Request Demo
What is Morphine Sulfate used for?
15 June 2024
Morphine sulfate, a potent opioid analgesic, has been a cornerstone in pain management for centuries. Derived from the opium poppy plant, it's known by various trade names including MS Contin, Kadian, and Avinza, among others. It targets the central nervous system (CNS) and binds to the mu-opioid receptors, providing relief from moderate to severe pain. Research institutions worldwide have extensively studied morphine sulfate to understand its pharmacodynamics, pharmacokinetics, and potential therapeutic benefits. It is mainly indicated for pain relief in conditions such as severe injury, post-surgical pain, cancer-related pain, and chronic pain unresponsive to non-opioid analgesics. The research progress on morphine sulfate continues to evolve, with ongoing studies focusing on improving its efficacy, reducing its side effects, and finding ways to mitigate the risk of addiction.
Morphine sulfate exerts its effects by binding to and activating the mu-opioid receptors in the brain and spinal cord. These receptors are part of the endogenous opioid system, which regulates pain, reward, and addictive behaviors. When morphine sulfate binds to these receptors, it inhibits the release of neurotransmitters like substance P and glutamate, which are involved in pain transmission. This leads to a reduction in the perception of pain and an increase in pain tolerance.
Additionally, morphine sulfate induces euphoria by stimulating the release of dopamine in the brain's reward pathways. However, this same mechanism also underlies its potential for abuse and addiction. Prolonged use of morphine sulfate can lead to tolerance, requiring higher doses to achieve the same analgesic effect, and dependence, characterized by withdrawal symptoms upon cessation.
Morphine sulfate can be administered through various routes, including oral, intravenous (IV), intramuscular (IM), subcutaneous (SC), and rectal. The method of administration often depends on the patient's condition, the severity of pain, and the required speed of relief. Oral formulations, such as tablets and capsules, are commonly used for chronic pain management. These can be immediate-release (IR) or extended-release (ER) forms. IR forms typically provide pain relief within 30 to 60 minutes, with effects lasting 3 to 4 hours. In contrast, ER forms provide sustained pain relief over 12 to 24 hours.
IV administration is used for rapid pain relief, often in acute settings like post-surgical or trauma care. The onset of action is almost immediate, within minutes, making it highly effective for severe pain. IM and SC routes are alternative options when IV access is not available or practical, with onset times of 10 to 30 minutes and durations of action similar to IV administration. Rectal administration is less common but can be useful in specific scenarios where other routes are not viable.
Despite its efficacy, morphine sulfate is associated with a range of side effects. Common side effects include constipation, nausea, vomiting, dizziness, drowsiness, and sweating. These effects are generally manageable with supportive care and dose adjustments. However, more severe side effects can occur, including respiratory depression, hypotension, bradycardia, and severe allergic reactions. Respiratory depression is particularly concerning, as it can be life-threatening. Therefore, patients receiving morphine sulfate should be closely monitored, especially during the initial phases of treatment or following dose increases.
Morphine sulfate is contraindicated in patients with known hypersensitivity to the drug, respiratory conditions like severe asthma or chronic obstructive pulmonary disease (COPD), and gastrointestinal obstruction. It should be used with caution in patients with head injuries, liver or kidney impairment, and a history of substance abuse. Additionally, pregnant and breastfeeding women should avoid morphine sulfate due to potential risks to the fetus or infant.
Morphine sulfate can interact with several other drugs, potentially altering its effects or increasing the risk of adverse reactions. Central nervous system depressants, such as benzodiazepines, other opioids, alcohol, and certain antihistamines, can enhance the sedative and respiratory depressant effects of morphine sulfate. This combination can be particularly dangerous and should be avoided or used with extreme caution under medical supervision.
Certain medications, like monoamine oxidase inhibitors (MAOIs), can also interact with morphine sulfate, leading to severe and unpredictable reactions. MAOIs should be discontinued at least two weeks before initiating morphine sulfate treatment. Other drugs that may affect morphine sulfate's metabolism include enzyme inducers like rifampin and phenytoin, which can reduce its efficacy, and enzyme inhibitors like fluoxetine and paroxetine, which can increase the risk of side effects.
