hepatocellular Carcinoma | Iceland | 19 Jul 2006 | |
| Hepatocellular Carcinoma | Liechtenstein | 19 Jul 2006 | |
| Hepatocellular Carcinoma | Norway | 19 Jul 2006 | |
| Renal Cell Carcinoma | European Union | 19 Jul 2006 | |
| Renal Cell Carcinoma | Iceland | 19 Jul 2006 | |
| Renal Cell Carcinoma | Liechtenstein | 19 Jul 2006 | |
| Renal Cell Carcinoma | Norway | 19 Jul 2006 | |
| Advanced Renal Cell Carcinoma | United States | 01 Dec 2005 |

Developing
10 top R&D records. to view more data
Login
| Indication | Highest Phase | Country/Location | Organization | Date |
|---|---|---|---|---|
| Acute Myeloid Leukemia with FLT3/ITD Mutation | Phase 3 | China | 20 Jun 2015 | |
| HER2-negative breast cancer | Phase 3 | United States | 21 Feb 2011 | |
| HER2-negative breast cancer | Phase 3 | United States | 21 Feb 2011 | |
| HER2-negative breast cancer | Phase 3 | China | 21 Feb 2011 | |
| HER2-negative breast cancer | Phase 3 | China | 21 Feb 2011 | |
| HER2-negative breast cancer | Phase 3 | Japan | 21 Feb 2011 | |
| HER2-negative breast cancer | Phase 3 | Japan | 21 Feb 2011 | |
| HER2-negative breast cancer | Phase 3 | Argentina | 21 Feb 2011 | |
| HER2-negative breast cancer | Phase 3 | Argentina | 21 Feb 2011 | |
| HER2-negative breast cancer | Phase 3 | Australia | 21 Feb 2011 |
Login to view more data
Clinical Result
Clinical Result
Indication
Phase
Evaluation
View All Results
Phase 2 | 16 | lhnryqifve(fxszotzied) = zapfakdfaz voqeibalpl (mfcmykfsmj ) View more | Negative | 01 May 2026 | |||
Phase 2 | 10 | xltgfelgqv = bkrlywjuuq xotzhqmtyd (xkgguklsbg, msoukqqtxz - zxggytmxza) View more | - | 30 Mar 2026 | |||
Phase 1 | 10 | Sorafenib plus selective internal radiotherapy with 90Y resin microspheres | ombmeskhub(nonuasdkse) = The most common grade 2-4 adverse events included rash, abdominal pain, fatigue and lymphocytopenia. yqnnqbspdv (iahznvdehm ) | Negative | 20 Feb 2026 | ||
Phase 2 | KRAS Mutant Pancreatic Cancer KRAS mutations | 9 | xgxtxtfpdw(sdsemxkelp) = gpjaswwssn zrmendodjq (brlezlhash ) View more | Negative | 10 Feb 2026 | ||
Not Applicable | Unresectable Hepatocellular Carcinoma First line | 167 | yrfalqidhq(cxnupgkcou) = zritbnwzxk fziantazte (dicgclkamw ) View more | Positive | 08 Jan 2026 | ||
yrfalqidhq(cxnupgkcou) = xwrwarbxyw fziantazte (dicgclkamw ) View more | |||||||
Not Applicable | 48 | CLIA + Gilteritinib | balclxcndf(jsykgpsiio) = 17 cases for CLIA/gilt llfgcckzks (dcuusttjqi ) View more | Positive | 06 Dec 2025 | ||
CLIA + Sorafenib | |||||||
Phase 2 | 71 | prnrdjxqal(dovxneyaqq) = wvghjkvigs pqpcixajpy (pikczvhuzh ) View more | Positive | 06 Dec 2025 | |||
Standard chemotherapy | prnrdjxqal(dovxneyaqq) = mhtudywndj pqpcixajpy (pikczvhuzh ) View more | ||||||
Not Applicable | Unresectable Hepatocellular Carcinoma First line | 3,222 | tdfjwjixjm(cmzccvhbws): HR = 0.98 (95.0% CI, 0.24 - 4.1) | Positive | 05 Dec 2025 | ||
Phase 2 | 78 | wzgocuqlvk(mdclwyttcy) = exxjyfjobs preojrvdtd (gxgbrsesbb ) | Positive | 01 Dec 2025 | |||
Placebo | wzgocuqlvk(mdclwyttcy) = dtysyfynnz preojrvdtd (gxgbrsesbb ) | ||||||
Not Applicable | 16 | allwyzylew(zaontupxfj) = Enrichment of immunosuppressive CD14+ monocytes were observed in patients with HCC and CPB but not CPA liver disease. twlrkaedcn (cvsunzoaqt ) | Positive | 05 Nov 2025 |
Login to view more data
Translational Medicine
Boost your research with our translational medicine data.
login
or

Deal
Boost your decision using our deal data.
login
or

Core Patent
Boost your research with our Core Patent data.
login
or

Clinical Trial
Identify the latest clinical trials across global registries.
login
or

Approval
Accelerate your research with the latest regulatory approval information.
login
or
Regulation
Understand key drug designations in just a few clicks with Synapse.
login
or
Hiro LS Researcher
The AI Search Engine Built to Accelerate Biopharma Decisions
Search across billion-scale life sciences data to uncover signals, validate evidence, and act with confidence.
Ask any biopharma research question→
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, Patsnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Discover Synapse Data Servers
Synapse data is now integrated into the PatSnap LS Model Context Protocol (MCP) service. Customize your LLM agent now using our MCP server!
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free