In conclusion, morphine sulfate remains a vital tool in the management of severe pain, offering significant relief to patients when used appropriately. However, its use requires careful consideration of its side effects, potential for addiction, and interactions with other medications. Ongoing research aims to optimize its use and find ways to mitigate its risks, ensuring that patients can benefit from its powerful analgesic properties while minimizing harm. As with any potent medication, healthcare providers must balance the benefits and risks, tailoring treatment to each patient's unique needs and circumstances.
Morphine sulfate exerts its effects by binding to and activating the mu-opioid receptors in the brain and spinal cord. These receptors are part of the endogenous opioid system, which regulates pain, reward, and addictive behaviors. When morphine sulfate binds to these receptors, it inhibits the release of neurotransmitters like substance P and glutamate, which are involved in pain transmission. This leads to a reduction in the perception of pain and an increase in pain tolerance.
Additionally, morphine sulfate induces euphoria by stimulating the release of dopamine in the brain's reward pathways. However, this same mechanism also underlies its potential for abuse and addiction. Prolonged use of morphine sulfate can lead to tolerance, requiring higher doses to achieve the same analgesic effect, and dependence, characterized by withdrawal symptoms upon cessation.
Morphine sulfate can be administered through various routes, including oral, intravenous (IV), intramuscular (IM), subcutaneous (SC), and rectal. The method of administration often depends on the patient's condition, the severity of pain, and the required speed of relief. Oral formulations, such as tablets and capsules, are commonly used for chronic pain management. These can be immediate-release (IR) or extended-release (ER) forms. IR forms typically provide pain relief within 30 to 60 minutes, with effects lasting 3 to 4 hours. In contrast, ER forms provide sustained pain relief over 12 to 24 hours.
IV administration is used for rapid pain relief, often in acute settings like post-surgical or trauma care. The onset of action is almost immediate, within minutes, making it highly effective for severe pain. IM and SC routes are alternative options when IV access is not available or practical, with onset times of 10 to 30 minutes and durations of action similar to IV administration. Rectal administration is less common but can be useful in specific scenarios where other routes are not viable.
Despite its efficacy, morphine sulfate is associated with a range of side effects. Common side effects include constipation, nausea, vomiting, dizziness, drowsiness, and sweating. These effects are generally manageable with supportive care and dose adjustments. However, more severe side effects can occur, including respiratory depression, hypotension, bradycardia, and severe allergic reactions. Respiratory depression is particularly concerning, as it can be life-threatening. Therefore, patients receiving morphine sulfate should be closely monitored, especially during the initial phases of treatment or following dose increases.
Morphine sulfate is contraindicated in patients with known hypersensitivity to the drug, respiratory conditions like severe asthma or chronic obstructive pulmonary disease (COPD), and gastrointestinal obstruction. It should be used with caution in patients with head injuries, liver or kidney impairment, and a history of substance abuse. Additionally, pregnant and breastfeeding women should avoid morphine sulfate due to potential risks to the fetus or infant.
Morphine sulfate can interact with several other drugs, potentially altering its effects or increasing the risk of adverse reactions. Central nervous system depressants, such as benzodiazepines, other opioids, alcohol, and certain antihistamines, can enhance the sedative and respiratory depressant effects of morphine sulfate. This combination can be particularly dangerous and should be avoided or used with extreme caution under medical supervision.
Certain medications, like monoamine oxidase inhibitors (MAOIs), can also interact with morphine sulfate, leading to severe and unpredictable reactions. MAOIs should be discontinued at least two weeks before initiating morphine sulfate treatment. Other drugs that may affect morphine sulfate's metabolism include enzyme inducers like rifampin and phenytoin, which can reduce its efficacy, and enzyme inhibitors like fluoxetine and paroxetine, which can increase the risk of side effects.
In conclusion, morphine sulfate remains a vital tool in the management of severe pain, offering significant relief to patients when used appropriately. However, its use requires careful consideration of its side effects, potential for addiction, and interactions with other medications. Ongoing research aims to optimize its use and find ways to mitigate its risks, ensuring that patients can benefit from its powerful analgesic properties while minimizing harm. As with any potent medication, healthcare providers must balance the benefits and risks, tailoring treatment to each patient's unique needs and circumstances.
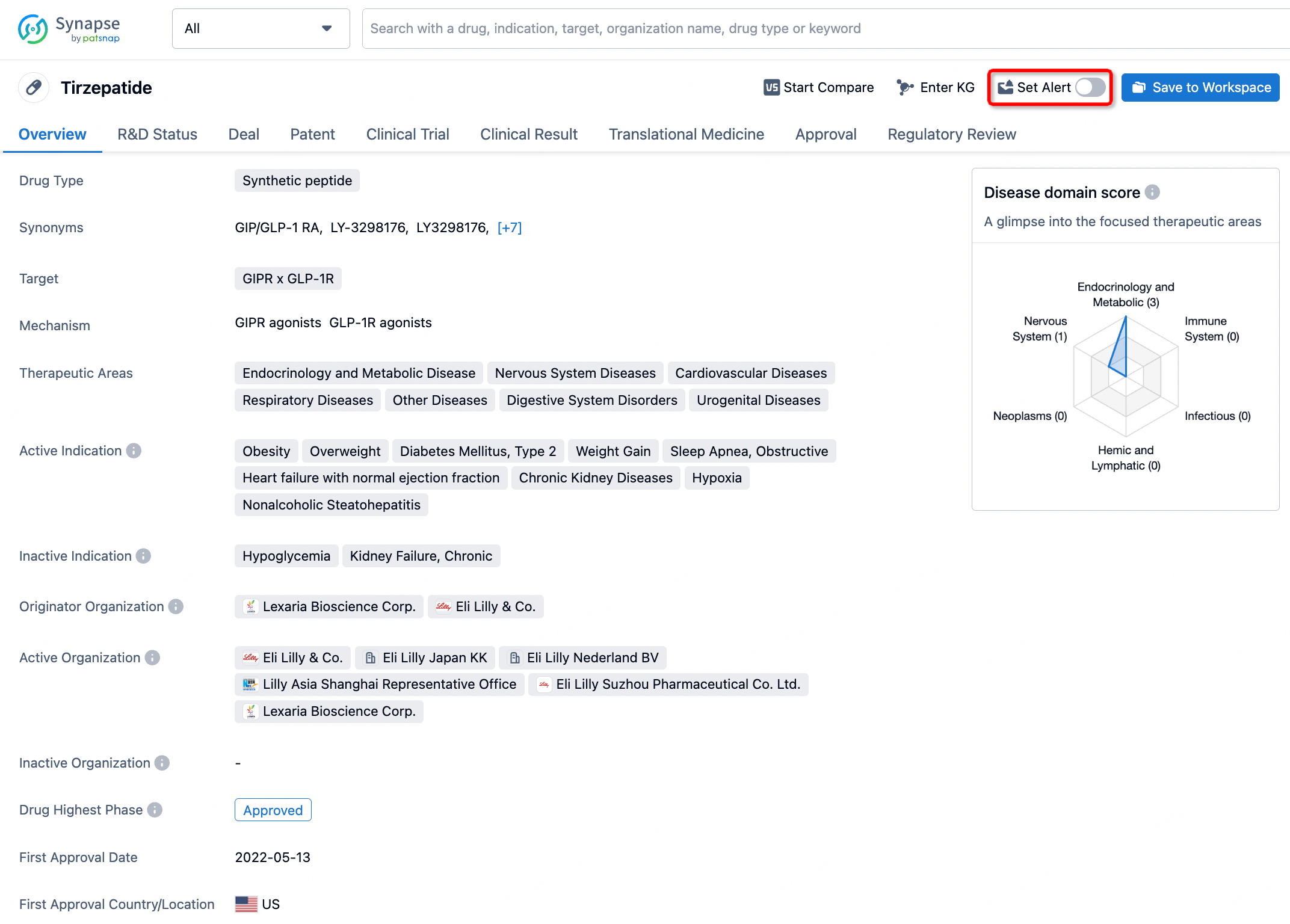
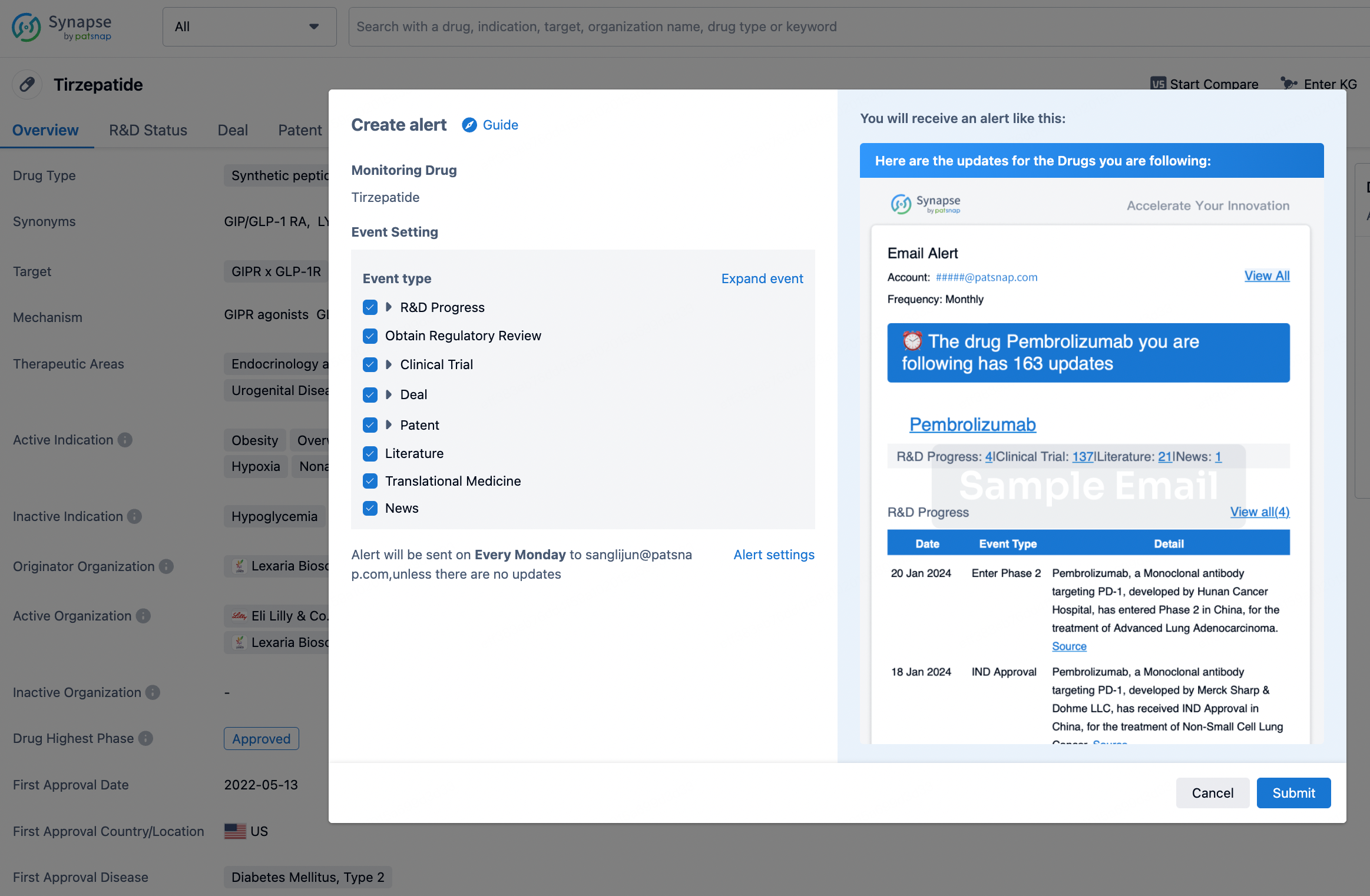
How to obtain the latest development progress of all drugs?
In the Synapse database, you can stay updated on the latest research and development advances of all drugs. This service is accessible anytime and anywhere, with updates available daily or weekly. Use the "Set Alert" function to stay informed. Click on the image below to embark on a brand new journey of drug discovery!
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.